대한외과학회지:제 69 권 제 6 호
□ 증 례 □
Vol. 69, No. 6, December, 2005
485 서 론
횡경막 탈장 중 식도 열공 탈장은 대부분 위가 위로 밀려
올라가 있으며, 증상은 형태에 따라 역류성 식도염을 비롯 하여 상부위장관의 천공, 출혈, 기계적 폐쇄 등 다양하게 나 타난다.(1) 저자들은 특별한 증세를 일으키지 않은 횡행결 장의 횡경막 탈장을 보인 환자에서 복강경을 이용한 수술 적 치료를 경험하여 보고하는 바이다.
증 례
환 자: 지○천, 28세, 남자
현병력: 신체검사 중 시행한 X-선 흉부촬영상 이상소견 보여 내원하였다.
과거력: 특이소견 없었다.
이학적 소견: 복부에 특이소견 없었으며, 좌하부 호흡음 이 감소되었으며, 장음이 청진되었다.
검사실 소견: 특이소견 없었다.
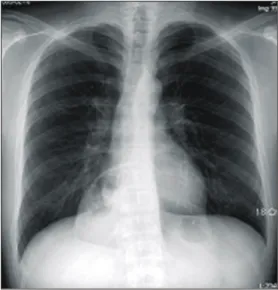
X-선 흉부촬영: 후종격동에 횡격막의 기초를 둔 비교적 경계가 분명한 경계를 가진 부채꼴 형태의 구조가 관찰되 었으며, 내부에는 공기음영을 포함하고 있었다(Fig. 1).
대장 조영 검사: 횡행 결장의 길이가 길었으며 중간 부분 이 흉곽 내로 밀려 올라간 소견을 보였다(Fig. 2).
횡격막 열공탈장의 복강경 수술
한양대학교 의과대학 구리병원 외과학교실 김 현 석․백 홍 규
Laparoscopic Repairing of Diaphragmatic Hernia
Hyun Seok Kim, M.D. and Hong Kyu Baek, M.D.
Hiatal hernias are usually classified into three distinct types:
type I, sliding hernias; type II, paraesophageal hernias; and type III, a combination of types I and II. Paraesophageal herniation is an uncommon disorder accounting for appro- ximately 5% of all hernias at the esophageal hiatus.
Laparoscopic repair of paraesophageal hernias is rapidly replacing the traditional open approach. However, several series have shown high recurrence rates due to the difficulty in closing the hiatal gap. A 28-year-old male patient pre- sented with no symptoms including reflux symptom, but a herniation of the transverse colon and omentum into the thorax to the right side of the esophageal hiatus of the diaphragm was found. The anatomy of the stomach and small bowel loops were unremarkable. After reduction of the colon and omentum, the defect was closed and reinforced using Prolene mesh via a laparoscopic procedure. The patient recovered early, with no complication, and has been recurrence free during the 8 months of followed up. (J Korean Surg Soc 2005;69:485-487)
Key Words: Hiatal hernia, Laparoscopy 중심 단어: 열공탈장, 복강경
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, College of Medicine, Hanyang University Kuri Hospital, Guri, Korea
책임저자: 백홍규, 경기도 구리시 교문동 249-1 ꂕ 471-701, 한양대학교 구리병원 외과 Tel: 031-560-2294, Fax: 031-566-4409 E-mail: hkbaik@hanyang.ac.kr
접수일:2005년 7월 7일, 게재승인일:2005년 10월 31일 본 논문의 요지는 2005년 대한외과학회 춘계학술대회에서 구연되 었음.
Fig. 1. Chest X-ray. Air-filled bowel shadow was seen in thoracic cavity.
486 대한외과학회지:제 69 권 제 6 호 2005
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 컴퓨터 단층 촬영: 횡경막의 식도열공의 우측을 통해 횡행
결장과 대망이 다량 흉곽 내로 탈장되어 있었다. 탈장된 부 분은 복막에 의해서 둘러싸여 가성 횡경막을 형성하고 있 는 것으로 보였다. 감돈이나 염전 등의 소견은 보이지 않았 다.
수술 소견 및 방법: 5 mm 투관침 1개와 10 mm 투관침 3개를 사용하여 복강경 수술을 시행하였다. 간좌엽을 견인 자로 젖히자 결손부가 보였으며, 감자를 사용하여 정복을 시작하였다. 정복시 탈장낭과 대망간에 약간의 유착이 있 어 박리를 하였다. 유착 박리를 마치자 식도 우측에 4×7
Fig. 2. Colon study. Transverse colon was herniated to thoracic cavity via paraesophageal hiatus.
Fig. 4. Follow up colon study. There was no abnormal findings and recurrence.
Fig. 3. Laparoscopic Operative find- ings and procedure. The colon and omentum, was reducted easily. The defect was closed by interrupt suture and rein- forced by prolene mesh which cover the suture line.
Liver
Defect
Esophagus
Stomach Mesh
김현석 외:횡격막 열공탈장의 복강경 수술 487 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ cm 크기의 큰 결손부가 보였다. 결손 부위의 좌우연을 poly-
glactin (VICRYLⓇ) 1-0를 사용하여 복강경용 직침기로 매듭 을 만든 후 knot pusher를 사용하여 5곳을 단속봉합하였으 며, 복원 부위에 장력이 가해지는 것을 막기 위해 prolene mesh (Ethicone)를 사용하여 결손부 전체를 다시 보강하였 다. Prolene mesh는 4군데를 poliglecaprone (MONOCRYLⓇ) 2-0를 사용하여 횡경막각과 식도주위에 고정하였다(Fig. 3).
수술 후 경과: 환자 술 후 1일째부터 식사를 시작하였으 며 식사 후 특별한 이상소견 보이지 않았다. 술 후 5일째 대장조영검사를 시행하였으며, 대장조영검사상 이상소견 이나 재발소견은 보이지 않았다(Fig. 4). 현재 외래를 통해 추적관찰 중으로 재발이나 이상소견은 보이지 않고 있다.
고 찰
횡경막 탈장은 크게 3가지 종류로 분류할 수 있다. 제1형 은 활주형이고, 제2형은 식도주위열공형, 3형은 혼합형이 다.(1,2) 다른 장기가 밀려 올라간 것을 제4형으로 분류하기 도 한다.(2) 일반적으로 제1형은 역류 증상이 주증상이며, 제2형 및 3형은 밀려 올라간 위의 기계적 폐쇄증상이 주를 이룬다.(3) 제1형은 역류성 식도염의 정도에 따라 수술을 결정하며, 2형 및 3형은 증세의 심한 정도 및 합병증 동반에 따라 수술을 결정한다. 수술을 해야하는 합병증으로는 천 공, 괴사, 출혈, 기계적 폐쇄 등이 있으며, 2형 및 3형의 경우 합병증 동반의 가능성이 높으므로 증상이 없더라도 수술을 고려해야 한다.(1) 수술은 위식도역류가 있고 내과 치료에 효과가 없는 경우에 위저부를 사용해 360도를 둘러싸는 Nissen 위저추벽성형술을 해야 하지만(1) 2형의 대부분 경 우 위식도역류가 없을 시 위고정술 같은 고정방법으로 충 분하다.(7) Nissen 위저추벽성형술을 시행한 경우 약 3개월 후에는 위식도역류 및 연하곤란 등의 증상이 사라진다고 보고되고 있다.(8) 최근에는 미세침습적인 복강경을 이용한 수술법이 고전적인 개복술을 대체하고 있다.(2,4) 본 례에서 는 위가 정상위치에 있었고 위식도역류가 없어서 복강경 수술 방법을 시행하였다. 복강경을 이용한 시술의 가장 큰 단점은 장력을 견디지 못하고 찢어져서 발생하는 재발의 문제점을 보완하기 위해 탈장복원술을 시행한 이후 mesh를 사용하여 보강하는 방법이 시도되고 있다. 이는 안정적이
고, 재발률이 현저하게 감소되었다는 보고들이 나오고 있 다.(2,5,6) 물론 장기 추적관찰을 시행한 문헌의 수가 적으 며, mesh 사용으로 인한 감염 등의 부작용으로 인한 재발률 의 증가 등으로 부정적인 견해도 있으나, 통증 및 출혈이 적고 일상생활로의 복귀가 빠르며 환자의 만족도가 높다는 분명한 장점이 있다. 횡경막 탈장의 수술 결정시 mesh를 사 용한 복강경 시술을 첫 번째로 고려해 보는 것이 필요하겠 다.
결 론
저자들은 최근 증세를 보이지 않은, 횡행결장이 밀려올라 간 횡경막 탈장을 단순 X-선 흉부촬영을 통해 진단하고 복 강경을 이용하여 치료하였기에 문헌고찰과 함께 보고하는 바이다.
REFERENCES
1) Mori T, Atomi Y. Laparoscopic repair of esophageal hiatal hernia. Nippon Geka Gakkai Zasshi 2003;104:587-92.
2) Targarona EM, Balague C, Martinez C, Garriga J, Trias M.
The massive hiatal hernia: dealing with the defect. Semin Laparosc Surg 2004;11:161-9.
3) Peeters MT, Wijsman JH, van Lanschot JJ. The para- esophageal hernia: a rare hiatal hernia requiring a specific approach. Ned Tijdschr Geneeskd 2004;148:1173-7.
4) Lal DR, Pellegrini CA, Oelschlager BK. Laparoscopic repair of paraesophageal hernia. Surg Clin North Am 2005;85:
105-18.
5) Keidar A, Szold A. Laparoscopic repair of paraesophageal hernia with selective use of mesh. Surg Laparosc Endosc Percutan Tech 2003;13:149-54.
6) Champion JK, Rock D. Laparoscopic mesh cruroplasty for large paraesophageal hernias. Surg Endosc 2003;17:551-3.
7) Baek HK, Yu HS. Paraesophageal hernia with gastric erosion.
Korean J Thorac Cardiovasc Surg 1993;26:337-41.
8) Csendes A, Burdiles P, Korn O. Laparoscopic nissen fundo- plication: the “right posterior” approach. J Gastrointestinal Surg 2005;9:985-91.