정신적 증상으로 발현된 뇌교외 수초용해증 1례
인제대학교 의과대학 소아과학교실
안보라미1・조현수2・유수정1
Case report
Submitted: 6 November, 2015 Revised: 7 January, 2016 Accepted: 22 March, 2016
Correspondence to Su Jeong You, M.D, PhD.
Department of Pediatrics, Inje University College of medicine, Sanggye Paik Hospital, 1342 Dongil-ro, Nowon-gu, Seoul 01757, Korea
Tel: + 82-2-950-1080, Fax: +82-2-951-1246 E-mail: [email protected]
J Korean Child Neurol Soc 2016;24(1):21-24 pISSN 1226-6884•eISSN 2383-8973
A Case of Extrapontine Myelinolysis Presented by Psychiatric Symptoms
Osmotic demyelination syndrome (ODS), especially extrapontine myelinolysis (EPM), is a rare neurological disorder caused by damage to the myelin sheath of the brain.
We encountered a 24-year-old man with psychiatric symptoms who was diagnosed with EPM following rapid correction of hyponatremia. Hyponatremia was induced by primary polydipsia; the serum sodium concentration of the patient was 97 mEq/L.
Previous medical history included mental retardation and epilepsy after childhood.
His seizures had been well controlled with antiepileptic drugs for about 10 years.
After admission, he was administered intravenous 3% NaCl, which increased his serum sodium concentration to 135 mEq/L over 6 days. After discharge, he com- plained of general weakness, agitation and insomnia and was readmitted. Brain magnetic resonance imaging showed symmetric T2 signal changes in the bilateral caudate head, putamen, and sparing globus. He was diagnosed with EPM and treated with diazepam and quetiapine, an atypical antipsychotic drug. Eight days later, his symptoms had improved. This study describes a 24-year-old man with psychiatric symptoms who was diagnosed with EPM caused by rapid correction of hyponatremia.
Key Words: Extrapontine myelinolysis (EPM), Hyponatremia, Psychiatric, Osmotic
demyelination syndrome (ODS)
Borami Ahn, MD
1, Hyun Soo Joh
2, Su Jeong You, MD, PhD
11
Department of Pediatrics,
2Department of Medical Science, Inje University College of Medicine, Sanggye Paik Hospital, Seoul, Korea
Copyright © 2016 by The Korean Child Neurology Society
http://www.cns.or.kr
Introduction
Osmotic demyelination syndrome (ODS) is a neurologic disease characterized by partial destruction of the myelin sheath of the brain1). Depending on the area of involvement, ODS has been classified as extrapontine myelinolysis (EPM) and central pontine myelinolysis (CPM), which differ in clinical features. The causes of ODS also vary and can include rapid correction of hyponatremia, extreme serum hyperosmolarity, chronic alcoholism, nutritional deficiency, pregnancy, organ transplantation and burns1). ODS occurs sporadically at any age, with CPM being more common than EPM. ODS can be seen on computed tomography (CT), but the current standard method for the diagnosis of ODS is brain magnetic resonance imaging (MRI). The increasing use of MRI, which is very sensitive in detecting myelinolysis, has led to increased identification of mild and even asymptomatic disease2). Although symptoms of CPM have been studied well,
22
Ahn B, et al. • A Case of EPM Presented by Psychiatric Symptoms http://www.cns.or.krthose of EPM are not as well known. In CPM, dysarthria and dysphagia (corticobulbar tract involvement) appear initially and progress from flaccid quadriparesis (corticospinal tract) to spastic quadriparesis (basis pontis). Further progression to the tegmen
tum may result in pupillary and oculomotor dysfunction35). Re
cent reports have described patients with symptoms originating beyond the central pons (EPM), including variable behavioral and psychiatric disorders. This report describes a man diagnosed with EPM without CPM, who had symptoms such as agitation, confusion, general weakness and insomnia, after rapid correction of hyponatremia.
Case Report
A 24yearold man was admitted after experiencing general weakness, insomnia and wandering at night after being dis
charged from the hospital. His previous history included mental retardation, epilepsy, and polydipsia after childhood. Because of his mental retardation, it was difficult to evaluate his symptoms.
Ten days prior to admission he experienced symptoms of vomi
ting, polydipsia, and polyuria. At admission, his mental status was confused, but he had no other neurological abnormality. Labora
tory findings showed a serum sodium concentration of 97 mEq/
L, a potassium concentration of 2.8 mEq/L and a chloride con
centration of 64 mEq/L. We was diagnosed with primary poly
dipsia and was administered intravenous 3% NaCl. His serum sodium concentration increased to 109 mEq/L after 15 hours;
after 1 to 6 days, his sodium concentrations were 109 mEq/L, 117 mEq/L, 121 mEq/L, 128 mEq/L, 133m Eq/L and 135 mEq/L, respectively. His mental status had improved and he was dis
charged. Five days later, he again became confused, was unable to avoid obstacles and had insomnia. He was admitted to the in
tensive care unit (ICU). Laboratory studies revealed no abnor
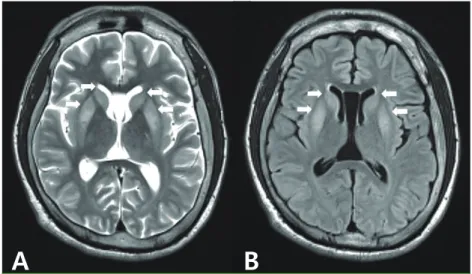
malities. An electroencephalogram (EEG) showed no epileptiform discharges and no EEG changes during abnormal behavior. MRI showed changes in symmetric T2 signals in the bilateral caudate head, putamen, and sparing globus (Fig. 1). These findings were compatible with EPM. He was treated with diazepam (15 mg/
day) and the atypical antipsychotic quetiapine (200 mg/day) to address his insomnia and irritability, respectively. Eight days later, his symptoms had stabilized and he was discharged. At a one week follow up after discharge, his symptoms well controlled with diazepam and quetiapine.
Discussion
ODS is a rare neurologic disorder characterized by damage to brain myelin. This disorder can be classified as CPM, EPM, or a combination of the two4). EPM differs from CPM, in that it invades extrapontine regions, including the cerebellum and lateral geni
culate body. EPM lesions can also occur in the external capsule, basal ganglia, thalamus, cerebral cortex, and hippocampus. In addition, although rare, these lesions occur in the mammillary bodies, columns of the fornix, amygdala, anterior commissure, optic tracts, and subthalamic nuclei. The most frequent cause of ODS is rapid correction of hyponatremia8). ODS, however, may develop in patients with other medical conditions, including chronic alcoholism, malnutrition, prolonged use of diuretics, ex
tensive burns and liver failure1). Brain MRI typically shows hyper
intense lesions in the central pons or associated extrapontine
A B
Fig. 1. MRI showed symmetric T2 and T1 signal changes in the bilateral caudate head and
putamen, sparing the globus (A, B).
J Korean Child Neurol Soc 2016;24(1):21-24
23
http://www.cns.or.krstructures such as the basal ganglia and thalamus on T2weighted and fluidattenuated inversion recovery sequences, with corres
ponding hypointensity on T1weighted sequences2). Symptoms of CPM include flaccid quadriplegia, and inability to speak or swallow, with occasional coma. In comparison, symptoms of EPM include general slowness and disorientation, with later oc
curring extrapyramidal manifestations including parkinsonism, dystonia and tremor7). Psychiatric symptoms have been reported in patients with combined CPM and EPM, but few studies have evaluated psychiatric symptoms in patients with EPM alone9,10). One patient in South Korea experienced cognitive dysfunction and neuropsychological findings of EPM without CPM11).
The patient described here presented with sleeplessness, irrit
ability at night, agitation, and confusion. MRI showed bilateral lesion of the caudate head and putamen. We considered a list of differential diagnosis including Wilson’s disease, multiple sclerosis, hypoxia, and encephalitis. However, these were excluded in this case base on the clinical examination and laboratory findings. In addition, his symptoms had improved with supportive treatment.
We concluded that EPM was the most likely diagnosis.
Psychiatric symptoms in patients with EPM may be associated with dysfunction of the frontalsubcortical circuits, including the anterior cingulate, orbitofrontal, and dorsolateral prefrontal cir
cuits12). The symptoms and brain imaging findings in the present patient were similar to those reported earlier.
No specific treatment has been shown to convincingly halt the progress of or reverse ODS. The best treatment of course is prevention. The correction of hyponatremia plays essential role in the prevention of CPM. In symptomatic acute hyponatremia, the initial rate of correction should be 12 mmol/L/h for several hours; the total daily correction should not be >8 mmol/L/d13). In this case, his sodium concentration rapidly corrected to 109 mEq/L from 97 mEq/L within 15 hours.
At present, the treatments of patients with CPM and EPM are based on their symptoms. Reports on small case series or case reports have shown a beneficial effect of various treatment such as corticosteroids, intravenous immunoglobulin, plasmapheresis and thyrotrophin releasing hormone4). Glucocorticoids have been reported to regulate BBB permeability and to prevent BBB dis
ruption induced by hyperosmolarity14). Among the sequelae of ODS, extrapyramidal Parkinsonlike symptoms can be managed by levodopalike agents and chronic seizures by antiepileptic drugs15,16).
Favorable outcomes have been reported in 5067% of patients with ODS. Factors predictive of poor outcome include hypona
tremia, associated hypokalemia, low Glasgow coma scale score, poor functional independent measures at admission and dis
charge, and poor disability rating scale scores at admission17). Although this patient had hypokalemia, he experienced a favo
rable outcome.
Findings in this patient indicate that psychiatric symptoms may be associated with EPM and that these symptoms can be suc
cessfully treated with antipsychotic drugs. ODS should be in
cluded in the differential diagnosis of patients who develop acute psychiatric symptoms after correction of hyponatremia.
요약
중심 뇌교 수초용해증과 뇌교외 수초용해증은 주로 저나트륨혈증 의 급격한 교정 후에 발생하는 질환으로 다양한 임상 양상과 특징적 인 뇌 자기공명영상 소견을 보인다. 특히 뇌교외 수초용해증에서 운 동 장애가 주 증상이며 정신적 증상에 대한 보고는 드물었다. 본 증례 의 24세 남자는 내원 10일 전 원발성 다음증으로 유발된 저나트륨혈 증의 교정 치료를 받았고, 퇴원 이후 전신 쇠약, 초조, 불면을 주소로 재 내원하였다. 입원 후 시행한 뇌 자기공명영상 결과 T2 강조 영상에 서 양측 꼬리핵머리와 조가비핵에 고신호 강도가 확인되었다. 임상 양상과 뇌 자기공명영상 소견을 토대로 뇌교외 수초용해증으로 진단 후 항정신병약을 복용하였으며 이후 증상은 호전되었다. 이에 저자들 은 정신적 증상으로 발현된 뇌교외 수초용해증 환자를 경험하였기에 보고하는 바이다.
References
1) Brown WD. Osmotic demyelination disorders: central pontine and extrapontine myelinolysis. Curr Opin Neurol 2000;13:691-7.
2) Singh TD, Fugate JE, Rabinstein AA. Central pontine and extra- pontine myelinolysis: a systematic review. Eur J Neurol 2014;21:
1443-50.
3) Graff-Radford J, Fugate JE, Kaufmann TJ, Mandrekar JN, Rabin- stein AA. Clinical and radiologic correlations of central pontine myelinolysis syndrome. Mayo Clin Proc 2011;86:1063-7.
4) Martin RJ. Central pontine and extrapontine myelinolysis: the osmotic demyelination syndromes. J Neurol Neurosurg Psy- chiatry 2004;75:22-8.
5) Ranger AM, Chaudhary N, Avery M, Fraser D. Central pontine and extrapontine myelinolysis in children: a review of 76 patients. J Child Neurol 2012;27:1027-37.
6) Huq S, Wong M, Chan H, Crimmins D. Osmotic demyelination syndromes: central and extrapontine myelinolysis. J Clin Neuro- sci 2007;14:684-8.
7) Seah AB, Chan LL, Wong MC, Tan EK. Evolving spectrum of mo- vement disorders in extrapontine and central pontine myelino- lysis. Parkinsonism Relat Disord 2002;9:117-9.
8) Kleinschmidt-DeMasters BK, Rojiani AM, Filley CM. Central and
24
Ahn B, et al. • A Case of EPM Presented by Psychiatric Symptoms http://www.cns.or.krextrapontine myelinolysis: then...and now. J Neuropathol Exp Neurol 2006;65:1-11.
9) Vermetten E, Rutten SJ, Boon PJ, Hofman PA, Leentjens AF.
Neu ropsychiatric and neuropsychological manifestations of central pontine myelinolysis. Gen Hosp Psychiatry 1999;21:296- 302.
10) Lim L, Krystal A. Psychotic disorder in a patient with central and extrapontine myelinolysis. Psychiatry Clin Neurosci 2007;61:
320-2.
11) Seok JI, Lee DK, Kang MG, Park JH. Neuropsychological findings of extrapontine myelinolysis without central pontine myelinolysis. Behav Neurol 2007;18:131-4.
12) Bridgeford D, Arciniegas DB, Batkis M, Sandberg E, Beresford TP. Methylphenidate treatment of neuropsychiatric symptoms of central and extrapontine myelinolysis. J Stud Alcohol 2000;61:
657-60.
13) Kumar S, Fowler M, Gonzalez-Toledo E, Jaffe SL. Central pontine myelinolysis, an update. Neurol Res. 2006;28:360-6.
14) Murase T, Sugimura Y, Takefuji S, Oiso Y, Murata Y. Mechanisms and therapy of osmotic demyelination. Am J Med 2006;119 (7 Suppl 1):S69-73.
15) Kwon DY, Seo WK, Park MH, Kang YS, Koh SB, Cha DR, et al. Ra- pidly deteriorating parkinsonism and dysautonomia in patient with central pontine and extrapontine myelinolysis. Clin Neurol Neurosurg 2011;113:513-4.
16) Odier C, Nguyen DK, Panisset M. Central pontine and extrapon- tine myelinolysis: from epileptic and other manifestations to cognitive prognosis. J Neurol 2010;257:1176-80.
17) Kallakatta RN, Radhakrishnan A, Fayaz RK, Unnikrishnan JP, Kesavadas C, Sarma SP. Clinical and functional outcome and factors predicting prognosis in osmotic demyelination syndrome (central pontine and/or extrapontine myelinolysis) in 25 patients. J Neurol Neurosurg Psychiatry 2011;82:326-31.