Comparative Effects of Dynamic
Neuromuscular Stabilization and
Abdominal Drawing-in Maneuver on
Anticipatory Postural Adjustment During
Rapid Shoulder Flexion Task in Individuals
With Chronic Stroke
The Graduate School
Yonsei University
Department of Physical Therapy
Namgi Lee
Comparative Effects of Dynamic
Neuromuscular Stabilization and
Abdominal Drawing-in Maneuver on
Anticipatory Postural Adjustment During
Rapid Shoulder Flexion Task in Individuals
With Chronic Stroke
Namgi Lee
A Dissertation
Submitted to the Department of Physical Therapy
and the Graduate School of Yonsei University
in partial fulfillment of the
requirements for the degree of
Doctor of Philosophy
This certifies that the doctoral dissertation of
Namgi Lee is approved.
The Graduate School
Yonsei University
Thesis Supervisor: Sunghyun You
Chunghwi Yi: Thesis Committee Member #1
Hyeseon Jeon: Thesis Committee Member #2
Bongsam Choi: Thesis Committee Member #3
Acknowledgements
I am very grateful to everyone who has helped me finish my doctoral program. First, I would like to express my thanks to Professor Sunghyun You. He has taught me many things over the seven years. I had no knowledge of projects and papers, and his expertise has been invaluable in helping me develop my capability. I have completed graduate school, but would like to continue studying in this area with Professor You because there is so much more to learn. I would also like to thank Professor Chunghwi Yi for helping me through the process of designing my thesis. I have also been moved by Professor Hyeseon Jeon‟s love for her graduate students. I have seen and appreciated her efforts to grasp and solve her students‟ difficulties. I have learned so much about my major and how to excel in class from Professor Ohyun Kwon, and gaining this knowledge has made me very happy. Professor Sanghyun‟s words were of great encouragement to me when I had difficulties in graduate school, and Professor Heonseok Cynn has always provided pleasant support. I have learned so much from Professor Cynn‟s teaching style and his way of understanding students.
I would also like to express my gratitude to the graduate students in our laboratory and the lab members who have already graduated. The encouragement and support I received from Dongryul Lee and Jaejin Lee, in particular, helped me meet the challenges of graduate school life and perfect the process of writing my thesis.
Thanks to them, I enjoyed my graduate school life, and I hope that we will continue to collaborate in the future. Dongkoog Noh was a great inspiration to me, as we motivated each other while preparing our doctoral theses at around the same time. I would also like to thank Jiho Park, who helped me adjust to graduate school life by providing much-needed information. I also extend my thanks to Dohyeon Kim, Jiwon Yoo and other graduate students too numerous to name for encouraging and supporting me.
In particular, I extend my heartfelt gratitude to Professor Bongsam Choi for becoming an assistant judge of my thesis despite a very busy schedule. Professor Choi was very considerate in his role as my boss at Woosong University, and his support was instrumental in my graduate work. I am also very thankful to Jungah Lee, my lovely mentor, for supporting me. I heartily thank Intae Ryu and Jaeman Park at the Daejeon Rehabilitation Center for helping me finish my doctoral thesis experiment. I will never forget their devoted assistance.
Finally, I must thank my lovely family (my parents, husband, daughter, elder sister, and elder brother). I could not have finished my doctoral thesis without the support of my husband, Taeheon Lee. I apologize to my daughter, Heejin Lee, for taking so much time away from her to complete the experiment, and I thank her for growing so well despite my absence. While writing my doctoral thesis, I continually thanked God for giving me such a precious life to match my birth name, „Luckluck‟. I wish health, happiness and full lives for all of my family and friends.
Table of Contents
List of Figures ··· iii
List of Tables ··· iv Abstract ··· v Introduction ··· 1 Methods ··· 6 1. Subjects ··· 6 2. Instrumentation ··· 9 2.1 Surface Electromyography ··· 9 2.2 Real-time Ultrasound ··· 9 3. Experimental Procedures ··· 10 3.1 Experimental Testing ··· 12
3.1.1 Surface EMG for Measuring Onset Latency ··· 14
3.2 Intervention ··· 15
3.2.1 Real-time US for Monitoring Diaphragm Movement and Contraction of the Lateral Abdominal Muscles ··· 19
4. Data Analysis ··· 20
5. Statistical Analysis ··· 21
Results ··· 22
2. Pre-test and Post-test Onset Latency (ms) in the ADIM Group ··· 25
3. Onset Latency (ms) between the DNS and ADIM Groups ··· 28
Discussion ··· 31
Conclusion ··· 35
References ··· 36
List of Figures
Figure 1. Neuromechanical core stabilization force produced by an abdominal drawing-in maneuver and by dynamic neuromuscular
stabilization ··· 4
Figure 2. Experimental procedures ··· 11
Figure 3. Rapid shoulder flexion task ··· 13
Figure 4. Postures and extremity movements for intervention ··· 17
Figure 5. Visual feedback using real-time ultrasound imaging ··· 18
Figure 6. Comparison of pre-test and post-test onset latency (ms) in the DNS group ··· 24
Figure 7. Comparison of pre-test and post-test onset latency (ms) in the ADIM group ··· 27
Figure 8. Comparison of onset latency (ms) between the DNS and ADIM groups ··· 30
List of Tables
Table 1. Demographic and clinical characteristics of the subjects ··· 8 Table 2. Comparison of pre-test and post-test onset latency (ms) in the
DNS group ··· 23 Table 3. Comparison of pre-test and post-test onset latency (ms) in the
ADIM group ··· 26 Table 4. Comparison of onset latency between the DNS and ADIM groups
ABSTRACT
Comparative Effects of Dynamic Neuromuscular
Stabilization and Abdominal Drawing-in Maneuver on
Anticipatory Postural Adjustment During Rapid Shoulder
Flexion Task in Individuals With Chronic Stroke
Namgi Lee
Dept. of Physical Therapy The Graduate School Yonsei University
The purpose of this study was to compare the effects of dynamic neuromuscular stabilization (DNS) and abdominal drawing-in maneuver (ADIM) exercises on anticipatory postural adjustment (APA) in individuals with chronic hemiparetic stroke. Twenty-eight adults with chronic hemiparetic stroke (15 males, 13 females; mean age ± standard deviation, 57.7 ± 8.5 years) were enrolled in this study. The subjects were randomly divided into the DNS (n = 14) and ADIM (n = 14) groups. Each of the DNS and ADIM exercises was performed for 30minutes per day, 5 days a week for 4 weeks. The APA was determined by measuring the electromyographic (EMG) onset latency
in external oblique (EO), transvers abdominis/internal oblique (TrA/IO), and erector spinae (ES) muscles during rapid shoulder flexion. Paired t-tests were used to compare the EMG onset latency between pre-test and post-test in the respective DNS and ADIM groups. Analysis of covariance (ANCOVA) was used to evaluate the differences between the adjusted means of post-test for the DNS and ADIM intervention groups while controlling for the covariates (pre-test). The level of significance was set at α = 0.05. In the DNS group, paired t-tests revealed significant differences in onset latencies for the EO and TrA/IO muscles between pre-test and post-test. In the ADIM group, paired t-test revealed a significant difference in onset latency for the TrA/IO muscles between pre-test and post-test. A separate ANCOVA showed significant differences in the adjusted mean onset latencies between groups during either the paretic or nonparetic shoulder flexion for the paretic and nonparetic postural trunk muscles (EO, TrA/IO, and ES), with exception of the nonparetic ES muscle during paretic shoulder flexion. Therefore, the results of this study suggest that DNS training was more effective than ADIM training in improving APA via the feedforward activation of postural trunk muscles in individuals with hemiparetic stroke.
Key Words: Abdominal drawing-in maneuver, Anticipatory postural adjustment, Chronic stroke, Dynamic neuromuscular stabilization.
Introduction
Anticipatory postural adjustment (APA) dysfunction is a common neuromuscular impairment in hemiparetic stroke, which is often associated with dynamic balance disorder (Aruin 2002). APA involves the feedforward mechanism where postural core muscles stabilize the spine against the internal and external perturbation forces imposed on the body segment during voluntary limb movements (Cordo, and Nashner 1982; Hodges, and Richardson 1997). APA is characterized as a “subconscious” preactivation of postural core muscles, particularly the transverse abdominis (TrA) (Aruin, and Latash 1995; Hodges, and Richardson 1999; Hodges, and Richardson 1997) and the diaphragm muscles (Kolar et al. 2012) before either shoulder or hip movement in healthy adults. In cases of pathological hemiparetic stroke, APA muscular activity is impaired, mainly on the paretic side (Bennis et al. 1996; Garland, Stevenson, and Ivanova 1997). Electromyographic (EMG) studies on APA have shown the delayed onset activation of the ipsilateral erector spinae (ES), latissimus dorsi (LD), and lower trapezius muscles during paretic and nonparetic arm flexion tasks (Dickstein et al. 2004; Pereira et al. 2014). Perhaps a postural core stabilization exercise that emphasizes the selective preactivation of the TrA and diaphragm muscles via the feedforward control mechanism would help individuals with hemiparetic stroke to achieve normalized APA patterns. Identifying the changes in the neuromotor control mechanisms underlying postural stabilization impairments could
also direct future interventions and integrate important clinical concepts into the development of novel and effective intervention.
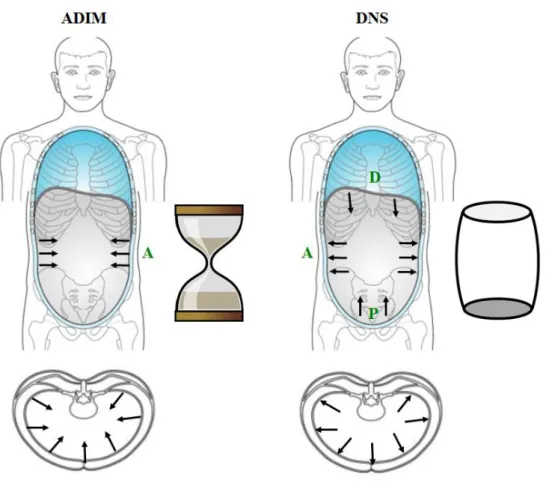
Contemporary postural core stabilization techniques including the abdominal drawing-in maneuver (ADIM) and dynamic neuromuscular stabilization (DNS), have been used to improve the postural stability and associated balance performance in individuals with stroke (Lim et al. 2012) or to enhance the APA activity of the TrA muscle in individuals with low back pain (LBP) (Tsao, and Hodges 2007). The ADIM involves a conscious feedback mechanism that improves postural stabilization through the selective activation of the TrA and the internal oblique (IO) muscles, combined with minimal contraction of other superficial abdominal (external oblique; EO) and paraspinal muscles. The method uses a real-time visual feedback about muscle size and pressure changes obtained from ultrasound (US) imaging and pressure biofeedback unit, respectively (Anderson Worth, Henry, and Bunn 2007; Henry, and Westervelt 2005; Hides et al. 2006; O‟Sullivan, Twomey, and Allison 1998). In essence, the concentric co-contraction of the TrA and the IO muscles creates a “sandglass-like stabilization cylinder” by increasing the tension of the thoracolumbar fascia (TLF) in relation to the TrA and IO muscles (Hodges, and Richardson 1999). This sandglass-like stabilization can increase the intra-abdominal pressure (IAP), allowing a localized lumbar segmental stability rather than overall postural stabilization. However, the sandglass-like stabilization limits natural descending movement of diaphragm, which affects normal breathing.
“postural stabilization cylinder belt (PSCB)” (comprising the diaphragm, TrA/IO, pelvic floor muscles, and the superficial abdominal and chest wall muscles) is synergistically orchestrated to create optimal IAP. This IAP provides overall postural stability in response to internal or external perturbation during dynamic limb movement (Frank, Kobesova A, and Kolar 2013). During inspiration, the diaphragm concentrically contracts in the caudal direction subconsciously or feedforwardly creating IAP within the PSCB. The increased IAP concurrently activates deep pelvic floor muscles (also known as a „pelvic diaphragm‟) to provide inferior stabilization and eccentrically contracts abdominal muscles to provide anterolateral stability and posterior stability to the spine, thereby improving overall postural stability (Chaitow, Bradley, and Gilbert 2014).
Figure 1. Neuromechanical core stabilization force produced by an abdominal drawing-in maneuver (ADIM) and by dynamic neuromuscular stabilization (DNS) (Modified illustration from Chaitow, Bradley, and Gilbert 2014).
(A: Direction of force on abdominal muscles; D: Direction of force on the diaphragm muscle; P: Direction of force on pelvic floor muscles.)
Despite the important contribution of the TrA on APA, it remains unclear whether its onset activation time is delayed during dynamic voluntary movements in individuals with hemiparetic stroke. Clinical and therapeutic effects of contemporary core stabilization techniques are relatively well established for the musculoskeletal LBP population. Nonetheless, the effect of these techniques on optimal APA is unknown in individuals with neurological hemiparetic stroke. Therefore, the purposes of this study were twofold: (1) to examine the main effect (pre-/post-test) of individual DNS and ADIM intervention on APA and (2) to compare the effects of the postural core stabilization interventions on APA between the DNS and ADIM groups in individuals with chronic hemiparetic stroke. APA is determined by measuring EMG onset latency in the postural trunk muscles during rapid shoulder flexion. Our hypothesis is that DNS training can improve APA in individuals with chronic hemiparetic stroke via the coordinated neuromuscular activation of postural trunk muscles, and that DNS can perform this function better than the ADIM.
Method
1. Subjects
Twenty-eight adults with chronic hemiparetic stroke (15 males, 13 females; mean age ± standard deviation, 57.7 ± 8.5 years) were recruited from the Daejeon Rehabilitation Center. This experimental procedure was approved by the Woosong University, College of Health and Welfare, Institutional Review Board (2014-04). Signed consent was obtained from all of the subjects before their participation in this study.
The inclusion criteria were as follows: (1) more than six months after the clinical diagnosis of ischemic or hemorrhagic hemiparetic stroke, (2) sufficient cognitive function, as determined by a score of at least 24 out of 30 on the Korean version of the Mini-Mental State Examination (MMSE-K), (3) the ability to walk at least 10 meters independently with or without the use of a walking aid, (4) a rating of stage 4 or higher in Brunnstrom‟s stages of motor recovery, (5) a score of less than 21 out of 23 points on the trunk impairment scale (TIS), (6) a score of less than 45 on the Berg balance scale (BBS), and (7) the ability to understand and follow simple verbal instructions (Chung, Lee, and Hwang 2014).
The exclusion criteria included a history or current diagnosis of other neurological or musculoskeletal diseases, hemineglect, visual lesions or pain (Pereira et al. 2014).
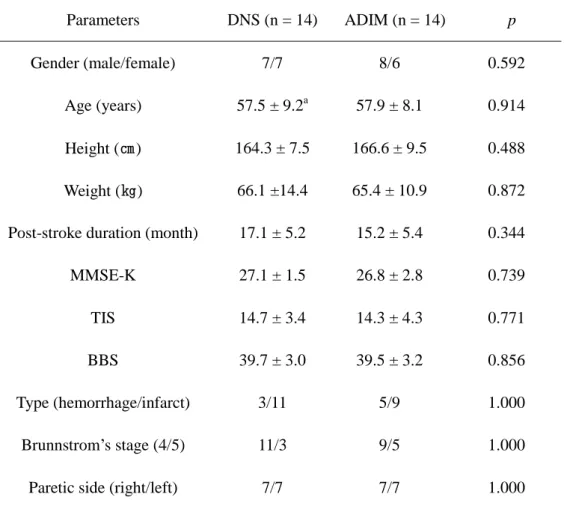
The demographic and clinical characteristics of the subjects are presented in Table 1. There were no significant differences in demographic and clinical characteristics between the DNS and ADIM groups, satisfying the homogeneity assumption (Table 1).
Table 1. Demographic and clinical characteristics of the subjects Parameters DNS (n = 14) ADIM (n = 14) p Gender (male/female) 7/7 8/6 0.592 Age (years) 57.5 ± 9.2a 57.9 ± 8.1 0.914 Height (㎝) 164.3 ± 7.5 166.6 ± 9.5 0.488 Weight (㎏) 66.1 ±14.4 65.4 ± 10.9 0.872 Post-stroke duration (month) 17.1 ± 5.2 15.2 ± 5.4 0.344 MMSE-K 27.1 ± 1.5 26.8 ± 2.8 0.739 TIS 14.7 ± 3.4 14.3 ± 4.3 0.771 BBS 39.7 ± 3.0 39.5 ± 3.2 0.856 Type (hemorrhage/infarct) 3/11 5/9 1.000 Brunnstrom‟s stage (4/5) 11/3 9/5 1.000 Paretic side (right/left) 7/7 7/7 1.000 DNS: Dynamic neuromuscular stabilization; ADIM: Abdominal drawing-in maneuver; MMSE-K: Mini-mental state examination (Korean version); TIS: Trunk impairment scale; BBS: Berg balance scale.
a
2. Instrumentation
2.1 Surface Electromyography
Surface EMG was used to measure the neuromuscular mechanism (or APA) of postural trunk control during rapid shoulder flexion. We measured the onset latency (relative to the anterior deltoid activity) of the postural trunk muscles. The EMG data were collected with a TeleMyo DTS (Noraxon Inc., Scottsdale, AZ, USA) and analyzed using MyoResearch software (Noraxon Inc., Scottsdale, AZ, USA) and Matlab R2008A (The MathWorks Inc., Natick, MA, USA).
2.2 Real-time Ultrasound
Real-time US systems (Achievo CST, V2U Co., Ltd, Singapore; MyLab25 GOLD, Esaote Co., Ltd, USA) in M-mode with 3.5 and 5 MHz curved transducers were used to provide accurate visual feedback on diaphragm and TrA muscle activation during DNS and ADIM interventions. However, the visual feedback on diaphragm activation was blinded to the subjects in the DNS group because DNS focuses on a feedforward mechanism, rather than the feedback needed for the ADIM.
3. Experimental Procedures
A procedural checklist was developed to ensure a consistent experimental protocol. Clinical tests included the MMSE-K, Brunnstrom‟s recovery stage, TIS, BBS, and a Health Screening for any medical conditions that could interfere with the experiment. Once the subjects met the inclusion and exclusion criteria, the EMG experiment was conducted to determine APA before and after the intervention. The present study used a two group pretest-posttest design. The subjects were randomly assigned to either the DNS or the ADIM group. The interventions comprised DNS and ADIM exercises that were performed for a four-week period (Figure 2). The pre-test and post-test included the measurements of changes in the EMG onset latency of the bilateral postural trunk muscles (EO, TrA/IO, and ES) during rapid shoulder flexion tasks performed while standing.
Figure 2. Experimental procedures. Group 1 Pre-test (n = 15) Group 2 Pre-test (n = 15) Dynamic neuromuscular stabilization (DNS) 4-week period Abdominal drawing-in maneuver (ADIM) 4-week period Drop out (n = 1)
After 4 weeks of training Post-test (n = 14) Random assignment
30 hemiparetic stroke patients meeting the inclusion and exclusion criteria
Drop out (n = 1)
After 4 weeks of training Post-test (n = 14)
3.1 Experimental Testing
All of the subjects underwent consistent standardized experimental testing at the pre-test and post-test. The rapid shoulder flexion task was used to create an APA response in the postural trunk muscles (Hodges, and Richardson 1997). All of the subjects maintained the standing posture quietly with their arms at their sides and their feet placed shoulder-width apart before moving their arm. Upon hearing a tone signal generated by a computer, they performed shoulder flexion to approximately 60° as fast as possible (Dickstein et al. 2004; Hodges, and Richardson 1997) and then immediately let the shoulder return to its starting position (Figure 3). All of the subjects were instructed to perform the rapid shoulder flexion without compensations such as trunk lateral flexion or extension. If any compensatory movement identified, a verbal cue was provided to mitigate it. Each trial was initiated with normal breathing and the test required an arm movement within a random period of up to 10 s after the preparation command (Dickstein et al. 2004). The intervals between trials were 10 s, and the intervals between using the paretic and nonparetic sides were about 2 minutes. All of the subjects completed 10 practice trials and data were collected for the following 10 test trials, first with the paretic and then with the nonparetic shoulder flexion tasks. Two investigators provided close supervision to ensure the safety of all of the subjects throughout the entire experiment.
3.1.1 Surface EMG for Measuring Onset Latency
During the rapid shoulder flexion task performed while standing, the surface EMG activity for each subject was recorded by wireless sensors that were 32 ㎜ (L) × 22
㎜ (W) × 15 ㎜ (H) in size (Noraxon Inc., Scottsdale, AZ, USA). The measurements were recorded from the right and left external oblique (EO), transverse abdominis/internal oblique (TrA/IO), erector spinae (ES), and anterior deltoid (AD) muscles. Before placing the surface EMG electrodes, the subject‟s skin was carefully prepared to reduce skin impedance by dry shaving any hair with a disposable razor and cleansing the skin with a 2% alcohol swab. For the EO, the electrode was placed halfway between the iliac crest and the twelfth rib at a slightly oblique angle running parallel to the muscle fibers (Cram, Kasman, and Holtz 1998). The TrA/IO electrode was located approximately 2 ㎝ medially and inferiorly from the anterior superior iliac spine (Marshall, and Murphy 2003). The ES electrode was placed on the skin over the muscle mass approximately 2 ㎝ from the lumbar (L-3) spine. Finally, for the AD, the electrode was placed on the anterior aspect of the arm at approximately 4
3.2 Intervention
For the DNS group, the standardized DNS steps were as follows: (1) A DNS certified therapist first centralized or neutralized a subject‟s sternum, ribcage, and thoracolumbar spine alignment in supine to allow normalized or natural diaphragmatic breathing. (2) The subject was then asked to maintain this centralized chest and spine alignment during the automatic descent of the diaphragm in normal inhalation, which simultaneously activates the TrA/IO. Correct DNS movement encompassed that the lower part of the sternum and the 10~12 ribs were anteriorly and laterally expanded from the medioclavicular line and posteriorly along the angulus costae like a cylinder barrel, resulting in the smooth caudal movement of the diaphragm and a widening of the intercostal spaces. This increased IAP and the associated core stabilization (Libenson 2007). The therapist inspected and palpated the subjects to ensure the correct and symmetrical movement of their chest, spine, and abdominal walls. (3) The therapist also scanned the caudal movement of the diaphragm during inspiration to ensure successful performance of DNS using a real-time US, but this information was not shared with the subjects. (4) Once the basic DNS skill as described in steps (1) – (3) was acquired in supine, then the subject progressed to a higher level of core stabilization activity including unilateral or bilateral shoulder and hip flexion-extension movement in the quadruped, sitting, and standing positions (Figure 4).
For the ADIM group, the subjects received standard verbal instructions for ADIM performance, as follows: “Pull your belly button up and in toward your spine without
pelvic movement while breathing quietly, and contract the deep abdominal muscles without excessive contraction of the superficial muscles.” The ADIM was also progressed through changes in position (supine, quadruped, sitting, or standing positions) and changes in limb movements to increase the level of difficulty. As the subjects performed this exercise, a real-time US device was used to provide visual feedback to monitor the changes in TrA/IO muscle thickness and confirm successful ADIM performance (Lee et al. 2011) (Figure 5).
The subjects in both groups sustained their DNS and ADIM performances for 10 seconds while maintaining their shoulder or hip flexion-extension. Each session consisted of 5 performances, and the subjects repeated 10 sessions with rest periods of 2 minutes between each session. All of the subjects underwent their regimes of standardized postural core stabilization exercises for 30 minutes per day, 5 days per week for 4 weeks.
3.2.1 Real-time US for Monitoring Diaphragm Movement and Contraction of the Lateral Abdominal Muscles
Real-time US was used to monitor the subjects‟ diaphragm movements during DNS training and to provide the visual feedback for ADIM training in individuals with hemiparetic stroke.
For monitoring the diaphragm movement, a real-time US with a 3.5 MHz curved transducer was used to confirm accurate performance of the DNS intervention. This second transducer was placed on the midpoint between the midclavicular and anterior axillary lines in the subcostal area, and directed medially, cranially, and dorsally (Boussuges, Gole, and Blanc 2009). The examiner could also observe the diaphragm movements in M-mode, but the subjects could not see the monitor showing these movements during their DNS exercises.
For performing ADIM accurately, a 5 MHz curved transducer was used to monitor changes in the thickness of the lateral abdominal muscles such as the TrA, IO, and EO. This transducer was placed on the anterolateral abdominal wall, lateral to the midline and halfway between the iliac crest and the inferior border of the rib cage (Richardson, Hodges, and Hides 2004). All of the subjects received visual feedback via real-time US during their ADIM training.
4. Data Analysis
The raw EMG data were collected during the „correct‟ shoulder flexion task at a sampling rate of 1000 Hz. If any compensatory movement was noted, the collected data were discarded and the test was repeated. The acquired raw EMG data were processed with a 60 Hz notch filter to reduce the noise associated with electrical interference, (including that of the 60 Hz power lines for electric or magnetic devices). The root mean-square EMG amplitude for the EO, TrA/IO, ES and AD muscles was computed, and the EMG signal was full-wave rectified and filtered using a band pass filter at 20–1000 Hz. The EMG onset time of the muscles was identified to evaluate the onset latency (or the time between the EMG onset activation of the postural trunk muscles [EO, TrA/IO, and ES] and that of the prime mover muscles [AD] during the shoulder flexion motion). The onset time was determined by a computer-based algorithm as the point at which the mean amplitude of 50 consecutive samples reached 3 standard deviations from the mean of the baseline amplitude recorded immediately before the movement stimulus (Hodges, and Richardson 1997).
5. Statistical Analysis
The descriptive statistics include the means and standard deviations. The one-sample Kolmogorov-Smirnov test was used to test for normal distribution. To assess the effects of our randomization procedure, the differences between all of the variables for the DNS and ADIM groups were evaluated by the χ2 test or the independent t-test. Paired t-tests were used to compare the EMG onset latency of each muscles between pre-test and post-test in the respective DNS and ADIM groups. An analysis of covariance (ANCOVA) was used to evaluate the difference between the adjusted means of post-test for the DNS and ADIM intervention groups while controlling for the covariate (pre-test). The level of significance was set at α = 0.05. The statistical package for the social sciences (SPSS) for Windows version 12.0 (SPSS, Chicago, IL, U.S.A) was used for statistical analysis.
Results
1. Pre-test and Post-test Onset Latency (ms) in the DNS Group
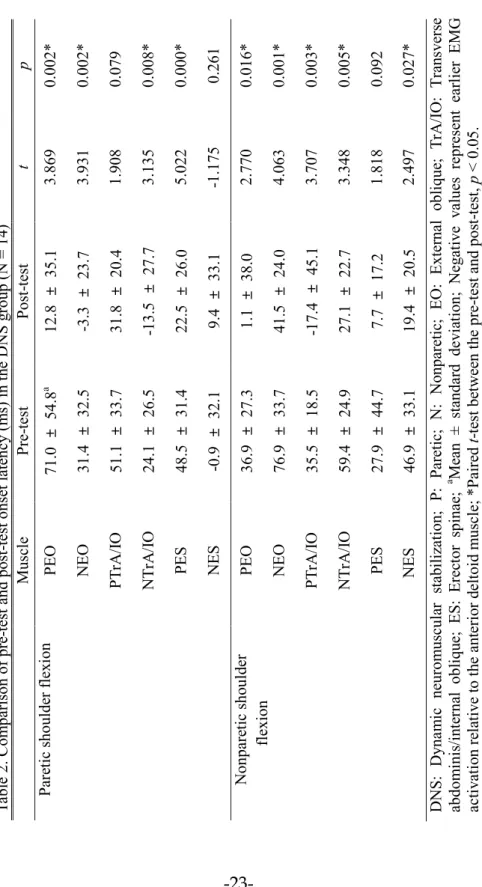
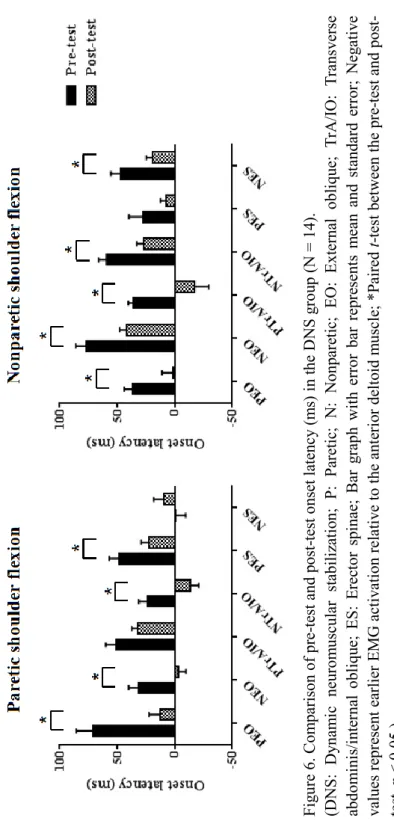
During the paretic shoulder flexion, the onset latencies for the paretic EO (p = 0.002), nonparetic EO (p = 0.002), nonparetic TrA/IO (p = 0.008), and paretic ES (p = 0.000) muscles between the pre-test and post-test decreased significantly in the DNS group. However, no significant difference was noted in the paretic TrA/IO and nonparetic ES muscle onset latencies.
During the nonparetic shoulder flexion, the onset latencies for the paretic EO (p = 0.016), nonparetic EO (p = 0.001), paretic TrA/IO (p = 0.003), nonparetic TrA/IO (p = 0.005), and nonparetic ES (p = 0.027) muscles between the pre-test and post-test decreased significantly in the DNS group. However, no significant difference was observed in the paretic ES muscle onset latency (Table 2 and Figure 6).
-23-Tabl e 2. C om par ison o f p re -te st and po st -te st onse t l at ency (m s) in t he DN S g roup (N = 14 ) D N S: D yna m ic neur om usc ul ar s tab ili zat ion; P : Par et ic ; N : N onpa ret ic ; EO : Exte rnal obl ique ; T rA /IO : T ra ns ve rse abdom ini s/ in te rna l obl iqu e; ES : E rec tor spi nae ; a M ean ± st andar d dev ia tio n; N eg at iv e val ues r epr es en t ea rlie r EMG ac tiva tion re la tiv e t o th e an ter io r d el toi d m usc le; *Pai re d t-t es t be tw ee n the p re -te st and pos t-te st, p < 0.0 5. Mus cl e Pre -tes t Post -tes t t p Par et ic shou lde r f lex ion PE O 71.0 ± 54.8 a 12.8 ± 35.1 3.869 0.002* NE O 31.4 ± 32.5 -3.3 ± 23.7 3.931 0.002* PTr A /IO 51.1 ± 33.7 31.8 ± 20.4 1.908 0.079 N Tr A /IO 24.1 ± 26.5 -13.5 ± 27.7 3.135 0.008* PES 48.5 ± 31.4 22.5 ± 26.0 5.022 0.000* NE S -0.9 ± 32.1 9.4 ± 33.1 -1.175 0.261 No npar et ic s ho ul der flex ion PE O 36.9 ± 27.3 1.1 ± 38.0 2.770 0.016* NE O 76.9 ± 33.7 41.5 ± 24.0 4.063 0.001* PTr A /IO 35.5 ± 18.5 -17.4 ± 45.1 3.707 0.003* N Tr A /IO 59.4 ± 24.9 27.1 ± 22.7 3.348 0.005* PES 27.9 ± 44.7 7.7 ± 17.2 1.818 0.092 NE S 46.9 ± 33.1 19.4 ± 20.5 2.497 0.027*
Table 2. Comparison of pre-test and post-test onset latency (ms) in the DNS group (N = 14)
DNS: Dynamic neuromuscular stabilization; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; aMean ± standard deviation; Negative values represent earlier EMG
activation relative to the anterior deltoid muscle; *Paired t-test between the pre-test and post-test, p < 0.05.
Muscle Pre-test Post-test t p Paretic shoulder flexion PEO 71.0 ± 54.8a 12.8 ± 35.1 3.869 0.002*
NEO 31.4 ± 32.5 -3.3 ± 23.7 3.931 0.002* PTrA/IO 51.1 ± 33.7 31.8 ± 20.4 1.908 0.079 NTrA/IO 24.1 ± 26.5 -13.5 ± 27.7 3.135 0.008* PES 48.5 ± 31.4 22.5 ± 26.0 5.022 0.000* NES -0.9 ± 32.1 9.4 ± 33.1 -1.175 0.261 Nonparetic shoulder flexion PEO 36.9 ± 27.3 1.1 ± 38.0 2.770 0.016* NEO 76.9 ± 33.7 41.5 ± 24.0 4.063 0.001* PTrA/IO 35.5 ± 18.5 -17.4 ± 45.1 3.707 0.003* NTrA/IO 59.4 ± 24.9 27.1 ± 22.7 3.348 0.005* PES 27.9 ± 44.7 7.7 ± 17.2 1.818 0.092 NES 46.9 ± 33.1 19.4 ± 20.5 2.497 0.027*
Figure 6. Comparison of pre-test and post-test onset latency (ms) in the DNS group (N = 14).
(DNS: Dynamic neuromuscular stabilization; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; Bar graph with error bar represents mean and standard error; Negative values represent earlier EMG activation relative to the anterior deltoid muscle; *Paired t-test between the pre-test and post-test, p < 0.05.) -24-Fig ur e 6. C om par ison o f pr e-te st and post -tes t ons et la tenc y ( m s) in t he DN S gr oup (N = 14 ). (D NS : D ynam ic neu rom usc ul ar st abi liz at io n; P: Pa ret ic ; N : N onp ar et ic; EO : Ext er na l obl ique ; Tr A /IO : Tr ans ver se abdom ini s/ in te rna l ob liqu e; ES : E rec tor sp inae ; B ar g raph w ith er ror bar r ep re se nt s m ea n and st and ar d erro r; Ne ga tiv e val ues re pr ese nt ea rli er E M G ac tiv at ion rel at iv e to t he ant er io r d elto id m us cle ; *P ai red t-te st bet w ee n the pr e-tes t and pos t-tes t, p < 0.05. )
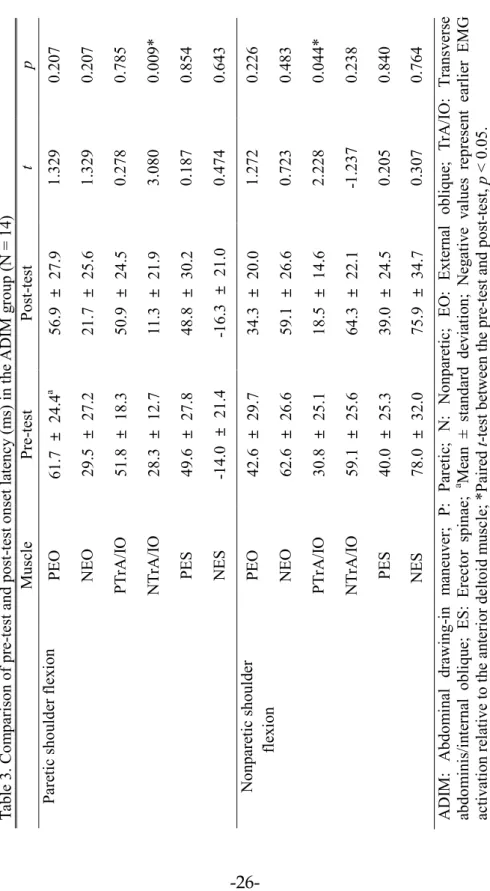
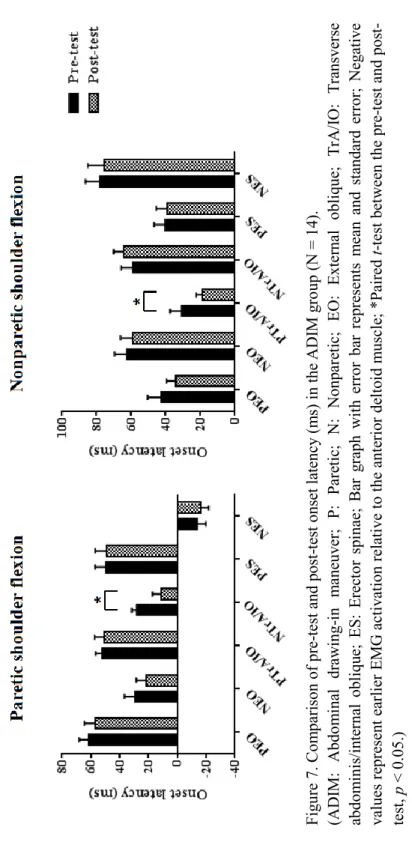
2. Pre-test and Post-test Onset Latency (ms) in the ADIM Group
During the paretic shoulder flexion, there was a significant difference in nonparetic TrA/IO muscle onset latency (p = 0.009) between the pre-test and post-test, but no significant differences were observed in the paretic EO, nonparetic EO, paretic TrA/IO, paretic ES, and nonparetic ES muscles.
During the nonparetic shoulder flexion, there was a significant difference in the paretic TrA/IO muscle onset latency (p = 0.044) between pre-test and post-test, however no significant differences were observed in the paretic EO, nonparetic EO, nonparetic TrA/IO, paretic ES, and nonparetic ES muscles in the ADIM group (Table 3 and Figure 7).
-26-
Table 3. Comparison of pre-test and post-test onset latency (ms) in the ADIM group (N = 14)
ADIM: Abdominal drawing-in maneuver; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; aMean ± standard deviation; Negative values represent earlier EMG
activation relative to the anterior deltoid muscle; *Paired t-test between the pre-test and post-test, p < 0.05.
Muscle Pre-test Post-test t p Paretic shoulder flexion PEO 61.7 ± 24.4a 56.9 ± 27.9 1.329 0.207
NEO 29.5 ± 27.2 21.7 ± 25.6 1.329 0.207 PTrA/IO 51.8 ± 18.3 50.9 ± 24.5 0.278 0.785 NTrA/IO 28.3 ± 12.7 11.3 ± 21.9 3.080 0.009* PES 49.6 ± 27.8 48.8 ± 30.2 0.187 0.854 NES -14.0 ± 21.4 -16.3 ± 21.0 0.474 0.643 Nonparetic shoulder flexion PEO 42.6 ± 29.7 34.3 ± 20.0 1.272 0.226 NEO 62.6 ± 26.6 59.1 ± 26.6 0.723 0.483 PTrA/IO 30.8 ± 25.1 18.5 ± 14.6 2.228 0.044* NTrA/IO 59.1 ± 25.6 64.3 ± 22.1 -1.237 0.238 PES 40.0 ± 25.3 39.0 ± 24.5 0.205 0.840 NES 78.0 ± 32.0 75.9 ± 34.7 0.307 0.764 -26-Tabl e 3. C om par ison o f pr e-te st and po st -tes t onse t l at ency (m s) in t he ADI M g roup (N = 14 ) A D IM : A bdom inal d rawi ng -in m ane uv er ; P: Pa re tic ; N : N onpa re tic; EO : Exte rna l ob lique ; Tr A /IO : Tr ans ver se abdom ini s/ in te rna l obl iqu e; ES : E rec tor spi nae ; a M ean ± st andar d dev ia tio n; N eg at iv e val ues r epr es en t ea rlie r EMG ac tiva tion re la tiv e t o th e an ter io r d el toi d m usc le; *Pai re d t-t es t be tw ee n the p re -tes t and pos t-te st, p < 0.0 5. Mus cl e Pre -te st Post -tes t t p Par et ic shou lde r f lex ion PE O 61.7 ± 24.4 a 56.9 ± 27.9 1.329 0.207 NE O 29.5 ± 27.2 21.7 ± 25.6 1.329 0.207 PTr A /IO 51.8 ± 18.3 50.9 ± 24.5 0.278 0.785 N Tr A /IO 28.3 ± 12.7 11.3 ± 21. 9 3.080 0.009* PES 49.6 ± 27.8 48.8 ± 30.2 0.187 0.854 NE S -14.0 ± 21.4 -16.3 ± 21.0 0.474 0.643 No npar et ic s ho ul der flex ion PE O 42.6 ± 29.7 34.3 ± 20.0 1.272 0.226 NE O 62.6 ± 26.6 59.1 ± 26.6 0.723 0.483 PTr A /IO 30.8 ± 25.1 18.5 ± 14.6 2.228 0.044* N Tr A /IO 59.1 ± 25.6 64.3 ± 22.1 -1.237 0.238 PES 40.0 ± 25.3 39.0 ± 24.5 0.205 0.840 NE S 78.0 ± 32.0 75.9 ± 34.7 0.307 0.764
Figure 7. Comparison of pre-test and post-test onset latency (ms) in the ADIM group (N = 14).
(ADIM: Abdominal drawing-in maneuver; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; Bar graph with error bar represents mean and standard error; Negative values represent earlier EMG activation relative to the anterior deltoid muscle; *Paired t-test between the pre-test and post-test, p < 0.05.)
Figure 7. Comparison of pre-test and post-test onset latency (ms) in the ADIM group (N = 14).
(ADIM: Abdominal drawing-in maneuver; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; Bar graph with error bar represents mean and standard error; Negative values represent earlier EMG activation relative to the anterior deltoid muscle; *Paired t-test between the pre-test and post-test, p < 0.05.) -27-Fig ur e 7. C om par ison o f pr e-te st and post -tes t ons et la tenc y ( m s) in t he ADI M g ro up (N = 14 ). (ADI M : A bdo m inal dr aw ing -in m ane uv er ; P: Par et ic ; N : N onp ar et ic; EO : Exte rnal obl ique ; Tr A /IO : Tr an sve rse abdom ini s/ in te rna l ob liqu e; ES : E rec tor sp inae ; B ar g raph w ith er ror bar r ep re se nt s m ea n and s tand ar d erro r; N eg at iv e val ue s r epr ese nt ea rli er E M G ac tiv at ion rel at iv e to t he ant er io r d elto id m us cle ; *P ai red t-te st bet w ee n the pr e-tes t and pos t-tes t, p < 0.05. )
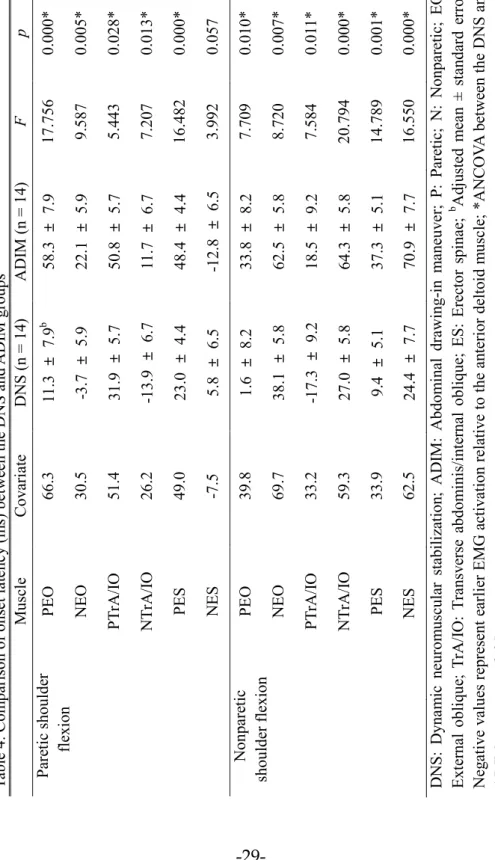
3. Onset Latency (ms) between the DNS and ADIM Groups
During the paretic shoulder flexion, significant differences were observed in the adjusted mean onset latencies between the groups in the paretic EO [F (1, 25) = 17.756, p = 0.000], nonparetic EO [F (1, 25) = 9.587, p = 0.005], paretic TrA/IO [F (1, 25) = 5.443, p = 0.028], nonparetic TrA/IO [F (1, 25) = 7.207, p = 0.013], and paretic ES [F (1, 25) = 16.482, p = 0.000] muscles, respectively. These findings indicate a strong relationship between the groups and the post-test, controlling for the pre-test. However, no significant difference was observed in the adjusted mean onset latency between the groups for the nonparetic ES [F (1, 25) = 3.992, p = 0.057] muscles.
During the nonparetic shoulder flexion, significant differences were found in the adjusted mean onset latencies between the groups in the paretic EO [F (1, 25) = 7.709, p = 0.010], nonparetic EO [F (1, 25) = 8.720, p = 0.007], paretic TrA/IO [F (1, 25) = 7.584, p = 0.011], nonparetic TrA/IO [F (1, 25) = 20.794, p = 0.000], paretic ES [F (1, 25) = 14.789, p = 0.001], and nonparetic ES [F (1, 25) = 16.550, p = 0.000] muscles, respectively. These findings suggest a strong relationship between the groups and the post-test, controlling for the covariate (Table 4 and Figure 8).
Table 4. Comparison of onset latency (ms) between the DNS and ADIM groups
DNS: Dynamic neuromuscular stabilization; ADIM: Abdominal drawing-in maneuver; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; bAdjusted mean ± standard error;
Negative values represent earlier EMG activation relative to the anterior deltoid muscle; *ANCOVA between the DNS and ADIM groups, p < 0.05.
Muscle Covariate DNS (n = 14) ADIM (n = 14) F p Paretic shoulder flexion PEO 66.3 11.3 ± 7.9 b 58.3 ± 7.9 17.756 0.000* NEO 30.5 -3.7 ± 5.9 22.1 ± 5.9 9.587 0.005* PTrA/IO 51.4 31.9 ± 5.7 50.8 ± 5.7 5.443 0.028* NTrA/IO 26.2 -13.9 ± 6.7 11.7 ± 6.7 7.207 0.013* PES 49.0 23.0 ± 4.4 48.4 ± 4.4 16.482 0.000* NES -7.5 5.8 ± 6.5 -12.8 ± 6.5 3.992 0.057 Nonparetic
shoulder flexion PEO 39.8 1.6 ± 8.2 33.8 ± 8.2 7.709 0.010* NEO 69.7 38.1 ± 5.8 62.5 ± 5.8 8.720 0.007* PTrA/IO 33.2 -17.3 ± 9.2 18.5 ± 9.2 7.584 0.011* NTrA/IO 59.3 27.0 ± 5.8 64.3 ± 5.8 20.794 0.000* PES 33.9 9.4 ± 5.1 37.3 ± 5.1 14.789 0.001* NES 62.5 24.4 ± 7.7 70.9 ± 7.7 16.550 0.000* -29-Tabl e 4. C om par ison o f ons et lat enc y ( m s) bet w een th e DNS and A D IM g roups D NS : D yna m ic neur om usc ul ar st abi liz at ion ; ADI M : A bdom inal dr awing -in m ane uv er ; P: Par et ic ; N : N onpar et ic; EO : Exte rnal obl ique ; T rA /IO : Tr ans ver se a bdom ini s/ in te rnal ob lique ; ES : Er ec tor s pi nae ; b A dj ust ed m ea n ± s tanda rd erro r; N eg at iv e val ues rep res ent ea rli er EMG a ct iv at ion rel at iv e to t he an ter io r de lto id m usc le; * ANC OV A b et we en th e DNS an d A D IM g roups , p < 0.05 . Mus cl e C ov ar iat e DNS (n = 14 ) A D IM ( n = 14 ) F p Pa ret ic shou lde r flex ion PE O 66.3 11.3 ± 7.9 b 58.3 ± 7.9 17.756 0.000* NE O 30.5 -3.7 ± 5.9 22.1 ± 5.9 9.587 0.005* PTr A /IO 51.4 31.9 ± 5.7 50.8 ± 5.7 5.443 0.028* N Tr A /IO 26.2 -13.9 ± 6.7 11.7 ± 6.7 7.207 0.013* PES 49.0 23.0 ± 4.4 48.4 ± 4.4 16.482 0.000* NE S -7.5 5.8 ± 6.5 -12.8 ± 6.5 3.992 0.057 No npar et ic shoul der fl exi on PE O 39.8 1.6 ± 8.2 33.8 ± 8.2 7.709 0.010* NE O 69.7 38.1 ± 5.8 62.5 ± 5.8 8.720 0.007* PTr A /IO 33.2 -17.3 ± 9.2 18.5 ± 9.2 7.584 0.01 1* N Tr A /IO 59.3 27.0 ± 5.8 64.3 ± 5.8 20.794 0.000* PES 33.9 9.4 ± 5.1 37.3 ± 5.1 14.789 0.001* NE S 62.5 24.4 ± 7.7 70.9 ± 7.7 16.550 0.000*
Figure 8. Comparison of onset latency (ms) between the DNS and ADIM groups.
(DNS: Dynamic neuromuscular stabilization; ADIM: Abdominal drawing-in maneuver; P: Paretic; N: Nonparetic; EO: External oblique; TrA/IO: Transverse abdominis/internal oblique; ES: Erector spinae; Bar graph with error bar represents adjusted mean and standard error; Negative values represent earlier EMG activation relative to the anterior deltoid muscle; *ANCOVA between the DNS and ADIM groups, p < 0.05.)
-30-Fig ur e 8. C om par ison of on se t l at enc y ( m s) b et w ee n th e DN S and ADI M g roups . (D NS : D ynam ic neur om usc ul ar s tab ili zat ion; A D IM : A bdom inal d rawing -in m ane uv er ; P: Pa re tic ; N : N onpar et ic; EO : Exte rnal obl ique ; T rA /IO : T rans ver se ab dom ini s/ in te rnal ob liq ue ; ES : Er ec tor sp inae ; B ar g rap h w ith er ror bar repr es en ts ad jus ted m ea n and st anda rd e rr or ; N eg at iv e val ues repr es en t ea rli er E MG ac tiv at io n rel at iv e to t he an ter io r de lto id m usc le ; *ANC OV A b et we en th e DN S and A D IM g roups , p < 0.05. )
Discussion
To the best of our knowledge, this study is the first clinical trial highlighting the effects of 4-week DNS and ADIM exercises on APA in individuals with chronic hemiparetic stroke. As anticipated, DNS training was more effective for improving APA via the coordinated neuromuscular activation of postural trunk muscles than the ADIM training. Most importantly, our novel EMG results showed significantly improved feedforward activation time after the DNS intervention. It was difficult to compare our results with those of previous APA studies, because according to our extensive review of the literature, the effects of postural stabilization exercises on APA in populations with neurological impairments have never been investigated.
In a between-group comparison, during the paretic shoulder flexion, the DNS group showed more decreased APA onset latency in the paretic and nonparetic EO, paretic and nonparetic TrA/IO, and paretic ES muscles than the ADIM group. Similarly, during the non-paretic shoulder flexion, significant differences in the paretic and nonparetic EO, the paretic and nonparetic TrA/IO, and the paretic and nonparetic ES muscles were found between groups. These findings suggest that the DNS intervention was more effective than the ADIM intervention in enhancing onset latencies in paretic and nonparetic EO and TrA/IO muscles. Perhaps DNS emphasized a subconscious feedforward mechanism that involved a relatively short-loop latency of APA (Frank, Kobesova, and Kolar 2013). However, the ADIM focused on a
conscious feedback mechanism (Lee et al. 2011), which involved a long-loop latency APA. Interestingly, Cordo and Nashner (1982) examined APA associated with rapid arm movements induced by variable handle perturbations with hand-held manipulandum in healthy adults. The APA responses were modulated on a subcortical level before voluntary movement and were not modified by a conscious-level effort (Cordo, and Nashner 1982). However, the present study demonstrated that the delayed onset latency of postural trunk muscles in individuals with chronic hemiparetic stroke was improved following both interventions. This implies that regardless of the intervention modes, altered or delayed preactivation time in individuals with hemiparetic stroke can be modified to a certain degree or near to normal APA as evident in the present APA data.
In the DNS group pre-/post-test comparison, during the paretic shoulder flexion, significant differences in the paretic and nonparetic EO, nonparetic TrA/IO, and paretic ES muscle onset latencies were observed between the pre-test and post-test. During the nonparetic shoulder flexion, significant differences in the paretic and nonparetic EO, paretic and nonparetic TrA/IO, and nonparetic ES muscle onset latencies were found between the pre-test and post-test. These results suggest that the delayed APAs (51.1 – 76.9 ms after AD activation) improved (31.8 – 41.5 ms after AD activation), which was comparable to previous APA data in which the range was from 100 ms before to 50 ms after AD activation in normal adults (Aruin, and Latash 1995, Hodges, and Richardson 1997).
In the ADIM group pre-/post-test comparison, significant differences in the nonparetic and paretic TrA/IO muscles were evident between the pre-test and post-test during either the paretic or nonparetic shoulder flexion, respectively. These results are consistent with Tsao and Hodges‟s study (2007), which compared the immediate effects of „Sit-up‟ and „ADIM‟ on APA in 22 individuals with recurrent LBP. The ADIM was effective in improving TrA muscle onset time during rapid shoulder flexion and extension movements (Tsao, and Hodges 2007). These findings suggest that the ADIM intervention was also beneficial for the enhancement of APA and the repetitive practice of ADIM overtime became automatic once the skill was mastered (Hayashi et al. 2002).
In the present study, baseline ES onset time data at the pretest was comparable to the results from Dickstein et al. (2004), which showed preactivation time of the contralateral ES muscle during paretic shoulder flexion in individuals with hemiparetic stroke. Moreover, the onset latencies in the ipsilateral EO and TrA/IO muscles during either the paretic or nonparetic shoulder flexion were delayed, ranging from 51.1 to 76.9 ms after AD activation. The contralateral EO and TrA/IO muscles showed earlier EMG activation relative to the ipsilateral EO and TrA/IO muscles during shoulder flexions which suggests that the contralateral postural trunk muscles preactivated to stabilize the trunk on the contralateral side to the shoulder flexion in individuals with chronic hemiparetic stroke (Dickstein et al. 2004).
The EMG onset latency in the present study was relatively variable during rapid shoulder flexion. Such variability may stem from altered motor recruitments in
individuals with stroke (Gemperline et al. 1995) or visually unnoticed compensation. The latter may be unlikely because the present experiment discarded data and repeated data collection if any potential compensatory activation was apparent. Nevertheless, the present results showed a promising difference within the group (pre-test vs. post-(pre-test) and between groups (DNS vs. ADIM), suggesting that both interventions were effective in improving APA, but DNS was seemingly superior to ADIM.
Although the present study has revealed meaningful findings, it also has several limitations that could be addressed in future studies. First, a surface EMG was used to record TrA/IO muscle movements in this study, so a fine-wire EMG should be used in future studies to prevent the crosstalk of the abdominal muscles. Second, a larger sample size is required for further investigations because it was difficult to generalize findings obtained from the small sample sizes of the two groups. Third, self-selected rapid shoulder flexion velocity should be recorded to investigate the association between arm flexion velocity and the APA patterns in individuals with hemiparetic stroke. Finally, a future research should focus on plastic changes in the excitability of the cerebral or cerebellar cortex, as measured by functional magnetic resonance imaging. Despite these various limitations, our findings make an important contribution to knowledge on the APA response associated with DNS and ADIM exercises in individuals with chronic hemiparetic stroke.
Conclusion
This study has provided the first empirical evidence on the comparative effects of 4-week DNS and ADIM exercises on APA responses during a rapid shoulder flexion task in individuals with chronic hemiparetic stroke. The study has demonstrated that DNS exercise was more effective than ADIM to mitigate delayed APA in the selected TrA/IO and EO muscles because DNS uses a feedforward mechanism that tends to involve a shorter APA process. Our findings may provide conceptual and clinical insights for clinicians into the examination and management of postural core stabilization in individuals with chronic hemiparetic stroke.
References
Anderson Worth SG, Henry SM, and Bunn JY. Real-time ultrasound feedback and abdominal hollowing exercises for people with low back pain. NZ J Physiotherapy. 2007;35(1):4–11.
Aruin AS. The organization of anticipatory postural adjustments. J Automatic Control. 2002;12:31–37.
Aruin AS, and Latash ML. Directional specificity of postural muscles in feed-forward postural reactions during fast voluntary arm movements. Exp Brain Res. 1995;103:323–332.
Bennis N, Roby-Brami A, Dufosse M, and Bussel B. Anticipatory responses to self applied load in normal subjects and hemiparetic patients. J Physiol Paris. 1996;90:27–42.
Boussuges A, Gole Y, and Blanc P. Diaphragmatic motion studied by m-mode ultrasonography: Methods, reproducibility, and normal values. Chest. 2009;135(2):391–400.
Chaitow L, Bradley D, and Gilbert C. Recognizing and Treating Breathing Disorders: A Multidisciplinary Approach. 2nd ed. Edinburgh: Churchill Livingstone, 2014.
Chung EJ, Lee BH, and Hwang SJ. Core stabilization exercise with real-time feedback for chronic hemiparetic stroke: A pilot randomized controlled trials. Restor Neurol Neurosci. 2014;32(2):313–321.
Cordo PJ, and Nashner LM. Properties of postural adjustments associated with rapid arm movements. J Neurophysiol. 1982;47:287–308.
Cram JR, Kasman GS, and Holtz J. Introduction to Surface Electromyography. Gaithersburg: Aspen, 1998.
Dickstein R, Shefi S, Marcovitz E, and Villa Y. Anticipatory postural adjustment in selected trunk muscles in poststroke hemiparetic patients. Arch Phys Med Rehabil. 2004;85:261–267.
Frank C, Kobesova A, and Kolar P. Clinical commentary: Dynamic neuromuscular stabilization and sports rehabilitation. Int J Sports Phys Ther. 2013;8(1):62–73.
Garland SJ, Stevenson TJ, and Ivanova T. Postural responses to unilateral arm perturbation in young, elderly, and hemiplegic subjects. Arch Phys Med Rehabil. 1997;78:1072–1077.
Gemperline JJ, Allen S, Walk D, and Rymer WZ. Characteristics of motor unit discharge in subjects with hemiparesis. Muscle Nerve. 1995;18(10):1101–11014.
Henneman E. Relation between size of neurons and their susceptibility to discharge. Science. 1957;126(2387):1345–1347.
Henry SM, and Westervelt KC. The use of real-time ultrasound feedback in teaching abdominal hollowing exercises to healthy subjects. J Orthop Sports Phys Ther. 2005;6:338–345.
Hides J, Wilson S, Stanton W, McMahon S, Keto H, McMahon K, Bryant M, and Richardson CA. An MRI investigation into the function of the transverses abdominis muscle during “Drawing-in” of the abdominal wall. Spine. 2006;31(6):E175–E178.
Hodges PW, and Richardson CA. Relationship between limb movement speed and associated contraction of the trunk muscles. Ergonomics. 1997;40:1220–1230.
Hodges PW, and Richardson CA. Transversus abdominis and the superficial abdominal muscles are controlled independently in a postural task. Neurosci Lett. 1999;265:91–94.
Kolar P, Sulc J, Kyncl M, Sanda J, Cakrt O, Andel R, Kumagal K, and Kobesova A. Postural function of the diaphragm in person with and without chronic low back pain. J Orthop Sports Phys Ther. 2012;42(4):352–362.
Lee NG, You JH, Kang SK, Lee DR, Kwon OY, and Jeon HS. Novel augmented ADIM training using ultrasound imaging and electromyography in adults with core instability. J Back Musculoskelet Rehabil. 2011;24:233–240.
Liebenson C. Rehabilitation of the Spine: A Practitioner's Manual. 2nd ed. Philadelphia: Lippincott Williams & Wilkins, 2007.
Lim JS, Lee SY, Lee DH, and Park JS. The effect of a bridge exercise using the abdominal drawing-in maneuver on the balance of chronic stroke patients. J Phys Ther Sci. 2012;24:651–653.
Marshall P, and Murphy B. The validity and reliability of surface EMG to assess the neuromuscular response of the abdominal muscles to rapid limb movement. J Electromyogr Kinesiol. 2003;13:477–489.
O’Sullivan PB, Twomey L, and Allison GT. Altered abdominal muscle recruitment in patients with chronic back pain following a specific exercise intervention. J Orthop Sports Phys Ther.1998;27:114–124.
Pereira S, Silva CC, Ferreira S, Silva C, Oliveira N, Santos R, Vilas-Boas JP, and Correia MV. Anticipatory postural adjustments during sitting reach movement in post-stroke subjects. J Electromyogr Kinesiol. 2014;24:165–171.
Richardson CA, Hodges PW, and Hides J. Therapeutic Exercise for Lumbopelvic Stabilization. 2nd Ed. Philadelphia: Churchill Livingstone, 2004.
Tsao H, and Hodges PW. Immediate changes in feedforward postural adjustments following voluntary motor training. Exp Brain Res. 2007;181:537–546.
국문 요약
만성 뇌졸중 환자에서 선행자세적 조절에 대한
동적 신경근 안정성 훈련과 복부당김 기법의 효과비교
연세대학교 대학원
물리치료학과
이 남 기
본 연구의 목적은 만성 뇌졸중 환자를 대상으로 동적 신경근 안정성 훈 련과 복부당김 기법을 적용하였을 때 선행자세적 조절에 미치는 효과를 비 교하는 것이다. 28명 만성 뇌졸중 환자가 참여하였으며, 그들은 동적 신경근 안정성 훈 련 집단과 복부당김 기법 집단으로 무작위 배정되었다. 동적 신경근 안정성 훈련과 복부당김 기법은 4주 동안 30분씩 주 5일간 시행되었다. 선행 자세적 조절은 빠른 어깨 구부림을 하는 동안 배바깥경사근과 가로배근/배 속경사근, 척주세움근에 대한 근전도상 개시잠복의 측정으로 결정되었다. 동적 신경근 안정성 훈련과 복부당김 기법의 적용 전과 후 사이의 차이를 알기 위하여 짝비교 t-검정을 사용하였고, 집단 간의 차이를 비교하기 위 해 공분산분석을 사용하였다. 유의수준은 α=0.05로 했다. 짝비교 t-검정은 동적 신경근 안정성 훈련 전과 후 사이에 배바깥경사 근과 가로배근/배속경사근의 개시잠복에 대한 유의한 차이를 보였다. 복부 당김 기법은 가로배근/배속경사근의 개시잠복에 대한 유의한 차이를 보였 다. 공분산분석은 마비측의 빠른 어깨 구부림에 대한 비마비측 척주세움근 을 제외하고, 마비측과 비마비측의 빠른 어깨 구부림에 대한 모든 자세적 중심 근육들(배바깥경사근과 가로배근/배속경사근, 척주세움근)의 개시잠 복에서 집단 간의 유의한 차이가 나타났다. 그러므로, 이 연구의 결과는 동적 신경근 안정성 훈련이 만성 뇌졸중 환자에서 자세적 중심근육의 피드 포워드 활성화를 통해 선행자세적 조절을 개선함으로써 복부당김 기법보다 효과적이라는 것을 시사한다. 핵심 되는 말: 동적 신경근 안정성, 만성 뇌졸중, 복부당김 기법, 선행자세 적 조절.