Treatment of ectopic eruption of maxillary permanent fi rst molars with modifi ed halterman appliance
6
0
0
전체 글
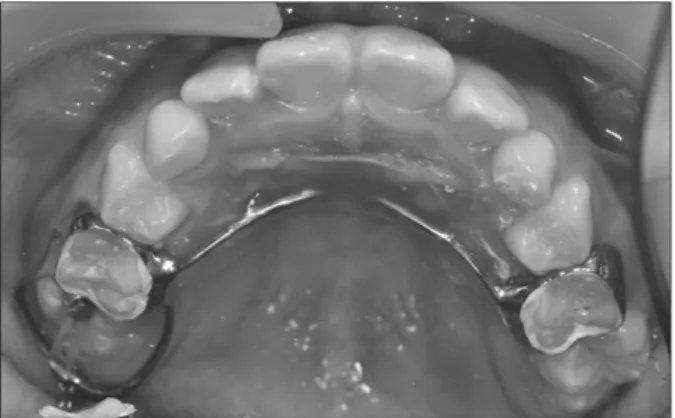
(2) Use of the modified halterman appliance in maxilla. 의하면 대구치가 이소맹출된 아이들의 형제, 자매 중 19.8%가. (Schneider & Dummett, 1985). 따라서 상악 제1대구치의 맹출. 또한 이소맹출을 보이며, 이는 이소맹출이 가족력을 가진다. 시기에는 주의깊은 관찰이 필요하며, 구순구개열을 갖는 환. 는 가설을 확인시켜주는 것이라고 하였다.. 자에서는 특히 그러하다(Da Silva Filho et al., 1996).. 제1대구치는 넓은 occlusal table을 갖고 있어 교합력의 대. 이번 증례에서는, 이소맹출한 우측 상악 제1대구치를. 부분을 담당하며, 교합의 중요한 열쇠가 되는 치아이다. 또. modified halterman appliance를 사용하여 적절한 맹출을 유도. 한 제1대구치가 제2유구치 후방으로 맹출하면서 악궁의 arch. 할 수 있었기에 보고하는 바이다.. perimeter가 확립되며, 가장 넓은 치근면적을 갖고 있어서 교. 증례보고. 정적 치아 이동에서 가장 중요한 고정원이 되는 치아이다. 따 라서 제1대구치는 전반적인 치열의 형태와 교합양상에 영향 을 미칠 수 있어 제1대구치의 이소맹출은 해소되어야 한다.. 증례1. Halterman appliance는 1982년 소개된 이후 제1대구치 이소. 만 8세 여아가 치아가 안 물려서 교정치료를 받고 싶다는 주. 맹출에 널리 사용되고 있다. 이것은 제작이 용이하고 환자의. 소로 조선대학교 치과병원 소아치과에 내원하였다. 검사 도. 협조도를 요하지 않는다는 장점이 있다(Harrison & Michal,. 중 상악 우측 제1대구치의 이소맹출이 관찰되었으며, 좌측 제. 1984). 또한 제2유구치가 심한 흡수를 보이는 경우에는 반대. 1대구치는 이미 교합면 수준까지 맹출한 상태였다. 상악 우측. 측 고정원을 Nance holding arch나 transpalatal bar를 사용하여. 제2유구치 치근이 중등도의 치근흡수를 보였으며, 동통의 병. 연결하면 고정원을 보강하여 안정성을 높일 수 있다(Kurol &. 력은 없었다(Fig. 1). 제1대구치의 제2유구치 원심치경부에의. Bjerklin, 1986).. 고착(locking)은 심하지 않았으나, 환아의 연령과 다른 제1대. 이소맹출은 크게 가역적 이소맹출과 비가역적 이소맹출로. 구치들의 맹출 정도와 비교했을 때, 비가역적 이소맹출로 진. 분류될 수 있다. 가역적 이소맹출은 특별한 치료 없이 자발적. 단되었다. Halterman appliance를 이용한 제1대구치의 원심이. 으로 치아의 맹출이 이루어지는 경우로 “jump case”라고도 하. 동을 통하여 이소맹출을 해소하기로 치료계획을 수립하였고,. 며 전체 이소맹출의 66%를 차지한다. 비가역적 이소맹출은. Halterman appliance가 아닌 반대편 상악 좌측 제2유구치를 포. 자발적으로 맹출되지 못하고, 근심에 위치한 치아의 접촉점. 함하여 고정원을 보강한 modified Halterman appliance를 계. 하방 치경부에 치아가 매복되어 인접치의 치근흡수 또는 탈. 획하였다.. 락을 야기할 수도 있어 구체적인 치료가 필요한 경우로 “hold case”라고도 한다(Young, 1957).. 양측 상악 제2유구치에 band를 적합시키고 인상을 채득 하여 양측 band가 Nance holding arch로 연결되는 modified. 일반적으로 상악 제1대구치의 이소맹출은 정기검진을 통. Halterman appliance를 제작하였다. Direct bonding system. 해 발견되는 경우가 많은데, 이는 근심경사된 상악 제1대구. (Transbond XT; 3M Unitek, Monrovia, CA, USA)을 이용하여. 치로 인해 전방의 제2유구치의 치근이 심하게 흡수되어 치수. 제1대구치 교합면에 lingual button을 부착하고 power chain을. 조직의 감염을 일으키지 않는 한 동통이 발현되지 않는 경우. 이용하여 상악 우측 제1대구치를 후방 견인하였다(Fig. 2).. 가 많기 때문이다(Pinkham et al., 2005). 정기검진 도중 이소. 그 후 2주 간격으로 환자를 내원시켜 power chain을 교환. 맹출된 치아를 발견했을 경우, 비가역적 이소맹출 여부가 확. 하였다(Fig. 3). 약 8주 후 이소맹출의 해소와 약 1 mm정도의. 실하지 않다면 약 6개월 정도는 2-3개월 간격으로 검사하면 서 자발적 맹출을 기다려 볼 수 있지만, 그 이후에도 개선되지 않을 경우 능동적인 치료를 고려해야 한다(Kennedy & Turley, 1987). Gehm과 Crespi (1997)에 의하면 만약 구강 내로 치관이 부분적으로 출은한 경우 이는 이미 비가역적인 이소맹출일 가능성이 높다고 한다. 만약 이러한 비가역적인 유형의 이소맹출이 치료되지 않은 경우에는, 치열궁(arch perimeter)의 감소와 이에 의한 인접한 소구치의 총생 또는 매복을 야기할 수 있다(Da Silva Filho et al., 1996). 또한 Venn (1995)에 의하면 치아가 고착된 부위로 타액의 유입은 치수염증이나 치주농양을 유발할 수 있다고 하였고, 이소맹출과 관련한 신경학적 통증 또한 보고되었다. 58. Fig. 1. Pre-treatment panoramic view. Right maxillary first molar mesially locked at the distal cervix of second primary molar and resorption of distal root of second primary molar were observed..
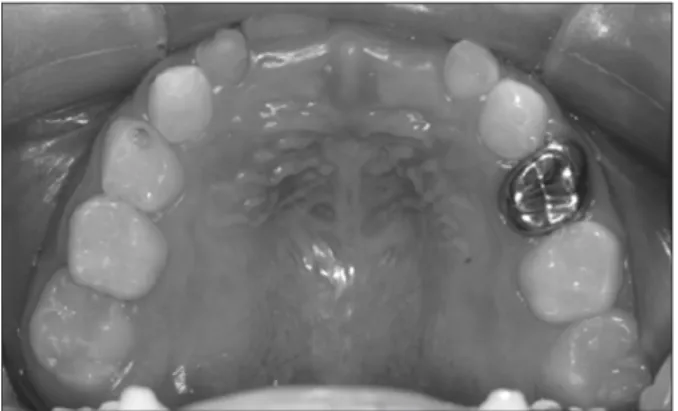
(3) Sang-Yun Jeon et al.. Fig. 5. Eight weeks after the delivery, panoramic radiograph was taken. Right maxillary first molar erupting into a normal position was observed. Fig. 2. Modified Halterman appliance was cemented. The power chain was applied.. Fig. 6. Three months after the delivery.. Fig. 3. Six weeks after delivery. Marginal ridge of the right permanent maxillary first molar was seemed to be locked.. overcorrection이 관찰되어 power chain과 lingual button을 제 거하였다(Figs. 4, 5). 장치를 장착하고 11주 후와 3개월 후 재 내원시켜 관찰하였을 때, 정상적으로 맹출하고 있는 상악 우 측 제1대구치를 관찰할 수 있었다(Figs. 6, 7).. 증례2 5세 여아로 정기검진 중 맹출한 다른 제1대구치와 달리 상 악 우측 제1대구치의 미맹출이 관찰되었다(Fig. 8). 환아의 연 령을 고려하여 5개월 간 관찰하였으나 맹출의 개선은 관찰되 지 않았고, 제2소구치가 결손된 상태이므로 제2유구치의 치 근흡수를 예방하기 위해 조기치료를 계획하였다(Fig. 9). 편측성 modified Halterman appliance를 사용하여 이소맹 출을 해소하기로 하였다(Fig. 10). 장치를 장착하고 제1대구 치 교합면에 버튼을 부착한 후 2주 간격으로 환자를 내원시켜 power chain을 교환하였다. 장치장착 6주 후 고착이 해소되고 Fig. 4. Eight weeks after delivery. The overcorrection of 1 mm was observed. The power chain and lingual button were removed.. 약 1 mm 과교정된 양상이 관찰되었다(Fig. 11). 장치장착 10주 후 power chain을 제거한 후 근심교합융선에 재발 방지를 위. 59.
(4) Use of the modified halterman appliance in maxilla. Fig. 7. Three months after the delivery. Panoramic radiograph was taken.. Fig. 10. Unilateral modified halterman appliance was cemented on right maxillary second deciduous molar.. Fig. 8. Unerupted right maxillary first molar was observed.. Fig. 11. Six weeks after the delivery of the appliance, overcorrection of 1 mm was observed.. Fig. 9. Five months after, the right maxillary first molar was still unerupted.. 한 복합레진을 첨가하였다. 장치장착 6개월 후 장치와 첨가했 던 복합레진을 제거하였다(Fig. 12). 장치제거 3주 후와 4개월 후 검진 시 정상적으로 맹출한 상악 제1대구치를 관찰할 수 있 었다(Fig. 13).. 고. 찰. Fig. 12. After 6 months, the appliance and composite resin were removed.. 증례1에서 이소맹출한 제1대구치와 맹출 중인 제2소구 치에 의한 제2유구치의 치근흡수 때문에, 제2유구치 단독. 에 충분하지 않다고 생각되었다. 따라서 양측성의 modified. 으로는 제1유구치를 원심이동시킬 수 있는 힘을 견뎌내기. Halterman appliance를 사용하였다. 또한 일반적으로 이소맹. 60.
(5) Sang-Yun Jeon et al.. 해 치아를 재위치시키는 방법을 사용할 수도 있다(Lee, 2010). 최근 mini screw와 mini plate 같은 골격고정원을 사용하 여 교정적 치아이동을 도모하는 경우가 많다. 이는 교정적 치 아이동에서 필연적으로 발생하는 고정원 상실을 최소화할 수 있으며, 또한 순, 협측 치은이나 구개부처럼 치아 외의 부 위에서 고정원을 얻어 교정력을 발생시킬 수 있기 때문에 치 아에 적합한 방향의 힘을 가하는 데 있어 유리하다. 하지만 mini implant의 식립 시 골의 해부학적 구조물과 치근을 주 Fig. 13. Four months after removal of the appliance, normal eruption of right maxillary first molar was observed.. 의해야 하며, 부가적인 수술이 필요하다. 또한 식립된 mini screw가 느슨해질 수 있어 교정력을 발휘하기에 충분치 않 을 수 있으며, 식립부위에 충분한 양의 골이 필요하다. 상악에. 출이 해소된 후 장치를 제거하는 것이 일반적이나, 장치 제거. mini implant를 식립할 때 상악 결절부위는 골량이 가장 적고. 도중 지대치로 사용되었던 상악 우측 제2유구치가 발거될 가. (Poggio et al., 2010), 이번 환자의 경우 제2대구치 치배가 위치. 능성이 높고, 하방의 제2소구치의 구강 내 출현까지 시간이 많. 하고 있기 때문에 골격고정원의 식립은 문제가 있었다.. 이 남은 것으로 생각되어, 하방 제2소구치의 맹출을 기다려 적 절한 시기에 장치를 제거하기로 계획하였다.. 이번 증례에서는 제2유구치의 치근이 심하게 흡수되어 단 독 고정원으로 사용되기 어려운 경우와 단독 고정원으로 사. 상악 제1대구치의 이소맹출의 치료방법을 선택하는데 있. 용될 수 있는 경우에서 modified Halterman appliance를 사용. 어서 상악 제1대구치의 맹출 정도, 인접한 제2유구치의 법랑. 하여 이소맹출한 상악 우측 제1대구치의 적절한 맹출을 유도. 질 ledge의 정도, 제2유구치의 동요도, 그리고 제2유구치의 동. 할 수 있었다.. 통 등을 고려해야 한다. 이소맹출의 대부분은 가역적인 경우 이므로 일차적으로 6개월 정도는 관찰이 필요하며, 그 후 맹출. 참고문헌. 방향의 개선이 관찰되지 않는다면 치료를 고려하게 된다. 비 가역적 이소맹출의 치료에는 brass wire, elastic seperator, 또 는 seperating spring 등의 간단한 장치나, Halterman appliance, Humphrey appliance 등의 장치를 이용하여 제1대구치를 원심 측으로 이동시킬 수도 있으며, 제2유구치를 발거하고 제1대 구치가 맹출한 후 상실된 공간을 회복해주는 방법을 사용할 수도 있다. 이소맹출을 치료할 경우에 인접치에 의해 매복되어 있는 양 에 따라 다양한 치료방법들을 적용할 수 있다. 인접치에 의해 매복되어 있는 양이 약 1 mm 정도인 경도의 이소맹출에서는 brass wire, separating spring, 또는 elastic separator를 이용하 여 치아 사이를 이개시키는 방법을 사용할 수 있다. 매복된 양 이 2-3 mm인 경우 장치를 이용한 본격적인 교정치료가 필요 한데, Humphrey appliance, Halterman appliance와 같은 교정 용 밴드를 이용한 장치나 교정용 브라켓과 개방형 코일 스프 링을 이용한 방법도 사용할 수 있다. 매복의 정도가 심하여 전 방치아의 동요도가 크거나 통증이나 농양이 발생한 경우, 치 근이 흡수되어 동요도와 동통이 발생한 유치를 발거하고, 가 철성 교정장치 혹은 pendulum appliance와 같은 고정성 장치 를 이용하여 상실된 공간을 재확보하고 유지하는 것이 필요 하다. 완전 매복된 치아의 경우에는, 치관의 외과적 노출과 함 께 교정력을 가하여 치아를 이동시키거나 외과적 수술을 통. Barberia-Leache E, Suarez-Clúa MC, Saavedra-Ontiveros D: Ectopic eruption of the maxillary first permanent molar: characteristics and occurrence in growing children. Angle Orthod 75:610-615, 2005. Bjerklin K, Kurol J: Prevalence of ectopic eruption of the maxillary first permanent molar. Swed Dent J 5:29-34, 1981. Bjerklin K, Kurol J, Paulin G: Ectopic eruption of the maxillary first permanent molars in children with cleft lip and/or palate. Eur J Orthod 15:535-540, 1993. Bjerklin K: Ectopic eruption of the maxillary first permanent molar. An epidemiological, familial, aetiological and longitudinal clinical study. Swed Dent J Suppl 100:1-66, 1994. Chintakanon K, Boonpinon P: Ectopic eruption of the first permanent molars: prevalence and etiologic factors. Angle Orthod 68:153-160, 1998. Da Silva Filho OG, De Albuquerque MV, Kurol J: Ectopic eruption of maxillary first permanent molars in children with cleft lip. Angle Orthod 66:373-380, 1996. Gehm S, Crespi PV: Management of ectopic eruption of permanent molars. Compend Contin Educ Dent 18:561-566, 1997. Harrison LM Jr, Michal BC: Treatment of ectopically erupting permanent molars. Dent Clin North Am 28:57-67, 1984. Kennedy DB, Turley PK: The clinical management of ectopically erupting first permanent molars. Am J Orthod Dentofacial Orthop 92:336-345, 1987. Kimmel NA, Gellin ME, Bohannan HM, Kaplan AL: Ectopic. 61.
(6) Use of the modified halterman appliance in maxilla. eruption of maxillary first permanent molars in different areas of the United States. ASDC J Dent Child 49:294-299, 1982. Kurol J, Bjerklin K: Ectopic eruption of maxillary first permanent molars: familial tendencies. ASDC J Dent Child 49:35-38, 1982. Kurol J, Bjerklin K: Ectopic eruption of maxillary first permanent molars: a review. ASDC J Dent Child 53:209-214, 1986. Lee JH, Kim JY, Park KT: Management of ectopically erupting permanent molars by the degree of impaction. J Korean Acad Pediatr Dent 37:136-142, 2010. (Korean) Pinkham JR, Casamassimo PS, McTigue DJ, Field Jr HW, Nowak AJ: Pediatric dentistry: infancy through adolescence. 4th ed, Elsevier Inc, St. Louis, pp.618, 2005.. 62. Poggio PM, Incorvati C, Velo S, Carano A: "Safe zones": a guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod 76:191-197, 2006. Pulver F: The etiology and prevalence of ectopic eruption of the maxillary first permanent molar. ASDC J Dent Child 35:138146, 1968. Schneider PE, Dummett CO Jr: Treatment of ectopic permanent molar eruption-case report. Quintessence Int 16:459-462, 1985. Venn RJ: Ectopic eruption of permanent first molars: a clinical technique. J Peded Fall 10:81-8, 1985. Young DH: Ectopic eruption of the first permanent molar. ASDC J Dent Child 24:153-162, 1957..
(7)
수치

관련 문서
