저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
1
The association between testosterone and
muscle mass, muscle strength, and physical
function in Korean men aged 60 and older
by
Sohyun Oh
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
2
The association between testosterone and
muscle mass, muscle strength, and physical
function in Korean men aged 60 and older
by
Sohyun Oh
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements
for the Degree of
Master of Medicine
Supervised by
Kwang-Min Kim, M.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
3
This certifies that the dissertation
of Sohyun Oh is approved.
SUPERVISORY COMMITTEE
Kwang-Min Kim
Sat-Byul Park
Bom-Taeck Kim
The Graduate School, Ajou University
December, 14th, 2012
4
-ABSTRACT-
The association between testosterone and muscle mass, muscle
strength, and physical function in Korean men aged 60 and older
Background: Ageing in men is associated with decline in serum testosterone level. Previous studies have shown that low testosterone level is an important cause of sarcopenia which contributes to development of frailty in elderly men. Sarcopenia was defined by low muscle mass in prior studies. However this study is to see the association between serum testosterone level and sarcopenia according to the new sarcopenia definition which considers not only muscle mass, but also muscle strength and gait speed in Korean men aged 60 years and older.
Method: Cross-sectional observational study of 161 participants who underwent routine check-up at Ajou University Hospital Health Promotion Center from March 1st, 2011 to
September 30th, 2012. Participants were community-dwelling healthy men aged 60 years and older. Outcome measures include muscle mass using dual energy X-ray absorptiometry (DXA), muscle strength by grip strength and physical performance by gait speed. Hypogonadism was defined by serum testosterone level of less than 350ng/dL. Muscle mass was calculated with appendicular skeletal muscle (ASM) by height square or weight. Results: Serum testosterone had significant relationship with muscle mass (ASM adjusted for body weight: p=0.023). However, serum testosterone had no significant relationship with muscle mass (ASM adjusted for height square: p=0.132), muscle strength (p=0.773), and gait
5
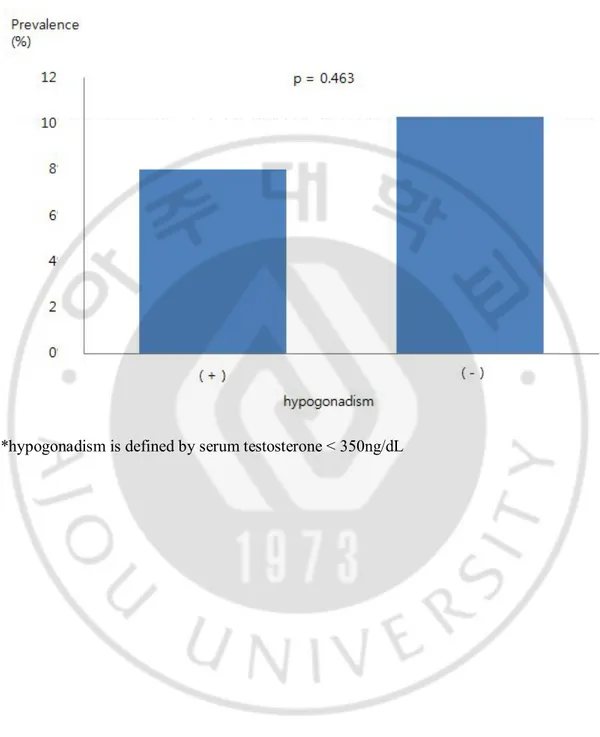
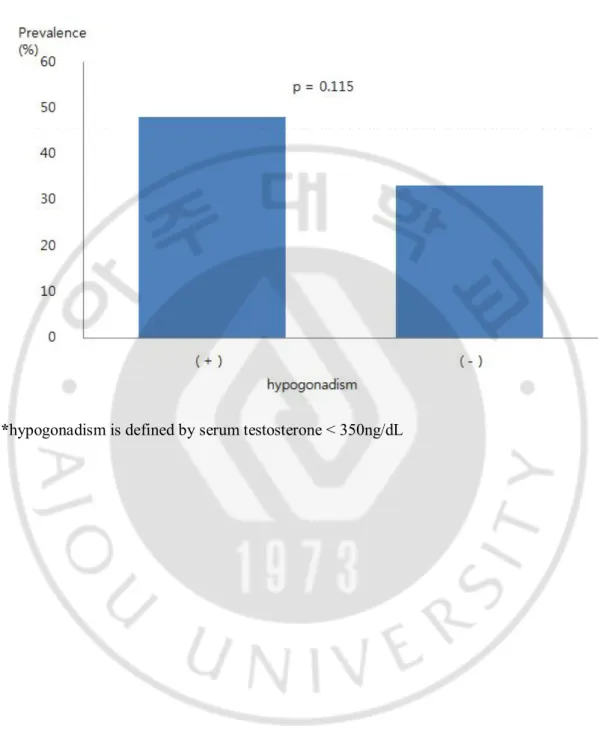
speed (p=0.201). Subjects were divided into quartiles according to serum testosterone level, which had no significant relationship with muscle mass (ASM/ht²: p=0.224, ASM/wt: p=0.169), muscle strength (p=0.100), and gait speed (p=0.064). Hypogonadism did not show significant relationship with sarcopenia defined by ASM/ht² (p=0.463) nor by ASM/wt (p=0.115).
Conclusion: Decreased serum testosterone has little predictive value of functional impairment represented by muscle mass adjusted by height (ASM/ht2), muscle strength, and
gait speed. However, muscle mass adjusted by body weight (ASM/wt) had significant relationship with serum testosterone.
Key words: testosterone, hypogonadism, muscle mass, muscle strength, gait speed, sarcopenia.
6
TABLE OF CONTENTS
ABSTRACT --- i
TABLE OF CONTENTS ---iii
LIST OF TABLES ---iv
LIST OF FIGURES---v I. INTRODUCTION ---6 II. METHOD---8 A. Study Participants---8 B. Measurements ---8 C. Statistical analysis ---10 III. RESULT ---11 IV. DISCUSSION ---22 V. CONCLUSION ---25 REFERENCES---26 국문요약 ---29
7
LIST OF TABLES
Table 1. General characteristics of the study population---13
Table 2. Serum testosterone level according to age groups ---14 Table 3.Serum testosterone level and muscle mass (ASM/ht2, ASM/wt), grip strength, gait
speed in older men by linear regression ---15
Table 4. Serum testosterone level in quartile and muscle mass (ASM/ht2, ASM/wt), grip
8
LIST OF FIGURES
Figure 1. Serum testosterone level and muscle mass adjusted by weight (ASM/wt) in elderly men ---17 Figure 2. The prevalence of sarcopenia defined by by ASM/ht2 according to hypogonadism in
elderly men ---18 Figure 3. The prevalence of sarcopenia defined by ASM/wt according to hypogonadism in elderlyl men ---19
Figure 4. The prevalence of sarcopenia defined by EWSGOP guideline, muscle mass
adjusted by height according to hypogonadism in elderly men---20
Figure 5. The prevalence of sarcopenia defined by EWSGOP guideline, muscle mass
9
I. Introduction
Sarcopenia is a syndrome characterized by progressive and generalized loss of skeletal muscle mass and strength with risk of adverse outcomes such as physical disability, poor quality of life and death.(Cruz-Jentoft et al., 2010) The EWGSOP recommends using the presence of both low muscle mass, low muscle strength, and low physical performance to diagnose sarcopenia.(Cruz-Jentoft et al., 2010) There are several mechanisms that involve in the onset and progression of sarcopenia which include protein synthesis, proteolysis, neuromuscular integrity and muscle fat content.
In an individual with sarcopenia, several mechanisms may be involved, and relative contributions may vary over time. In some individuals, a clear single cause of sarcopenia can be identified. In other cases, no evident cause can be isolated. Sarcopenia can be considered ‘primary’ (or age-related) when no other cause is evident but ageing itself. Prior studies have shown that testosterone level decline with aging, and this is associated with sarcopenia. However, there were some conflicting studies that showed testosterone level did not fall significantly with age in healthy men. (Kim et al., 2012a)
Over the last few years there has been a serious effort to define and operationalize clinical and biochemical characteristics of the testosterone deficiency syndrome. (Valenti et al., 2002) As a result, specific symptoms associated with low serum testosterone level in older people may negatively affect the quality of life and contribute to deterioration of function of organs and systems. (Bhasin et al., 2006) Main characteristics include decrease of libido, carbohydrate metabolism disorders, sarcopenia and adverse changes in mood and cognition. (Maggio et al., 2011) In cross-sectional and longitudinal studies, lower sex hormone levels are associated with greater dependency, impaired balance, and falls, whereas
10
higher levels are associated with better performance of activities of daily living. (Szulc et al., 2003; Schaap et al., 2005)
It is known that age-related declines in strength and muscle mass are highly correlated with each other. (Kallman et al., 1990) However, measuring “muscle quality” as strength per unit of muscle mass may be an independent indicator of muscle performance useful in understanding age-related changes in skeletal muscle.(Kallman et al., 1990; Frontera et al., 1991; Metter et al., 1999) Also observational and interventional data show that higher sex hormone levels improve body composition, including increasing lean mass and decreasing fat mass. (Araujo et al., 2008) Improvements in body composition should have downstream influences on measures of physical performance and function, given their known association with muscle strength. However, there are limited data on the effect of sex hormone on physical function on racially and ethnically diverse men.
The aim of this study is to determine the association between serum testosterone level and muscle mass, muscle strength, physical performance in elderly Korean men aged 60 and older.
11
II. Method
A. Study participants
330 participants underwent routine check-up at Ajou University Hospital Health Promotion Center from March 1st, 2011 to September 30th, 2012. Female participants were
all excluded (147 participants). Participants with systemic conditions that would have effect on muscle strength and physical function (22 participants) were excluded. The excluded conditions were cerebrovascular disease, rheumatologic disease. Total of 161 men were included in the study. The age ranged from 60 years old to 84 years old. All subjects gave informed consent and all the information in the study was approved by the institutional review board.
B. Measurement
Blood samples were collected during first visit between 8AM~10:30AM to minimize circardian variation. Samples were analyzed by radioimmunoassay. The subjects were divided into quartiles according to the level of serum testosterone. According to the baseline serum testosterone level, subjects were divided into two groups: <350ng/dL as hypogonadal status, ≥350ng/dL as normal. (Maggio et al., 2011)
Appendicular skeletal muscle mass (ASM) was measured by dual energy X-ray absorptiometry (DXA). ASM was calculated by the summation of muscle mass measured in the upper limb and lower limb. Muscle mass was corrected for body sizing by dividing the ASM with square of height and weight. We defined sarcopenia according to the recent sarcopenia prevalence study. According to the definition proposed in the previous studies,
12
sarcopenia was divided into normal, class I sarcopenia, class II sarcopenia. Individuals of whom height-adjusted and weight-adjusted ASM were higher than 1 SD below the gender-specific mean for young reference group were considered normal. Class I sarcopenia was indicated by the definition in participants whose height-adjusted and weight-adjusted ASM was from 1 to 2 SD below the mean for young adults. Class II sarcopenia was indicated by definition in participants whose height-adjusted and weight-adjusted ASM was below 2 SD (cutoff value was 6.58kg/m2 for height-adjusted, 29.1% for weight adjusted). (Kim et al.,
2012b)
Muscle strength was assessed by using handgrip strength. Although lower limbs are more relevant than upper limbs for gait and physical function, prior studies have shown that handgrip strength is well correlated with muscle strength. Grip strength was measured using both hands. The stronger side of hand grip strength was used as a representation
measurement. Isometric hand grip strength is strongly related with lower extremity muscle power, knee extension torque and calf-cross sectional muscle area. (Lauretani et al., 2003) Low handgrip strength is a clinical marker of poor mobility and a better predictor of clinical outcome than low muscle mass. (Lauretani et al., 2003) In clinical practice, there is also a linear relationship between baseline handgrip strength and incident disability for activities of daily living (ADL). (Al Snih et al., 2004) We used the cutoff value of low handgrip strength from the study done by Soo-hong Han et al using the cutoff value of average of 234 Korean healthy men in 20s and 30s. The cutoff value was 32.82kg.
Physical performance was assessed by gait speed. Gait speed is a part of short physical performance battery (SPPB), but it can also be used as a single parameter for clinical practice. Gait speed was measured by timing the speed of going 2 meters. We used
13
the cut-off value of low gait speed suggested in the study done by S. H. Cho et al which was 0.87m/s. (Cho et al., 2004)
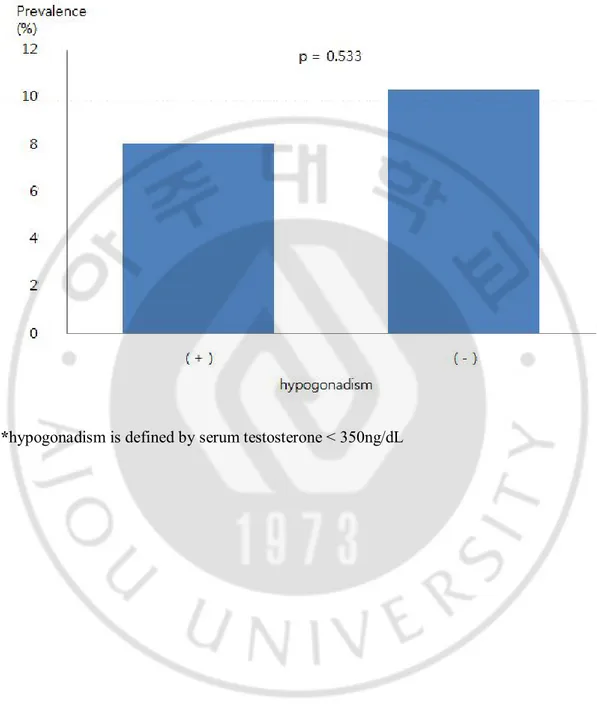
We diagnosed sarcopenia according to EWGSOP guideline by using the presence of low muscle mass and 1 of either low grip strength or gait speed. The rationale for using 2 criterion out of 3 is defining sarcopenia only in terms of 1 criteria may be of limited clinical value.
C. Stastical analysis
Variables are shown as mean values ± standard deviations (SD) or number and percentages. To test the relationship between serum testosterone level (independent variable) and 3 criterion: muscle mass, grip strength, gait speed (dependent variables), we used linear regression. We also performed two additional statistical analysis by dividing the independent variable according to the level of serum testosterone. First was to test the relationship between the quartiles of serum testosterone level and muscle mass, grip strength, gait speed by using ANOVA. Second was to determine the relationship between the presence of sarcopenia and serum testosterone level by using chi-square test.
We considered p<0.05 to be statistically significant. All statistical analyses were performed using SPSS 19.0(IBM, NY, USA).
14
III. Result
The mean age of the study population is 65.3 years. The mean serum testosterone level is 513ng/dL. The prevalence of sarcopenia according to muscle mass adjusted by height is 23%, sarcopenia according to muscle mass adjusted by weight is 35%, sarcopenia defined by EWGSOP guideline and muscle mass adjusted by height is 9.9%, and sarcopenia defined by EWGSOP guideline and muscle mass adjusted by weight is 14.9%. (Table 1)
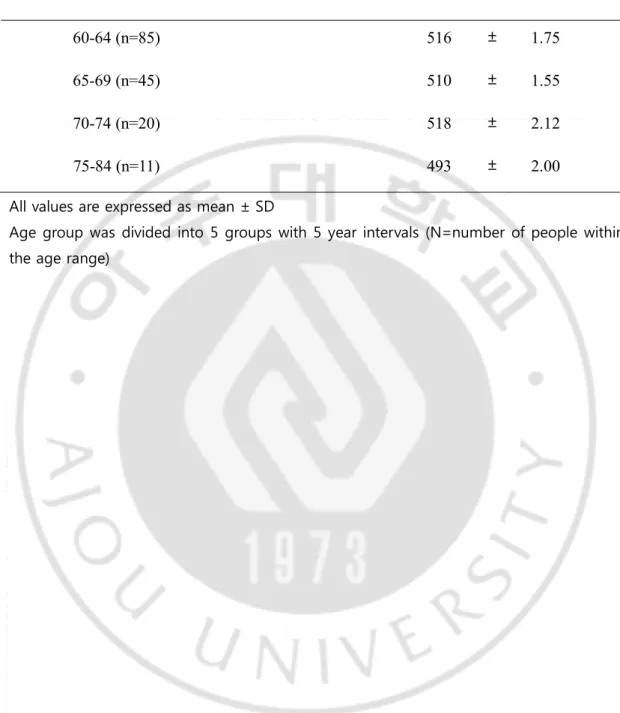
There was no significant difference between the levels of serum testosterone
according to age groups. Serum testosterone level of age group of 60-64 years was 516(±175) ng/dL and 75-84 years was 493(±200) ng/dL. These two groups showed no significant difference. (Table 2)
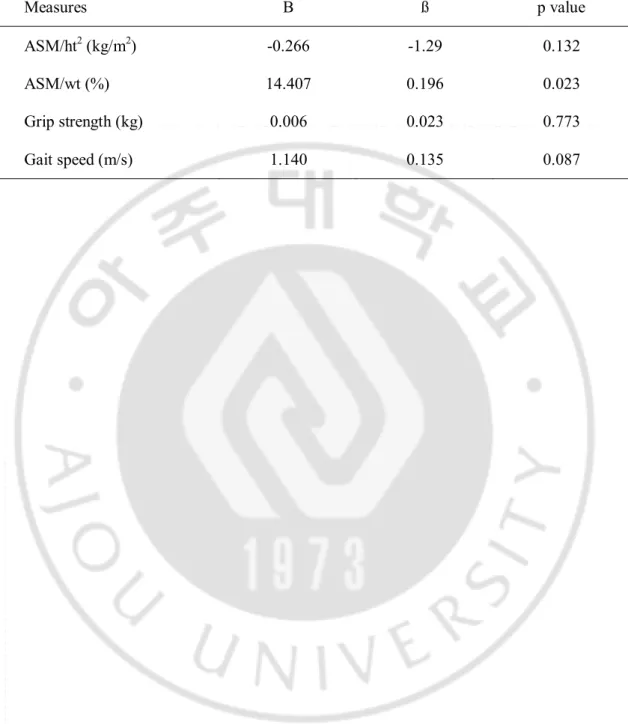
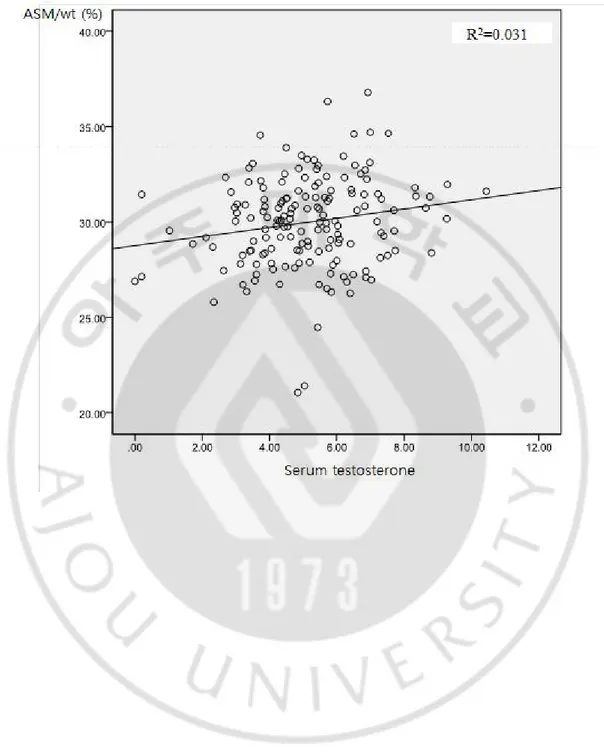
The level of serum testosterone had significant relationship with muscle mass (ASM/wt: p=0.023), but was not statistically significant with muscle mass (ASM/ht2:
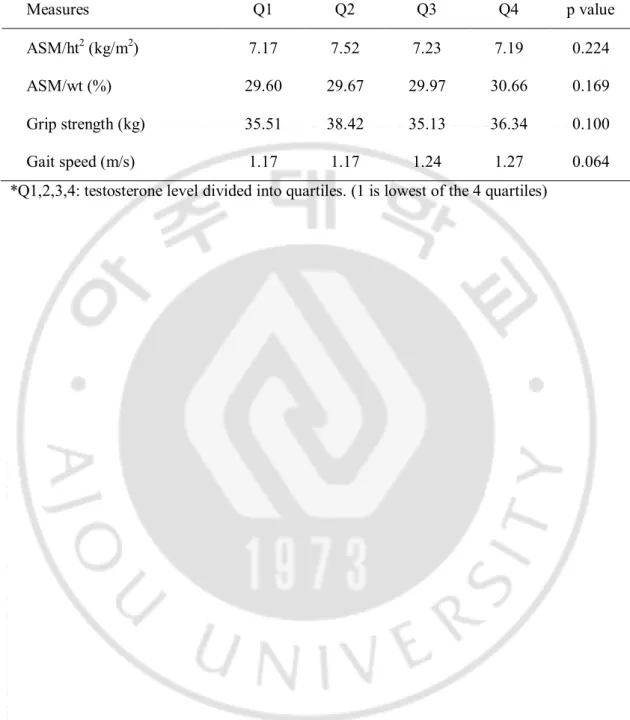
p=0.132), muscle strength (p=0.773), and gait speed (p=0.201). (Table 3, Figure 1) Dividing the subjects into quartiles by serum testosterone level and testing the correlation between muscle mass (ASM/ht2: p=0.224, ASM/wt: p=0.169), muscle strength
(p=0.100), and gait speed (p=0.064) were found to have no significant relationship. (Table 4) Our study showed significant relationship between serum testosterone level and muscle mass adjusted by weight (ASM/wt) but no significant relationship between serum testosterone and muscle mass adjusted by height square (ASM/ht2)
There was no significant difference between the level of serum testosterone level and presence of sarcopenia by using chi-square test. The diagnosis of sarcopenia was done by using the cutoff vales written on the method above. Serum testosterone level and
15
sarcopenia defined by muscle mass (ASM/ht2, ASM/wt) by chi square is shown in Figure 1
and 2 which showed no significance. Serum testosterone level and sarcopenia defined by EWGSOP guideline (presence of sarcopenia: 2 out of 3 criterion) by chi square is shown in Figure 3 and 4 which also showed no significance.
16
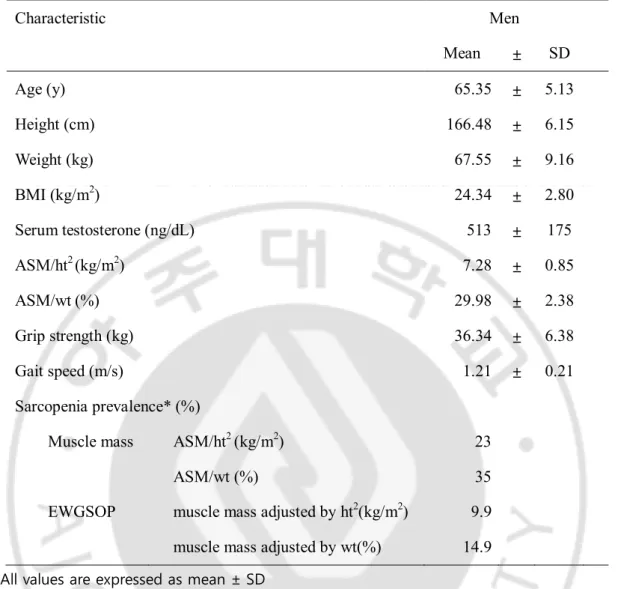
Table 1. General characteristics of the study population (N=161)
Characteristic Men Mean ± SD Age (y) 65.35 ± 5.13 Height (cm) 166.48 ± 6.15 Weight (kg) 67.55 ± 9.16 BMI (kg/m2) 24.34 ± 2.80 Serum testosterone (ng/dL) 513 ± 175 ASM/ht2 (kg/m2) 7.28 ± 0.85 ASM/wt (%) 29.98 ± 2.38 Grip strength (kg) 36.34 ± 6.38 Gait speed (m/s) 1.21 ± 0.21 Sarcopenia prevalence* (%)
Muscle mass ASM/ht2 (kg/m2) 23
ASM/wt (%) 35
EWGSOP muscle mass adjusted by ht2(kg/m2) 9.9
muscle mass adjusted by wt(%) 14.9
All values are expressed as mean ± SD
SD= standard deviation, BMI= body mass index = weight / height2, ASM= appendicular
skeletal muscle = upper limb muscle mass + lower limb muscle mass, ht2= height x
height, wt= weight, EWGSOP = European Working Group on Sarcopenia in Older People * sarcopenia prevalence: sarcopenia defined by muscle mass (adjusted by height and weight) and sarcopenia definition by EWGSOP guideline.
17
Table 2. Testosterone level according to age groups. (p=0.963)
Age (yrs) Testosterone (ng/dL)
Mean ± SD
60-64 (n=85) 516 ± 1.75
65-69 (n=45) 510 ± 1.55
70-74 (n=20) 518 ± 2.12
75-84 (n=11) 493 ± 2.00
All values are expressed as mean ± SD
Age group was divided into 5 groups with 5 year intervals (N=number of people within the age range)
18
Table 3. Serum testosterone level and muscle mass (ASM/ht2, ASM/wt), grip strength, gait
speed in older men by linear regression
Measures B ß p value
ASM/ht2 (kg/m2) -0.266 -1.29 0.132
ASM/wt (%) 14.407 0.196 0.023
Grip strength (kg) 0.006 0.023 0.773
19
Table 4. Serum testosterone level in quartile and muscle mass (ASM/ht2, ASM/wt), grip
strength, gait speed in older men by ANOVA
*Q1,2,3,4: testosterone level divided into quartiles. (1 is lowest of the 4 quartiles)
Measures Q1 Q2 Q3 Q4 p value
ASM/ht2 (kg/m2) 7.17 7.52 7.23 7.19 0.224
ASM/wt (%) 29.60 29.67 29.97 30.66 0.169
Grip strength (kg) 35.51 38.42 35.13 36.34 0.100
20
Figure 1. Serum testosterone level and muscle mass (ASM/wt) in older men by linear regression (p=0.023)
21
Figure 2. The prevalence of sarcopenia defined by ASM/ht2 according to hypogonadism in
elderly men.
22
Figure 3. The prevalence of sarcopenia defined by ASM/wt according to hypogonadism in elderly men.
23
Figure 4. The prevalence of sarcopenia defined by EWGSOP guideline, muscle mass adjusted by height square according to hypogonadism in elderly men.
24
Figure 5. The prevalence of sarcopenia defined by EWSGOP guideline, muscle mass adjusted by weight according to hypogonadism in elderly men.
25
IV. Discussion
In a representative sample of older Korean men, we found significant relationship between serum testosterone and muscle mass adjusted by weight (ASM/wt). However, there was no significant relationship between serum testosterone level and muscle mass adjusted by height square (ASM/ht2), muscle strength, and gait speed. Also, there was no
significance between the quartile of testosterone nor hypogonadism (serum testosterone <350ng/dL) with the 3 criterion above.
In previous studies, it has been proven that testosterone affects muscle function and quality. (Ferrando et al., 2002) Several other randomized controlled studies conducted with testosterone in men show a direct effect of this hormone on muscle strength, in hypogonadal and frail elderly men. (Coviello et al., 2008; Onder et al., 2009; Srinivas-Shankar et al., 2010) A recent meta-analysis including data from 11 randomized-clinical trials suggests that, in older men, testosterone therapy produced a moderate increase in muscle strength compared with placebo. (Ottenbacher et al., 2006) However, testosterone administration did not improve leg muscle fatigability. Healthy older men experienced no detectable improvements in performance-based measures of physical function such as walking, climbing stairs, or rising from a chair and walking a distance after receiving supraphysiological doses of testosterone that induced substantial gain in skeletal muscle mass and maximal voluntary strength. According to another study reported by Storer et al., the relationship between testosterone and muscle strength does not imply an immediate effect on physical function. (Buchner et al., 1996)
In our study, we used both ASM adjusted by height square and ASM adjusted by weight. According to recent studies, ASM adjusted by weight may be more appropriate
26
method in defining sarcopenia, especially in the Korean population. (Kim et al., 2012b) Weight-adjusted definition was more closely associated with metabolic syndrome. Though height-adjusted ASM has been regarded as a good index of relative skeletal muscle mass, it showed poor correlation with age-related muscle mass loss. Prevalence of sarcopenia is very low by the height-adjusted definition and high among sarcopenic participants by the weight-adjusted definition. As we can see from our data, serum testosterone level showed significant correlation with ASM adjusted by weight but not with ASM adjusted by height square.
Sarcopenia definition was mainly based only on muscle mass. However, the strong point of our study is that we saw the association between serum testosterone level and
sarcopenia according to the new sarcopenia definition which considers not only muscle mass, but also muscle strength and gait speed. This definition is a better index to see the overall physical function of the elderly. However, our study was done with a group of relatively healthy young aged group compared to other studies. Mean age of the population was 65.35(±5.13) years old. Other studies were done with older age group which included more participants with very old men (age of 80 years and older). To represent more frail elderly men, the mean age of our study should have been older to generalize the population.
Neuromuscular adaptations play an important role in improvements in function during resistance exercise training. [24] Others have suggested that the translation of strength gains into improvements in physical function may require cognitive, behavioral, or
functional training. (Latham et al., 2004) A systematic review of the effectiveness of progressive resistance strength training in older adults revealed that resistance exercise training may need to be combined with functional or behavioral training to translate strength gains into functional improvements. (Latham et al., 2004) Thus, there could be other factors
27
that have greater effect than testosterone on muscle and physical function that need to be further investigated.
Our study has some limitations. This is a preliminary analysis with a cross-sectional design and therefore no causality can be determined. First, the age range of the subject group was younger than what we initially anticipated. In order to see the low testosterone effect on elderly healthy men, we should have had more subjects with older age. Second, the cutoff value used in our study may be inaccurate due to values from different studies. It would have been more accurate if we used a cut off value using a control group value from our own study. Third, muscle strength was only measured with grip strength and physical
performance was only measured with gait speed. In addition to muscle strength and power, there are other determinants of performance in physical tasks. There is a need of
longitudinal study of older age group to determine a more accurate correlation between testosterone level and muscle mass, muscle strength, and physical function.
28
V. Conclusion
In older Korean men, testosterone level had little predictive value of functional impairment related to muscle mass(ASM/ht2), muscle strength, and gait speed except for muscle mass (ASM/wt).
29
VI. References
1. Al Snih S, Markides KS, Ottenbacher KJ, Raji MA: Hand grip strength and incident ADL disability in elderly Mexican Americans over a seven-year period. Aging Clin Exp Res 16: 481-486, 2004
2. Araujo AB, Travison TG, Bhasin S, Esche GR, Williams RE, Clark RV, McKinlay JB: Association between testosterone and estradiol and age-related decline in physical function in a diverse sample of men. J Am Geriatr Soc 56: 2000-2008, 2008
3. Baumgartner RN, Waters DL, Gallagher D, Morley JE, Garry PJ: Predictors of skeletal muscle mass in elderly men and women. Mech Ageing Dev 107: 123-136, 1999
4. Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM: Testosterone therapy in adult men with androgen deficiency syndromes: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 91: 1995-2010, 2006
5. Buchner DM, Larson EB, Wagner EH, Koepsell TD, de Lateur BJ: Evidence for a non-linear relationship between leg strength and gait speed. Age Ageing 25: 386-391, 1996
6. Cho SH, Park JM, Kwon OY: Gender differences in three dimensional gait analysis data from 98 healthy Korean adults. Clin Biomech (Bristol, Avon) 19: 145-152, 2004
7. Coviello AD, Kaplan B, Lakshman KM, Chen T, Singh AB, Bhasin S: Effects of graded doses of testosterone on erythropoiesis in healthy young and older men. J Clin Endocrinol Metab 93: 914-919, 2008
8. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinkova E, Vandewoude M, Zamboni M: Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 39: 412-423, 2010
9. Ferrando AA, Sheffield-Moore M, Yeckel CW, Gilkison C, Jiang J, Achacosa A, Lieberman SA, Tipton K, Wolfe RR, Urban RJ: Testosterone administration to older men improves muscle function: molecular and physiological mechanisms. Am J
30
Physiol Endocrinol Metab 282: E601-607, 2002
10. Frontera WR, Hughes VA, Lutz KJ, Evans WJ: A cross-sectional study of muscle strength and mass in 45- to 78-yr-old men and women. J Appl Physiol 71: 644-650, 1991
11. Kallman DA, Plato CC, Tobin JD: The role of muscle loss in the age-related decline of grip strength: cross-sectional and longitudinal perspectives. J Gerontol 45: M82-88, 1990
12. Kim YS, Hong D, Lee DJ, Joo NS, Kim KM: Total testosterone may not decline with ageing in Korean men aged 40 years or older. Clin Endocrinol (Oxf) 77: 296-301, 2012a
13. Kim YS, Lee Y, Chung YS, Lee DJ, Joo NS, Hong D, Song GE, Kim HJ, Choi YJ, Kim KM: Prevalence of Sarcopenia and Sarcopenic Obesity in the Korean Population Based on the Fourth Korean National Health and Nutritional Examination Surveys. J Gerontol A Biol Sci Med Sci, 2012b
14. Latham NK, Bennett DA, Stretton CM, Anderson CS: Systematic review of progressive resistance strength training in older adults. J Gerontol A Biol Sci Med Sci 59: 48-61, 2004
15. Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, Corsi AM, Rantanen T, Guralnik JM, Ferrucci L: Age-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol 95: 1851-1860, 2003
16. Maggio M, Ceda GP, Lauretani F, Bandinelli S, Metter EJ, Guralnik JM, Basaria S, Cattabiani C, Luci M, Dall'Aglio E, Vignali A, Volpi R, Valenti G, Ferrucci L: Gonadal status and physical performance in older men. Aging Male 14: 42-47, 2011 17. Metter EJ, Lynch N, Conwit R, Lindle R, Tobin J, Hurley B: Muscle quality and age:
cross-sectional and longitudinal comparisons. J Gerontol A Biol Sci Med Sci 54: B207-218, 1999
18. Onder G, Della Vedova C, Landi F: Validated treatments and therapeutics prospectives regarding pharmacological products for sarcopenia. J Nutr Health Aging 13: 746-756, 2009
19. Ottenbacher KJ, Ottenbacher ME, Ottenbacher AJ, Acha AA, Ostir GV: Androgen treatment and muscle strength in elderly men: A meta-analysis. J Am Geriatr Soc 54: 1666-1673, 2006
31
20. Schaap LA, Pluijm SM, Smit JH, van Schoor NM, Visser M, Gooren LJ, Lips P: The association of sex hormone levels with poor mobility, low muscle strength and incidence of falls among older men and women. Clin Endocrinol (Oxf) 63: 152-160, 2005
21. Srinivas-Shankar U, Roberts SA, Connolly MJ, O'Connell MD, Adams JE, Oldham JA, Wu FC: Effects of testosterone on muscle strength, physical function, body composition, and quality of life in intermediate-frail and frail elderly men: a randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab 95: 639-650, 2010
22. Szulc P, Claustrat B, Marchand F, Delmas PD: Increased risk of falls and increased bone resorption in elderly men with partial androgen deficiency: the MINOS study. J Clin Endocrinol Metab 88: 5240-5247, 2003
23. Valenti G, Bossoni S, Giustina A, Maugeri D, Motta M, Vigna GB, Fellin R, Corica F, Corsonello A, Paolisso G, Barbagallo M, Dominguez L, Denti L, Ceda G, Ferrari E, Pontiggia B, Strollo F: Consensus Document on substitution therapy with testosterone in hypoandrogenic elderly men. Aging Clin Exp Res 14: 439-464, 2002
32 - 국문 요약- 아주대학교 대학원 의학과 오소현 (지도교수: 김 광 민)
60세 이상 한국 남성에서의 테스토스테론과
근육량
, 근력, 및 보행속도와의 관계
배경: 연령의 증가와 혈중 테스토스테론의 농도의 감소는 연관이 있다. 이전 연 구에 따르면, 고령의 남성에서 노쇠를 일으키는 가장 큰 요소인 근감소증의 원인 으로 낮은 혈중 테스토스테론이 밝혀진 바 있다. 본 논문의 요지는 60세 이상 한 국 남성에서의 테스토스테론 수치에 따른 근육량, 근력, 보행속도와의 관계를 보 는 것이다. 방법: 2011년 3월부터 2012년 9월까지 아주대학교 병원 건강검진센터에서 건강검 진을 받은 161명의 건강검진 결과를 바탕으로 하였다. 근육량은 DXA, 근력은 악 력, 보생속도는 2m 거리를 주행하는데 걸리는 시간으로 측정하였다. 결과: 혈중 테스토스테론의 농도와 근육량 (ASM/ht2 : p=0.132, ASM/wt: p=0.023), 근력 (p=0.773), 보행속도 (p=0.201)의 연관성을 본 결과 몸무게로 보정한 근육량 값 이외에는 유의한 관련성을 보이지 않았다. 혈중 테스토스테론33 을 4분위로 나누어 다시 연관성을 살펴보았지만, 유의한 관련성을 보이지 않았 다. 성선저하증 (혈중 테스토스테론 <3.50ng/dL)도 유의한 연관성을 보이지 않 았다. 결론: 혈중 테스토스테론 농도의 감소는 근육량 (몸무게로 보정한 값) 이외에 근 육량(키로 보정한 값, 근력, 보행속도)의 예측 인자로 보기 어렵다. 중심 단어: 테스토스테론, 성선저하증, 근육량, 근력, 보행속도, 근감소증