댄흐
Journ믿 P’
뼈맨현쁘 U딴판,e만딩 Vol. 10,N0-,-2(Decernber),~013 •Evaluation of Carotid Atherosclerosis Using Three-Phase
CT'
In YoungKim
’,
Sun Young Jeong',
Ji Kang Park' lJeju Nalional Universily SCh∞
1이Medicine,2Depar1menl이Radiol얘y,Jeju Nalional Universily SChoolof Medicine,Jeju,Korea
(ReceivedJuly 18‘2013; Revised Ju1y 25,2013; Aαepled July 31,2013)
Abstraet
→←」
Purpose: Carotid atherosclerolic plaque (CAP) was evalualed by Ihree-phase CT ITPCT; CT_,CT••••,CT_). The purposes 01 lhis study are 10: (1) 10 delermine oplimal phase for the visualizalion 01 CAP companents; (2) evaluate whether there is a significan1 difference in the Quantitative CT Hounsfield unit (CTHUs) of the CAP companenls between Ihe arterial and delay phase
Ma1erials and Me1hods : Two re끼ewers evaluated the deteclion rale and image quality lor CAP components on CT_ and CTæ
‘
source images in 36 palients. Quanlitat;ve analysis 01 the CTHUs for the soft plaque and outer wall was performed in 47 arteries. The CTHUs were measured for Ihe soft plaque and the outer wall using the manual ROI method for each carotid plaque. The difference 01 image quality on CT•••••.•.and CTdclclv,the difference 01 the CTHUs according 10 CT phase ,the dil’
erence in CTHUs according to the arterial symptomatology or slenosis degree were stalis1ically evaluatedResutts : CTdOIIOl'was the optimal phase for the delineation of soft plaque and ou1er wall enhancemenl. The CAP companents showed progressive delayed enhancement. There were statistically signilican1 increase in" the enhancement 01 the 。이er wall Ihrough TPCT (p (0.001). CTHUs이S이t plaque and ouler wall on CT
""‘
and CT.--.,
did nol show 잉gnificanl correlations wilh symplomalology. The CTHUs 01 soft plaque on CTM~ (p =0.02) and CTHUs 01 Ihe ouler wall on CT.‘
..
(p =0.01) weresignificanlly higher in the group 01 symptomatic ar1eries or severely stenotic arteries together that that in the group 01 asymptomatic ar1eries with less than 70% stenosis‘
Conclusion : CT.-
,
was lhe 。이mal phase for plaque detection and the characterization 이plaque compane미s,(J Med UfeSci 2013;1 0(2):94-1 00)
Key Words ; CT,C앙ωd 앙'leIγ. Atherosclerotic plaque
Correspandence10: Jj Kang ?ark
Departmenlof Radlology,Jeju Nalion히University Hospilal,
Jeju Nalional UniversitySCh。이 이 Medicine,
1753-3,Ara-HJon9 ,JEJU-SI,Jeju 690-767,Republìc이Korea E-mail: jkconlrast@l미aver.com
Carotid atherosclerotic plaque (CAP) is one of π에or and preventable causes of ischemic cerebr.외sbuke,Early clliUc~
studies revealed that the degree of stenosis and symptomatology are the most import밍1t prognostic factor of
carotid atherosclerosis in predicting the risk of future sσ'okes (1-3). lt was shown that carotid endarterectomy is benefici외m 양mptomatic patients wi야1 stenosis greater th밍1
70% (4). However,there have been debates about whetl1er a revascularization procedure is beneficiaJ in patients with
8양mptomatic high grade stenosis or in symptomatic patients
with moderale slenosis (5,6) 꺼1e dynamic natural course
。
f atherosclerotic plaque and the role of inflarnmation in the progression of atherosclerotic plaque have been iden마00.introduction
j
and the concept of vulnerable plaque has been int.roduced (7-10). Vu1nerable plaques,which are prone to rupωre ,have the following characteristics: hi엉1 inflammaωry cell비와
infiltration ,thin or ruptured fibrous cap,fresh luminal thrombus near the CAP. a large LRNC. sænosis greater than 90%,and intraplaque hemorrhage (11-13). To delect these characteristics ,MRI has been widely used in CAP imaging. MRI can display CAP with sufficientJy hi앙1 spati외
resolution to measure accurate plaque volume and can differentiate CAP components ,such as a :fibrous caps. LRNC,and intraplaque hemorrhage (14,15),In addition , MRI can assess the burden of i삐와nmatory cell inmσation within the plaque using a macrophage-speci:fic contrast agent (16,17),ln contrast to MRI,CT has not been widely used in CAP imaging due ω its limited soft tissue conσ'ast However. recent CT studies using CT 와땅1。양'aphy (CTA) and its source image have reve외려 a polenti~ role of CT for plaque imaging. Despite the overlap and the variable r밍19'e of CT Hounsfield unit (CTHU). these studies reve외ed that plaque components such as LRNC,fibrous tissue ,and
hemorrhage could be characterized according to C1HU 08.
19)
Recent investigation revealed that neoangiogenesis within the CAP is a marker of plaque vulnerability and is associated with intraplaque hemorrhage. necrosis,and inf1ammaωrycell inmσation (20-22). Neoangiogenesis arises from the vasa vasorum of the adventitial layer (22)‘
Neoangiogenesis has been evaluated by MRI밍ld US with contrast agent,and the density and charaeteristics of neoangiogenesis have been evaluated by DCE-MRI Adventitial (carotid outer wall) Klta‘showed a good c
。
π'elation with the amount of neoangiogenesis and the degree of macrophage infùtration (23. 24) 까le carotid outer W외1 showed progressive and delayed enhancement in DCE-MRl studies and dYJ냉mic MR wall imaging. and the peak enhancement occurred nearly three minutes after contrast agent adminisσ'ation(24,25). CTA has been become one of the first-line methods for the evaluation of carotid atheros“
clerosis; however,dynarnic CTA are limited due to the problem of radiation exposure,외ld there have been n。
repoπ5 on dynamic CTA. CTA is usually perfonned with a sing1e arteri외phase or two phases,including a preeontrast and arterial phase. for bone subtraction. In this study‘we
미ed three-phase CT (TPCT) for CAP imaging as follows CTP"l.CT-π and CTdHIo'wi야1 야rree minutes after eontrast agent adminisσ'ation
π1e purposes of야lis study are 10: (j) ω detennine which
phase is better in depicting
∞
rotid plaque components; (2) assess the pattem of contrast enhaneernent in the CAP component by measuring quantitative CTHUs in CT-.,. andCT,‘"'"'"phase; (3) evaluate whether there is a significant
difference in the quantitative CTIfUsof the CAP components according to symptomatology or joint grouping of symptomatologyor severe stenosis of greater th밍1 70%
Malerials and Melhods
까니s study was approved by the Iocal research committee,
and all patients gave written infonned consent prior t
。
inclusion. From May 2008 to October 2008. 102 patients were consecutively enroUed. TPCT studies were performed for the screening of carotid atherosclerosis or the evaluation。
f vascular lesions in patients with recent ischemic cerebr외sσ'Oke.Among these 102 patients. 66 were excluded because
。
f the absence of carotid plaque in both carotid arteries,and 36 patients were finally included in this study (69.4:t1O.4. M:F=27:9).Risk싫etors for atherosclerosis were
as follows: diabetes mellitus 38.9%(14/36). hypertension
Evaluationof CarotidAtheroscJerosisUsing1'hree-Phasec1잉
11.1% (4/36). hyperlipidemia 22.2% (8/36). and heavy smoking greater than 20packs/year 11.1%(4/36). A recent eerebral ischemic event within one month of the CT study had occurred in 10 patie따s. and CAP in 10 arteries was associated with recent ischemic stroke in the arterial territory of the ipsilateral cerebral hemisphere. These arteries were regarded as앙mptomatic arteries.
Image acquisilion
CTA was peñormed with a 16-detecror row CT scanner (Sensation 16; Siemens‘Erlangen. Germanyl Patients were
positioned supine with앙1eir anns along the chest on the CT
table. The scan range reached from the ascending aorta t
。
the skull base or the 잉rcle of Wìllislevel (2 cm above Üle sella) for CT…
and CTartel"7.The arterial phase was determined by real-time bolus뼈cking. and the delay phasewas acquired three minutes after contrast agent aφninisìration. For CT~. the center slice was positioneclat the level of the angle of the mandible angle,and the z-axis coverage was set to 8 cm. 80 ω 100 mL of nonionic conσast agent (Ultra
、
rist 370; Schering. Berlin. Germany) was injected with a power injeetor at a rate of 4 mL/s followed by a saline f1ush of 50 mL 매e n앙1t antecubi때]vein was preferentially used. Scanning parameters were 0.75-nun collimation. 12-nun (pitch of 1) table feed per rotation. 0.5-second rotation time. 120 kV. and 160-180 mAs. Additional CTDlvol for CT.ωrqwas 5.6:t0.3 mGy Sections were reconstructed with 1.0 mm increments and a soft convolutionkemel æ20)
Image analysis
π1e CT••••".뻐d CT6Ia:1 source images were retrospectively analyzed by two radiologists. Carotid artery stenosis on CT-.,. was measured by Reviewer 1 on a workstation
(Leonsrdo. Siemens) using the standard NASCETmethod'. Both reviewers independently eva1uated the presence of carotid plaques near the carotid bifurcation on CT-.,. and
CT.,.source image. Each phase of the source images were
reviewed separately in three sessions at one-week inteπ머s and was independently assessed by the two reviewers Carotid plaque cornponents were classified by visual assessment of CT morpholo양 and CTHUs as follows. 80ft plaque was defmed by a low density on CTarll'fJ'and CTcHa1 and CTHUs between 0 and 70 π1e carotid outer w외1 was
identified by enhancement on CT"""'Tand CT-.:r. Then the reviewers evaluated the deteetión rate and over외1 image
In YoungKim,5un YoungJeong. Ji KangPark
Interobserver variability in interpreting the detection rate and U1e quality of the images was ca1culated with " statistics using SPSS version 15.0,with <
<:
0.80 defmed as excellent agreement ,K = 0.60 to 0.79 as good agreement. and K = 0.50 ω 0,59 as moderate agreement π1e significant difference in the quality of CT images in each phase for depiction of carotid plaque components was determined with Friedman two-way analysis of variance by ranks. The differences of the CTHUs according to CT phase in each arteIγ were assessed using paired t-test. To evaluate the difference in CTHUs according ω the arterial 양mpωmatology or grouping ofsymptomatology or severe stenosis greater than 70% together versus asymptomatic 양teries wiU1 stenosis less th밍1 70%,independent t-tests were perfonned for soft
plaque and the outer arterial wall. When we used 70% stenosis as the criteria,5 arteries were added to the 10 qu외ity for U1e depicti.on of carotid plaque components on the CT-ι and CTdelI3'using the following sca1es comparing CT-.,. and CT~ source image‘For soft plaque: 0 for no
visible soft plaque. 1 for suspicious soft plaque with luminal contour change,and 2 for clearly visible low-densît\Ysoft plaque. For carotid outer w외1: 0 for less than 20% visible
fractions of the nonnal wall circle. 1 for 20 to 50% visîble fractions of the normal wall circle. and 2 for more than 50% visible fractions of the normal wall cîrcle. Thirdly QuantitBtive analysis based on the CTHUs of soft plaque and the outer wall was peñormed. We included the arteries wl야1 the CAP that had a measurable area of soft plaque on CT~여‘and 47 carotîd arteries were evaluated for ROI
analysis. Reviewer 1 measured the CTHUat the soft. plaque and outer wa11in 1 to 3 slices according ω plaque burden with a manual ROI method at each CAP. For soft plaque cπ-lUs‘a ROI covering 50 ω 80 pixels was drawn in the
centl'al part of the soft plaque in the same posi디。n on the CT•..•••,..and CT.s.lI1source images. For the CTHUs of the
。
uter waIl. a ROI covering 3 to 10 pixels was drawn in the잃me position on the CT""""",.and CT~ source images. In
the analysis of s.따 plaque in 37 asymptomatic arteries,5 arteries in CTRl"lf!r7were excluded because reliable Ror measurement was difficult due to the sma)) size and indistinct visualization of the soft plaque. ln tlle ana1ysis of tlle outer wall in 37 a앙mpωmatic arteries,6 arteries in CT-.,..2 arteries in CTdolatwere excluded for the same
[_ .. Resul!s
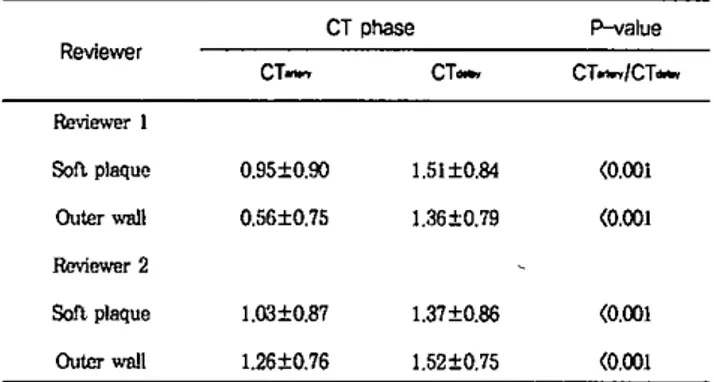
Table 1. Results of carotid plaque detection in CTartery and CTdelay phase source image
72 T이.1 72 9 8 63 64 CTPhase CT_ N얘 60 60 CT_ 2 Re띠ewer CTphase P-value Re
、
ne
앤r CT_ CT_ CT-•./CT_ &에ower1S이t plaqu(! O.95::tO.90 1.51:tO.84 (0.001
ou
‘
erwall 0.56"0.75 1.36::tO.79 (0.001&에ew연<2
80ftplaque 1.03::tO.87 1.37::tO.86 (0.001 Ou""w피l 1.26tO.76 1.52::tO.75 (0.001 symptomatic arteries. The norma1it;yassumption was verified using the Shapiro-Wilk test. 8tBtistica1 sîgnificance was dermed at an외pha level of p(0.05,two tailed. SPSS (SPSS Inc.,Chicago,JL) statistical software was used for all computaüons
The mean degree of stenosis in the 47 arteries was 57.5%:!:31.5‘and the mean degree of stenosis in the 10 symptomatic arteries was 84.4%:t 16.5. The degree of st.enosis in the 5 a양mptomatic arteries with stenosis greater
than 70% was 74.2:!:5.9%. The mean stenosis in the 32 arteries wiili stenosis less th밍1 70% was 29.2:!:18.4%. For both observers‘CAP was more frequently detected in
CTdelay images than in CT_ images (Tablej)
Interobserver agreement for the detection of CAP in CT••••,., 밍ld CT.••,. source image was excellent. For overa11image
quaIity‘CTddo:Timages were statistically superior to the CT- .•,.
images for the delineation of carotid plaque components (Table 2)
Table 2. Results of the image quality of source images from CT-.n"'7and CT
“
n for depicting carotid plaquecomponents
CT.••,.was the better than CT•••••,. for the delineation of
soft plaque and outer wa11enhancement for 빙1 reviewers (Fï밍lre 1). Jnterobserver agreement for the image quality when depicting the components of CAP was as follows good in CT_ for soft plaque (< = 0.69). and moderate in Statislical analy~s~s
τ
reason
Evaluation of Carotid Atherosclerosis using Three- Phase CT
Table 3. Comparison of the C'l'HUs of the soft plaque 밍ld the outer
、
vεùl in TPCT source image from each phase outer wall between CT8rteIY, and CTdιιy images (p-value<
0.001,Table 3) CT phase 0.07 (0.001 P-value CT-이S. CT"",., CT ••,"" 71.7:1::20.1 41.0:1::18,9 CT,… 49.3:112.7 37-7:114.2 Reviewer 80ft plaque αlter Wall Fi밍ne 1. De에ction 01' carotid p빼Je on TPCT. C뻐하ay is thebest phase for the depiction of the soft plaque ar펴ouær
、
Nall among Ü1e ü1ree pbasesCTdclo,y for the outer wall (K = 0.56) and in CTarIeryfor soft
plaque depiction (K =0,53). There were statistically
Sl망파icant differences of the con납ast enhancement in the
The outer wall showed more prominent enhancement in CTμi'IYthan in CT8rtery.The difference in CTHUs of soft plaque enhancement was not signif'icant between CTmteηand CTdel"" CTHUs of soft plaque and the outer wall on CTdel8yand
CT",,,,ry did not show significant correlations with group
membership of arteri머symplomalology (Table 4)
Table 4. Comparison of the Cπ-IUs between symptomati.c and asymptomatic arteries
Reviewer
Symptom(+}
S01lPlaque
SymplomH p-value Symptom(+}
OulerWall Symplor미 ) p-value CT_ CT.“” 41.7:1::10.8 43.2:1::13.5 35.7:114.6 39.2:115,9 0.24 O갱 52.9:t11.9 73.8:1::11.8 47.6土12.9 67,4:t17,4 0.26 0.28
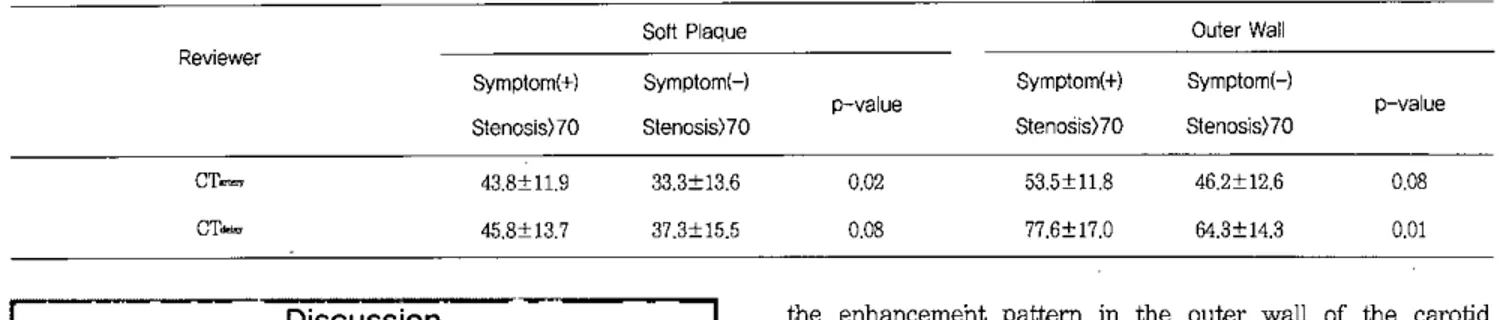
Tbe CTHUs of soft plaque on CT_ (P=0.02) and CTHUs of the outer wall on CT,“""(P=O,Ol) were significantiy higher in the group of symptomati.c 양teries or severely stenotic
arteries together that the CTHUs in the group of asymptomatic 밍ieπes with 1ess than 70% stenosis (Figure 2,
Table 5) B ~."
영
훌’
M ; §~.
Á~~Fi밍Jre 2. The difference in the CIHUs of the outer wall between symptomatic/severe stenotic arteries (greaær 뼈1 7CP1o sten
∞
is) and asymptαnatic 앙따ies wi.th stenosis less than 700'c어)π1e outer w머lofan asymptomatic arterγ has a nod버.ar calcification 뻐dthin wall wiÜ1 rnild enhanεement (1짧 cohnnn,arπW , CIHU 65). 1he ouær w머1 of a양mpìomatic ar떠γ has
、뼈1 enhancement (ri영lt cohunn,려TOW,CIHU 없:).æ)
Symptomatic or severe stenotic arteries show
잉gnificantly greater enha nc(αnent in 1he outer w밍l ü1an a앙mptomatic arteries wi.1h stenosis less than
7Cff
,
(P=O.ollSt.n
。…
e<TO% Sympt。찌
<-J,>T。‘
E"",B.‘
.h"•• 95。‘
Ctor"'''nIn Young Kim,Sun Young Jeong,Jî Kang Park
Table 5. Comparison of the CTHUs between symptomatic/severe1y stenotic arteries and asymptomatic arteries 、、rith stenosis 1ess than 70% 80ftPlac니e Reviewer CT_ CT_ Sym이m미:+) 8lenosis)70 43.8:t11.9 45,8:t13.7 8ymplor미 ) Slenc잉s)70 33,3:t13,6 37.3:t15.5 OuterW에 Symptor미+) Symptom(냐 P→ alue p-value Stenosìs)70 Slenosis)70 0,02 53.5:t11.8 46.2:t12.6 0,08 0,08 77,6:t17,O 64,3:t14,3 0,01
L_
‘ Discussion츠---그
In previous CT-based studies from the symptomatic patients ,plaque composition was evaluated according to CTHUs in arterial phase 'source images; the CTHUs of LRNC ranged from 22.9 to 32.6,and the CTHUs of fibrous tissue ranged from 46.4 1D 52,9 (18,19),In terms of CTHUs,the soft p1aque in our study may correspond to the mixture of LRNC없d fibrous tissue in the previous CT studies. In this
study,the component of the CAP showed progressive and delay enhancement. De1ayed enhancement is defmed as an increase of w외1 enhancement that occurs several mÎIlutes af‘"-ter contrast infusion in comparison with the degree of enhancement of상1e arterial phase. Delayed enhancement of the arterial wal1 has been reported in coronarγ p1aque MRI and aortic aneurysm CT study. De1ayed enhancement was associated with the severity of luminal stenosis and p1aque ca1cification in coronary atherosc1erosis (26) and was associated with a significantly larger diameter and atheromatous burden as well as a higher leve1 of CRP in abdominal aornc aneUIγsms (27) 만1e mechanism of delayed enhancement is thought to be increased interstitial space
밍1d de1ayed contrast wash-out in tissues supplied by fme
microvessels (27,28). The blood f10w of the atherosclerotic plaque is mai띠.y supplied by the adventitial vasa vasorum and neoangiogenic microvessels from the vasa vasorum,and the necrotic core has abundant interstitial space. Therefore, the enhancement of the outer wall and soft plaque is probably representatιve of de1ayed enhancement. In 야llS study,CTdelaywas the optimal phase for the detection and delineation of soft plaque and the enhancement of the outer wal1. The difference in CTHUs between soft plaque and outer wall was progressive1y increased through TPCT and was greatest on CTd뼈,and this 1arge CTHUs difference on
CT,’,.,IIll양1t grant better soft tissue contrast and higher
detection rate of the CAP to CTdeμyunages
It has been sh
。、
iVDthat the degree of neoangiogenesis can be assessed by qu밍1titative or semiquantitative analysis ofthe enhancemeht pattern in the outer wall of the carotid
없terγ in DCE→MRI and CTA studies (24,29),According 1D
these res버t.s,it wc띠d be possible to detennine whether the
plaque is vulnerable by analyzing the enhancement pattern
。
f the outer wal1. In our study,outer wall enhancement showed a similar pattern to that in the previous DCE- MRI study and sh。、
iVed progressive and delayed enhancement regard1ess of symptomatology or degree of stenosis; h。、
iVever,감1e degree of contrast enhancement in the outer wall was not significantly different between symptomatic 없1dasymptomatic arteries. When symptomatic arteries or arteries with stenosis greater than 70%
、
iVere grouped together,the degree of enhancement in the outer w'때l、
Ilas significant1y greater than that in asymptomatic arteries with stenosis of 1ess than 70%. Symptαnato1ogy is a clinical criterion and is dependent on the time point of the events: in contrast,the vu1nerability of the p1aque is a pathological criterion 잉1d is dependent on histologica1 characteristics(30),Asymp1Dmalic앙ieries with severe stenosis of greater
than 70% in our study might have had the features of vulnerable plaque,which might have affected the statistical result.s 01' the groups according to the symptomato1ogy. In the previous DCE-MRI and CTA studies,the pattern of contrast enhancement was significantly different for the group with the symptomatic or severe stenotic arteries together but not in야1e pure symptomatic group (24,29). In
。
ur study, the CTHUs of soft plaque on CT“"π、
iVere SI망파ìcantly hi양1er in symptomatic arteries and arteries with stenosis greater than 70% than that in asymptomatic arteries with stenosis less than 70%. In previous report of coronarγ arteries,vulnerab1e plaque had significantly greater iron deposition from the extravasated erγthrocytes and greater macrophage infiltration compared to plaque with early-stage CAP,which was presumed to be due to repeated microhem。
πhage from 1eaky microvessels within CAP(31l. The higher CTHUs of soft plaque in symp1Dma디Cand severe stenotic arteries in our study may reflect the presence of repeated rnicrohem
。
π'hageOur studv has several limitations. This study was based on a small sample group vrithout histological correlation. We did not roulinely apply TPCT 10밍I CTA sludies due 10 the problem of additional radiation. The lens of the eye is a radiation- sensitive organ. For radiation dose reduction t
。
the lens,we caìl use bismuth eye shielding or special CT algorithm for dose reduction such as angWar tube cwrent modulation and automatic z-axis dose modulation (32-34) In this study,the CTIWs of the soft plaque and outer wall were measured in only one location per slice by drawing the ROI manu외lγ Measurement by manual ROI may be accurate if the ROI is drawn at the exact lesion site; however,the reproducibility may be inferior to automatic or semiautomatic ROI measurementIn conclusion , CTdelaywas the optimal phase for the detection and characterization of the CAP components. CAP components showed progressive and delayed enhancement
。
n TPCT, and the outer wall showed more prominent enhancement than soft plaque. CTHUs of the outer w머1 on CTde!oYand soft plaque on CTarteηwere significan이y higher insymptomatic or severely stenotic arteries
[ References
1) Autret A,Pourcelot 1 ,Saudeau D,March외 C,Berlrand
P,de Boisvillîers S. Stroke risk in patienís with c강olid
s!enosis,Lancet 1987:1:888-890
2) Meissner 1,Wìebers DO,Whisnant JP ,O'Fallon vrM. The natural histαγ
。
f asymptomatic c않。
lid arterγ occlusive lesions. J따!lA 1987:258:2704-27073) Dennis MS,Bamford JM ,Sandercock PA,Warlow CP,A comparison of risk factors and prognosis for transient ischemic attacks and minor ischemic strokes. The Oxfordshire Community Stroke Project. Stroke 1989:20:1494-1499
4) Rigamonti D,Johnson PC,Spetzler RF,Hadley MN, Drayer BP. Cavernous malformations and capillary telangiectasia: a spectrum within a single pathol。밍cal en며ty,Neurosurgery 1991:28:60-64
5) Endarterectomy for asymptomatic carotid artery stenosis Executive Committee for the Asymptomatic Carotid Atherosclerosis Sludy,JAMA 1995:273:1421-1428
6) Rothwell PM,Eliasziw M,Gutnikov SA,Fox AJ,Taylor DW,Mayberg :tvffi,et a1. Analysis of pooled data from the randomised contr'olled trials of endarterectomy for symptαnatic carotid stenosis. Lancet 2003:361:107-116 7) Glagov S,Weisenberg E ,Zarins CK,Stankunavicius R,
Kolettis GJ. Compensatory enlargement of human
Evaluation of Carotid Atherosclerosis using Three-Phase CT1
atheroselerotie eoronary arteries. N Engl J Med 1987:316:1371-1375
8) Ambrose JA,Tannenbaum :tv1A,A1exopoulos D,Biemdahl Monsen CE,1eavy J,Weiss M,et a1. Angiographic progression of eoronary artery disease and the development of myoeardial infaretion. J Am Co11Cardiol 1988:12:56-62
9) Moreno PR,Falk E ,Palaeios IF,Newe11 JB ,Fuster V, Fallon JT. Macrophage infiltration in acute coronary syndromes. Implieations for plaque rupη미re. Circulati.on
1994:90:775-778
10)Moreno PR,Bernardi VH,1opez-Cuellar J,Murcia AM, Palaeios IF,Gold Hlζ et al. Maerophages ,smooth musc1e eells,and tissue faetor in tU1Stab1eangina. Implieations for eell-mediated thrombogenicity in aeute coronary syndromes. Circula디on 1996:94:3090-3097
11)Jander S,Sitzer M,Schumarm R,Sehroeter M,Sieb1er M, Steinmetz H,et al. Inflammation in high-grade earotid stenosis: a possible role for macrophages and T cells in plaque destabilization. 8troke 1998;29:1625-1630
12)Spagnoli 1G,Mauriello A,Sangiorgi G,Fratoni S, Bonanno E, Sehwartz RS, et a1. Extraeranial thrombotically aetive earotid plaque as a risk faetor for ischemic slroke,JAMA 2004:292:1845→1852
13) Sa잉n T,Hats따‘ami TS,Takaya N,Chu B,Underhill H, Kerwin WS,et a1. The vulnerable ,or high-risk , atheroselerotie plaque: noninvasive MR imagin~ for charaeterization and assessment. Radiolo양 2007:244:64-77
14)Yuan C,.Mitsumori 1M,Beaeh KW,Maravilla KR. Carotid atherosc1erotic plaque: noninvasive .tV1Reharaeterization and identifieation of vulnerable lesions. Radiology 2001:221:285-299
15)Chu B,Kampsehulte A,Ferguson MS,Kerwin WS, Yarnykh VL,0’Brien KD,et a1. Hemorrhage in the atherosclerotic earotid plaque: a high-resolution 11RI sludy,Slroke 2004:35: 1079-1084
16)Trivedi RA,Mallawarachi C,JM UK-I ,Graves MJ, Horsley J,Goddard MJ,et 려 Identifying inf1amed carotid plaques using in vivo USPIO-enhanced :tvffiimaging t
。
labe1 plaque maerophages. Arterioscler η1fomb Vasc Biol 2006:26:1601-16061끼Tang TY,Howarth SP ,Miller SR,Graves MJ,JM UK-I , 1i ZY,et al. Correlation of caroti.d atheromatous plaque inflammation using USPIO-enhaneed :MR imag끄19 with degree of luminaI s!enosis,Slroke 2008:39:2144-2147
18) de Weert 'IT,Ouhlous M,Mei,iering E,Zondervan PE , Hendriks JM,van Sambeek MR, et a1. In viv
。
charaeterization and quantification of atheroscleroticIn Young Kim,Sun Young J eong. Ji Kang Park
carotid. plaque components wi바1 multidetector computed tomography and histopathological coπelation. Aπerioscler Thromb Vasc Bìol 2006:26:2366-2372
19)Wìntermark M,Jawadi SS,Rapp 따i,Tìhan T,Tong E, Glidden DV,et a1. High-resolution CT imaging of earotid arteη atherosclerotic plaques. AJNR Am J Neuroradiol 2008:29:875-882
20) de Boer OJ,van der Wal AC,Teeling P ,Beeker AE 1eueoeyte reeruitment in rupture prone regions of lipid rieh plaques: a prominent r
‘。
le for neovascularization? Cardiovasc Ras 1999:41:443-44921) MeCarthy MJ,10ftus 1M,Thompson MM,Jones 1, 1ondon NJ,Bell PR,et. a1. Angiogenesis and the atherosclerotie carotid plaque: .an association betWeen symptomatology and plaque morphology. J Vase Surg 1999:30:261-268
22)Virmanì
요
Kolodgie FD,Burke AP,Fìnn AV,Gold HK, Thle마‘o 'IN,et 81. Atherosclerotic plaque progression and vulnerability to rupture: angiogenesis as a source of intraplaque hemorrhage. Arterioscler 'Thromb Vasc Biol 2005:25:2054-206123) Kerwin WS,O'Brien KD,Ferguson M3,Polissar N, Hatsukami TS,Yuan C. Inf1ammation in carotid atherosclerotic plaque: a dynamic contrast-enhaneed :MR imaging study. Radiology 2006:241:459-468
24) Kerwin WS,Oikawa M,γùan C,Jarvik GP,Hatsukami TS. :MR imaging of adventiti81 vasa vasorum in carotid atheros이erosis. Magn Reson Med 2008:59:507-514
25) Aoki S,Aoki K,Obsawa S,N따mjima H,Kumagai H,
Araki T. Dynamic :MR imaging of the carotid w81l. J Magn Reson Imaging 1999;9:420-427
26)Yeon SB,Sabir A,Clouse M,M앙tinezclark PO,Peters DC, Hauser TH, et a1. Delayed-enhancement eardiovase 띠ar rnagnetic resonance coronary 양iery wall imaging: comparison with multislice computed tomography and quantitative coronarγ angiograpby. J Am Coll C와diol 2007:50:441-447
27) 3akuta A,Kimura F ,Aoka Y,Aomi 3 ,Hagiwara N, Kasanuki H. Delayed enhancement on computed tomography in abdominal aortic aneurysm wal1. Heart Vessels 2007:22:79-87
28) Kleìn C,Scbmal TR,Nekolla SG,Scbnackenburg B,Fleck E,Nagel E. Mechanism of late gadolinium enhancement in patients with acute myocardi81 infaretion. J Cardiovasc Magn Reson 2007:9:653←658
29)Romero JM,Babiarz L8,Forero NP,Murphy EK, Schaefer PW,Gonzalez RG,et a1. Arterial wall enhancement overlying carotid plaque on CT 킹땅iographj correlates with symptoms in patients with high grade stenosis. Slroke 2009:40:1894-1896
30)Takaya N,Yuan C,Chu B,Saarn T,Underhill H,Cai J , et a1. Association between carotid plaque characteristics and subsequent ischemic cerebrovascular events: a prospective assessment with :MRl--initial results. 8troke 2006:37:818-823
31) Kolodgie FD,Gold HK,Burke AP,Fowler DR,Kruth HS, Weber DK, et a1. Intraplaque hemorrhage and progression of coronary atheroma. N Engl J Med 2003:349:2316-2325
32) Ryu CW,Kim JK ,Kim SJ ,1ιee JH ,Kim따"Ha Jll,et al Head and neck vascular lesions: characterization of the
n。、
N pattem by 야1e use of three-phase CT. Korean J Radiol 2009:10:323-33233) Namasivayam S,Kalra :MK,Pottala KM,Waldrop 3M , Hudgins PA. Optimization of Z-axis automatic exposure control for multi.detector row CT ev81uation of ne얘 and comparison with fJxed tube current technique for image quality and radiation dose. AJNR Am J Neuroradiol 2006:27:2221-2225
34) van Slraten M,Deak P ,Shrimpton PC ,Kalender WA. The effect of angular and longitudinal tube current modulations on the estimation of organ and effective doses in. x-ray eomputed tomography. Med Phys 2009:36:4881-4889