서론
치주질환의 진행을 정지시키고 이미 파괴된 치주조직을 기 능적으로 재생시키는 것은 오랫동안 치주치료의 궁극적인 목
Correspondence: Dr. Jung-Kyu Chai.
Department of Periodontology, College of Dentistry, Yonsei University, Shinchon-dong 134, Seodaemun-gu, Seoul, 120-752, Korea.
e-mail: [email protected]., Tel: 82-2-2228-8820, Fax: 82-2-392-0398
* 본 연구는 Medical Science and Engineering Research Program of Korea Science
치조골 결손부 치료시 calcium carbonate 와 calcium sulfate 혼합물의 임상적 효과
이승범
1,2, 채경준
1,2, 정의원
1,2, 김창성
1,2, 최성호
1,2, 조규성
1,2, 김종관
1,2, 채중규
1,2*연세대학교 치과대학 치주과학교실 1.
치주조직재생연구소 2.
The clinical effects of Calcium Sulfate combined with Calcium Carbonate in treating intrabony defects
Seung-Bum Lee
1,2, Gyung-Jun Chae
1,2, Ui-Won Jung
1,2, Chang-Sung Kim
1,2, Kyoo-Sung Cho
1,2, Seong-Ho Choi
1,2, Chong-Kwan Kim
1,2, Jung-Kyu Chai
1,2*1. Department of Periodontology, College of Dentistry, Yonsei University 2. Research Institute for Periodontal Regeneration
ABSTRACT
Purpose: If bone grafts and guided tissue regeneration are effective individually in treating osseous defects, then the question is, what would happen when they are combined. Bone grafts using Calcium Carbonate(Biocoral) and Guided Tissue Regeneration using Calcium Sulfate(CALMATRIX) will maximize their advantages and show the best clinical results in intrabony defects. This study was to compare the effects of a combination of CS and CC with control treated only with modified widman flap in a periodontal repair of intrabony defects.
Materials and Methods: 30 patients with chronic periodontitis were used in this study. 10 patients were treated with a combination of CS and CC as the experimental group Ⅱ and another 10 patients were treated with CC as the experimental group Ⅰ , and the remaining 10 patients, the control group were treated only with modified widman flap. Clinical parameters including probing depth, gingival recession, bone probing depth and loss of attachment were recorded 6 months later.
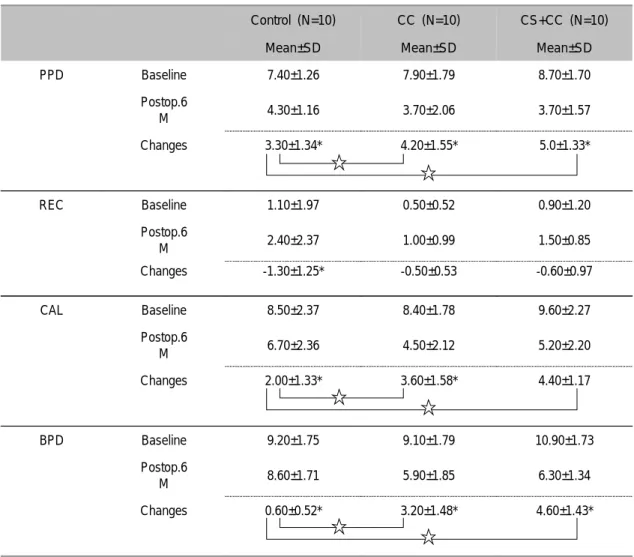
Results: The probing depth changes were 3.30±1.34 mm in the control group, 4.2±1.55 mm in the experimental group Ⅰ (CC) and 5.00±1.33 mm in the experimental group Ⅱ (CS+CC). They all showed a significant decrease 6 months after surgery( p
<0.01). There was a significant difference(p <0.05) between the control and experimental group. However there were no significant difference(p <0.05) between the experimental group Ⅰ and Ⅱ . The gingival recession changes w -1.30±1.25 mm in the control group, This is a significant difference(p <0.01). However, there was a -0.50±0.53 mm change in the experimental group Ⅰ (CC) and -0.60±0.97 mm in the experimental group Ⅱ (CS+CC). In addition, in terms of gingival recession, there was a no significance difference(p <0.05) among the groups. The clinical attachment level changes were 2.00±1.33 mm in the control group, 3.60±1.58 mm in the experimental group Ⅰ (CC) and 4.40±1.17 mm in the experimental group Ⅱ (CS+CC). They all showed a significant decrease 6 months after surgery(p <0.01). There was a significant difference(p <0.05) between the control and experimental group. However there was a no significance difference(p <0.05) between the experimental groupⅠ and Ⅱ . The bone probing depth changes were 0.60±0.52 mm in the control group, 3.20±1.48 mm in the experimental groupⅠ (CC) and 4.60±1.43 mm in the experimental group Ⅱ (CS+CC). All of them showed a significant decrease 6 months after surgery(p <0.01), there was a significance difference(p <0.05) among the groups.
Conclusion: Treatment using a combination of CS and CC have a potential to improve periodontal parameters in intrabony defects and More efficient clinical results can be expected in intrabony defects less than 2 walls grafted with CS and CC.
(J Korean Acad Periodontol 2008;38:237-246)
KEY WORDS: calcium sulfate; calcium carbonate; periodontal tissue regeneration; bone graft material.
용한 치주조직유도재생술(Guided Tissue Regeneration, 치근면 처치 등의 방법이 사용되어 왔고 최근에는 성
GTR), ,
장인자 골형성 단백질, (bone morphogenic protein, BMP), 법랑기질 유도체(Enamel Matrix Derivative, EMD)의 처치 법 등이 연구되고 있다2-6).
골이식 재료 혹은 골대체물은 골형성 세포를 갖추고 있거 나 골형성( , osteogenesis)골형성을 위한 비계 골전도( , os- 또는 골유도물질을 포함하는 이식 재료의 teoconduction),
기질역할 골유도( , osteoinduction)을 하여 치조골의 재성장 과 신부착을 촉진시킨다7).이를 이용한 골이식술에는 자가골 이식 동종골이식 이종골이식 골대체물 등이 있다 그 중 자, , , . 가골은 표준 이식재(gold standard)로서 염증반응과 면역반 응 없이 탁월한 골형성 유도능을 갖고 있는 것으로 알려져 있 다8).많은 이전 연구에서 치조골 결손부위 사용시 임상적으로 도 성공적인 결과를 나타내었다8,9).그러나, (1)부가적인 수 술부위의 필요성(2)이식시 필요한 형태 부여의 어려움(3) 골유착 유발(4)충분한 공여부 획득의 어려움(5)치근 흡수 등의 문제가 발생하기도 하였다 따라서 최근까지 이상적인. , 골대체물을 찾기 위한 많은 연구가 진행되어져 왔고 합성골, 이식재에 대한 관심도 더욱 증폭되고 있다10).
합성골 이식재 중 흡수성은 porous resorbable calcium 흡수성 carbonate, calcium sulfate, tricalcium phosphate,
가 있으며 비흡수성은 치밀성
hydroxyapatite , polymers, 등이 있다
hydroxyapatite 10-12).
이 중porous resorbable calcium carbonate(CC)는 골 결 손부의 외과적 수복을 위한 이식 골대체물로서 aragon- ite(>98%[CaCO3])결정 상태인 자연 산호를 가공하여 얻는다
13-16).약150㎛직경의 소공을 내포한 다공성 구조(>45%)이
며 생체 적합성이 좋고 골전도능이 있어서 골조직내로 이식, , 될 경우 점차 흡수되면서 신생골로 대치된다고 알려져 있다.
이미 많은 연구에서 치주 골결손부 수복을 위해 사용할 경우 성공적 결과가 나타남을 보고하였다10,17-20).
한편, GTR은Gottlow21)에 의해 처음 사용된 용어로서 차, 단막을 이용하여 치은 상피와 결합조직으로부터의 세포유입 을 차단하고 치주인대에서 유래하는 세포들이 치근면에 재증 식 할 수 있도록 공간을 유지함으로써 파괴되었던 치조골 조, 직과 치주인대를 회복시키고 소실된 백악질을 재생시키고자 하는 술식이다22). 사용되는 차단막 중 비흡수성은e-PTFE
막이 있고 흡수성은, Polylactic acid polymer, Polyglycolic acid polymer, Vicryl mesh, Oxidized cellulose, collagen 막, calcium sulfate 등이 있다23-26). 이 중 Calcium 는 최근 년간 정형외과 분야에서 인체에 안전 Sulfate(CS) 100
한 골이식재로 보고되어 왔다27).치주치료 영역에서의 사용은 약30~40년 전부터로 평균 흡수율은, 4~7주이고 생체적합성 이 우수하여 골결손부에 이식했을 때 상피의 이동을 억제함으 로써 신생골 형성에 일익을 담당한다고 보고되었다14,28-30). 그러나 Shaffer31)는CS의 직접적인 골유도기능은 없는 것으 로 보고하였고 이후 얼마간 치주영역에서의 사용은 중단되었, 다. Yamazaki32)가Bone Morphogenetic Protein(BMP)의 운송체 역할로서CS의 효능을 발표하여 다시 주목받기 시작 하였다.
그렇다면, CS는BMP의 운송체가 아닌 다른 골이식재의 골 유도 혹은 골전도 효과 역시 증진시킬 수 있는가 하는 점과 골 이식술과 치주조직유도재생술을 함께 사용한다면 보다 좋은 효과를 기대할 수 있는가 하는 점에 주목하게 된다.
과
Schallhorn McClain33,34)은 골결손부에 골이식술과 치 주조직유도재생술을 함께 사용하였고 단기 및 장기적인 관찰, 을 통해 성공적인 결과를 도출하였다 또한. Sottosanti35)는
를 와 함께 이
CS Demineralized Freeze Dried Bone(DFDB)
식시CS가 치은상피의 치근면으로의 이주 및 결합조직의 유 입을 방지함으로써 골결손부의 공간확보와 창상의 안정 에 기여하고 의 신생골 형성효과 (wound stabilization) , BMP
와DFDB의 골유도 작용을 촉진시킬 수 있다고 발표하였다. 본 교실에서도 일련의 동물실험 및 임상실험을 진행하여 성, 견 치아 주위로 형성된1,2,3면 골결손부에Medical Grade 를 적용시 우수한 치조골 형성과 백악질 형성 등의 치주조 CS
직재생을 이룰 수 있다는 것을 확인하였으며, Medical Grade 를 다른 이식 재료와 혼합이식하였을 때에도 우수한 치조 CS
골의 재생을 확인할 수 있었다19,20,36-48)
.
이에 본 연구에서는 인체의 치조골 결손부에서CS와CC를 혼합이식하였을 때CS의 공간확보 및 창상의 안정에 기여하 는 작용이CC의 신생골 대체 효과에 상승 작용을 일으켜 치주 조직재생에 효과적인 결과를 나타낼 것으로 사료되어, CS와 를 혼합이식한 경우와 단독으로 처치한 경우 및 치은박
CC CC
리소파술만 시행한 경우의 술 전과 술 후 개월의 결과를 비6 교하여 다소의 지견을 얻었기에 이를 보고하는 바이다.
재료 및 방법
연구대상 1.
연세대학교 치과대학병원 치주과에 내원한 만성 치주염으 로 진단된30명 환자에서30군데 실험군( 20 ,개 대조군10 )개 의 벽성과 벽성 혹은 환상형 골결손부 벽성1 2 (2 20 , 1개 벽성8 개 환상형 개 를 이용하였다 환자의 연령분포는, 2 ) . 30세에서 세까지 평균 세 다양하였고 남자 명 여자 67 ( 43.2±8.0 ) , 21 , 9 명이었다 연구 대상자들은 특이한 전신적 질환이 없었고 최. , 근12개월 내에 약물투여를 받지 않았다 대상 치아는 구강위. 생교육과 치석제거술 후 치주낭 탐침 깊이가 6mm이상이고, 수술시 골결손부 깊이 3mm이상 평균( 6.5±2.0mm),골결손 부 폭 2mm이상 평균( 4.6±1.9mm)의 치조골 결손부를 가진 치아를 선택하였다 제 대구치는 연구대상에서 제외하였다. 3 .
연구방법 2.
실험군 설정 1)
명 환자의 개의 골결손부에서 치은박리소파술만을 시
10 10
행한 경우를 대조군으로 정하였다. 10명 환자의10개의 골결 손부에서 치은박리소파술시 Biocoral-450(calcium carbo- 이식한 군을 실험 군 nate, Inoteb, Saint Gonnery, France) 1 으로, 10명 환자의 10개 골결손부에 CALMATRIX(calcium
와 sulfate, Lifecore Biomedical, Minesota, USA)
혼합이식한 군을 실험 군으로 나누어 실험하
Biocoral-450 2
였다.
외과적 처치 및 관찰 2)
모든 대상 환자에 대해 구강위생교육과 치석제거술을 시행 하고 치은박리수술 시행시 치주낭 깊이 치은퇴축 임상부착, , , 수준 탐침골 깊이를 측정하였다 술 후 개월에 내원하여 구강, . 3 위생관리를 받고 술 후 개월에는 수술시 측정한 임상지수들, 6 을 다시 측정하고 구강위생교육과 치석제거술을 시행하였다.
대조군에서는 Lidocaine(2% Lidocaine HCl-Epinephrine, 1.8mL, Yuhan Co., Seoul, Korea)으로 침윤마취를 시행한 후 치은열구에 절개를 시행하여 전층 치은판막을 형성한 후 골결손부 주위에 존재하는 염증조직을 제거하고 치근활택술 을 시행한 후 판막을 재위치시켜 봉합하였다.
하여 골결손부를 완전히 노출시키고 이식할 부위의 모든 육아 조직을 제거하였으며 노출된 치근은 치석제거술과 치근활택, 술을 시행한 후 Tetracycline tab. 250 mg(Chong Kun Dang 으로 치근면 처치를 시 Pharmaceutical Co., Seoul, Korea)
행하였다. 골결손부에 Biocoral 또는 CALMATRIX와 를 섞어서 채워넣고 치은 판막을 재위치시킨 후 흡수 Biocoral
성 봉합사로 완전히 봉합하였다(Fig. 1).이 때 실험 군에는1
만을 이식하고 실험 군에는 와
Biocoral , 2 CALMATRIX
를 혼합이식하였다 와 의 혼
Biocoral . CALMATRIX Biocoral 합비율은CALMATRIX 0.17g에Biocoral 0.25 로 하였다cc . 술 후 일간 항생제5 (penicillin 250 mg, t.i.d., Moxicle tab, 를 복용하고 Daewoong Pharm. Co., Seoul, Korea) ,
액 Newtrine(Kun Wha Pharmaceutical Co., Seoul, Korea) 으로 구강세척을 하루 회 이상 시행하도록 하였다 치은 판3 . 막에 위치한 봉합사(Monosyn 4.0 Glyconate Monofilament, 는 술 후 주에 제거하였 B|BRAUN, Tuttlingen,Germany) 1
다 대상환자는 술 후 개월에 내원하여 임상지수를 측정하고. 6 구강위생술식을 시행하였다
측정에 사용된 임상지수들 3)
치주낭 탐침깊이(Probing Pocket Depth)
①
각각의 대상치아에서 협측 근원심면 협측 중앙면 설측 근, , 원심면 설측 중앙면의 부위를, 6 marquis color-coded치주 낭 탐침소자를 이용하여 조직의 저항력이 느껴질 정도까지 근 단방향으로 삽입한 후 치은변연부터 치주낭 기저부까지의 깊, 이를 1.0mm단위로 측정하였다 이 중 가장 큰 값을 측정값. 으로 정하였다.
치은퇴축량(Gingival Recession)
②
백악법랑경계부에서 치은변연부까지의 길이를 1.0mm단 위로 측정하였다.
임상부착수준(Clinical Attachment Level)
③
치은퇴축량의 측정치와 측정된 치주낭 탐침깊이를 합산하 였다.
탐침골 깊이(Bone Probing Depth)
④
각각의 대상치아에서 국소 침윤마취 후 치주낭 탐침깊이의
침소자를 치조골 변연부에 닿는 느낌이 있을 때까지 힘있게 근단방향으로 삽입하여 백악법랑경계로부터의 길이를 측정하 였다.
통계처리 4)
치주낭 탐침깊이 치은퇴축 임상부착수준 탐침골 깊이는, , , 각 대상 치아의 여섯 부위에서 얻어진 기록 중 가장 깊은 부위 의 기록을 통계처리에 사용했다 대조군과 실험군들에서 각각. 의 술 전 술 후 측정값을 비교하기 위해, Wilcoxon signed 를 이용하였다 또한 대조군과 실험군들간의 측정 rank test .
지수의 비교를 위하여Kruskal-Wallis test를 이용하였다. 통계처리는SPSSWIN 12.0프로그램을 사용하여 분석하였다.
결과
육안적 소견 1.
모든 환자에서 구강 위생 상태는 양호하였고 대조군과 실, 험군들은 모두 술 후 주에 봉합사를 제거하였으며 모두 염1 , 증 소견 없이 정상적인 치유상태를 보였다.
임상지수의 변화 2.
치주낭 탐침깊이의 변화 1)
치주낭 탐침깊이는 대조군의 경우 술 전 7.40±1.26mm에 서 개월 후6 4.30±1.16mm 3.30±1.34로 mm의 감소를 실험,
군은
1(CC) 7.90±1.79mm에서3.70±2.06mm 4.20±1.55로 mm의 감소를 실험, 2(CS+CC)군은 8.70±1.70mm에서 3.70±1.57mm로5.00±1.33mm의 감소를 보였으며 세 군 모두 유의성이 있었다(P<0.01). 6개월 후 변화량에 대한 세 군간의 비교시 실험군들과 대조군간에 유의성을 보였다(p
하지만 실험 군과 실험 군간에는 유
<0.05). 1(CC) 2(CS+CC) 의한 차이가 없었다(Table 1).
치은퇴축의 변화 2)
치은퇴축량은 대조군의 경우 술 전 1.10±1.97mm에서6 개월 후 2.40±2.37mm로1.30±1.25mm의 유의한 증가를 보였다(P<0.01). 그리고 실험, 1(CC)군은 술 전0.50±0.52
에서 개월 후
mm 6 1.00±0.99mm로0.50±0.53mm의 증가 를 실험, 2(CS+CC)군도0.90±1.2mm에서 1.50±0.85 mm 로 0.60±0.97mm의 증가를 보였으나 유의성은 없었다 개. 6 월 후 변화량에 대한 세 군간 비교시도 유의한 차이는 없었다 (Table 1).
임상부착수준의 변화 3)
임상부착수준의 변화는 대조군의 경우 술 전 8.50±2.37 에서 개월 후
mm 6 6.70±2.36mm로2.00±1.33mm의 증가 를 실험, 1(CC)군은8.40±1.78mm에서4.50±2.12mm로 3.60±1.58mm의 증가를 실험, 2(CS+CC)군은9.60±2.27
에서
mm 5.20±2.20mm로4.4±1.17mm의 증가를 보였으 며 세 군 모두 유의성이 있었다, (P<0.01). 6개월 후 변화량에 대한 세 군간의 비교시 실험군들과 대조군간에 유의성을 보였 다(p<0.05).하지만 실험1(CC)군과 실험2(CS+CC)군간에 는 유의한 차이가 없었다(Table 1).
탐침골 깊이의 변화 4)
탐침골 깊이의 변화는 대조군에서 술 전 9.20±1.75mm에 서 개월 후에6 8.60±1.71mm로0.60±0.52mm의 감소를, 실험 1(CC)군은 9.10±1.79mm에서 5.90±1.85mm로 3.20±1.48mm의 감소를 실험, 2(CS+CC)은 10.90±1.73
에서
mm 6.30±1.34mm로4.60±1.43mm의 감소를 보였으 며 세 군 모두 유의성이 있었다, (P<0.01). 6개월 후 변화량 에 대한 세 군간의 비교시 대조군 실험, 1(CC) ,군 실험
군 간에 유의성을 보였다
2(CS+CC) (p <0.05)(Table 1).
Table 1. Change of Clinical Prameters (unit :mm)
Control (N=10) CC (N=10) CS+CC (N=10)
Mean±SD Mean±SD Mean±SD
PPD Baseline 7.40±1.26 7.90±1.79 8.70±1.70
Postop.6
M 4.30±1.16 3.70±2.06 3.70±1.57
Changes 3.30±1.34* 4.20±1.55* 5.0±1.33*
REC Baseline 1.10±1.97 0.50±0.52 0.90±1.20
Postop.6
M 2.40±2.37 1.00±0.99 1.50±0.85
Changes -1.30±1.25* -0.50±0.53 -0.60±0.97
CAL Baseline 8.50±2.37 8.40±1.78 9.60±2.27
Postop.6
M 6.70±2.36 4.50±2.12 5.20±2.20
Changes 2.00±1.33* 3.60±1.58* 4.40±1.17
BPD Baseline 9.20±1.75 9.10±1.79 10.90±1.73
Postop.6
M 8.60±1.71 5.90±1.85 6.30±1.34
Changes 0.60±0.52* 3.20±1.48* 4.60±1.43*
PPD: Probing Pocket Depth, REC : Gingival Recession, CAL: Clinical Attachment Level, BPD : Bone Probing Depth,
CC: Calcium Carbonate, CS : Calcium Sulfate, SD : Standard Deviation,
* significant difference from change between baseline and Postop.6 months(p<0.01, p-value of using the Wilcoxon Signed Rank)
# significant difference between groups (p <0.05)
A
B
C고찰
외과적 치주 치료는 병소 부위의 세균을 제거하고 염증상 태를 개선하지만 치조골과 치주조직 재생에 있어서는 개선없, 이 긴 접합상피의 형성으로 치유된다 따라서 보다 효과적인. 치주조직의 재생을 위해 골이식을 동반한 치은판막술과 차단 막을 이용한 치주조직유도재생술이 사용되고 있다2-6).
합성골 이식재 중 본 연구에 사용된CC는 임 등19)이 성견의 골내 치주낭에 이식하여 접합상피 차단효과와 함께 신생골 형 성을 보고하였고, Gottlow, Guillemin, Yukna10,21,49) 등도 는 점차적으로 흡수되면서 신생골로 대체되며 골형성을 유 CC
도한다고 하였다 김 등. 14)은CC를 인체의 골내 결손부에 이식 한 경우와 단순 치주판막수술을 한 경우를 비교하였는데 개, 6 월 후에 치주낭 탐침깊이 임상부착수준 탐침골 깊이를 측정, , 하여 비교한 결과에서 대조군에 비해 통계학적 유의성있는 증 가를 보고하였다.
이번 연구에서도 치조골 결손부에 CC만를 적용한 실험 군의 경우
1(CC) 4.20±1.55mm의 치주낭 탐침깊이 감소(P
<0.01), 3.60±1.58mm의 임상부착수준의 증가(P<0.01) 및 3.20±1.48mm의 탐침골 깊이의 감소(P<0.01)를 보이며 기 존의 연구와 유사한 결과를 나타내었다 하지만 조직학적 검. 사를 시행할 수 없었으므로 임상지표의 개선과 신생골 형성의 직접적인 관계는 확인할 수 없었다.
한편 지금까지 연구된 치주조직의 재생의 또다른 치료방, 법인 치주조직유도재생술의 결과들을 바탕으로 생각한다면
10,13,50),결국 골이식술과 치주조직유도재생술을 혼합한 술식
으로 한층 효과적인 치주조직 재생을 유발시킬 수 있을 것이 라는 점에 주목하게 된다. Schallhorn33)과 McClain34)은 골결
손부에 대한 두 술식의 혼합사용 후 단기 및 장기적인 관찰을 통해 성공적인 결과를 도출하였다 본 연구에서도 골형성 전. 도능이 있고 점차 흡수되는 성질의CC와 치은상피가 치근면 으로 이주하는 것을 방지함으로써 골결손부의 공간을 확보하 는CS를 혼합이식 하였다 이번 연구에 사용된. CS는CC와 혼 합되어 경화 전까지putty상태를 유지하면서 비정형 골결손 부의 형태를 따라 채워질 수 있게 술자가 조작할 수 있다 따. 라서, CS는 골결손부에서 차단막의 역할을 수행하게 된다22). 특히 골결손부의 형태가 환상형이거나 벽성 이하일 경우 이2 , 식재에 안정을 부여해 줌으로써 골형성 전도능의 증진을 기대 할 수 있게 된다. CS에 대한 이전의 연구를 살펴보면,
과
Weinmann Sicher28)는 칼슘염이 조골세포의 분화에 가장 중요한 자극원이라고 생각하였고 골화는 Ca++의 국소적인 농 도 증가에 기인한다고 하였다. Bahn51)은 토끼의 하악골 결손 부에 이식시 평균4.7주 내에 모두 흡수되며 골막과 함께 작 용할 때 골형성이 촉진된다고 하여 공간 충전물(Space Filler) 로서의 역할을 강조하였다. Frame등52)은CS Hydroxyapatite를 와 함께 치조골 재생에 사용할 때CS가 조작을 용이하게 한다 고 하였고, 1988년Yamazaki 등32)은BMP의 운송체로서, 골 유도효과의 증폭제 로서의 역할을 발표하
BMP (enhancer)
였다. CS는 다른 이식재와 혼합하였을 때도 이식재의 효과를 증폭시킬 수 있었다. Sottosanti35)는DFDB와 함께 이식시 형 태부여가 쉽고, CS가 치은상피의 치근면으로의 이주 및 결합 조직의 유입을 방지함으로써 골결손부의 공간확보와 창상의 안정(wound stabilization)에 기여하며DFDB의 골유도 작용 을 촉진시킬 수 있다고 발표하였다 또한 조직 절개선을 따라. 노출시에도 조직의 수축없이 천천히 흡수된다고 하였다 본. 교실에서도CS에 대한 일련의 실험들을 진행하여 치주조직
Figure 1. Clinical case of Biocoral graft plus CALMATRIX.
A. clinical periodontal status before surgery. B. initial radiograph. Tooth #37. C. surgical view of circumferential defect after debridement and SRP. D. Biocoral plus CALMATRIXhas been placed into the defect. E. 6 months postoperative clinical periodontal status. F. 6 months postoperative radiograph demonstrates filling of the defect.
D
E
F
재생에 대한 효과 및 다른 이식재와 혼합 후 재생 증진의 가능 성에 대하여 알아보았다 성견 치아 주위로 형성된. 1, 2, 3면 골결손부에서Medical Grade CS가 우수한 치조골 형성과 백 악질 형성 등의 치주조직 재생을 이룰 수 있다는 것을 확인한 바 있으며, Medical Grade CS를 다른 이식 재료와 혼합이식 하였을 때에도 우수한 치조골의 재생을 보였고 단독으로 이용 한 임상 실험에서도 골결손부의 치유에 효과적인 결과를 보였
다19,20,36-45,47,48).특히 최 등36)에 의하면 성견의 면 골내낭에3
와 를 혼합이식한 후 관찰한 조직학적 결과에서 신생백 CC CS
악질과 신생골의 형성이 증가하였으며 생체반응 역시 우수하, 였다고 하였다 본 연구에서도 실험. 2(CS+CC)군의 경우 5.00±1.33mm의 치주낭 탐침깊이 감소(P<0.001)와4.40±
1.17mm의 임상부착수준의 증가(P<0.01)및4.60±1.43mm의 탐침골 깊이에 감소(P<0.01)를 보였다 대. 조군과 비교시에도 치주낭 탐침깊이 감소 및 부착수준의 증가와 탐침골 깊이의 감소에서 유의성을 보였다 하지만 실험. 1(CC)군과 비교시에 는 탐침골 깊이의 감소에서만 유의성을 나타내었다 이것은. 대상 환자의 선정에 있어서 실험, 1(CC)군의 경우 벽성 골결1 손부는 없이 개의 벽성 골결손부에 시행하였고 골결손부9 2 , 깊이는 평균 6.20±2.2mm, 폭은 평균3.10±0.6mm였다. 반면 실험, 2(CS+CC)군은 개의 벽성 골결손부와 개의5 1 4 2 벽성 골결손부에 시행하였으며 골결손부 깊이도 평균 7.70±1.4mm,폭은 평균5.60±1.8mm였다 즉 골결손부의. , 형태에 따라 치조골의 재생에는 차이가 나는데, Quintero53)에 의하면 치료 개월 후 벽성 골결손부는6 1 61%, 2벽성 골결손부 는62%, 3벽성 골결손부는73%의 치조골 재생을 보였다 따라. 서 골결손부의 벽면이 많을수록 세포의 공급이 많아지고 이식, 재의 유지가 좋아져서 재생의 예후가 우수해지는데 이러한 양 상은 실험 결과에서 확인할 수 있었다.
본 연구는 술 후 개월의 평가이므로6 CS와CC의 장기적인 골재생 효과를 알아보기 위해서는 보다 오랜 기간의 연구가 필요하며 각각의 골결손부의 형태에 따라서 수복량이 어떻게, 변화하는가에 대한 연구도 필요할 것으로 사료된다 또한 임. 상 결과의 계측방법에 있어서도 정확한 골충전(bone fill)상 태를 계측할 수 있도록 방사선 사진을 이용한 디지털 계측 방 법의 추가가 필요하리라 사료된다.
이번 연구로 치주골 결손부의 수복 치료시CS와CC의 혼합 물을 이식하는 술식은 상실된 치주조직 재생에 효과적이라고 할 수 있으며 특히 벽성 이하의 골결손부에 있어서 보다 좋, 2
참고문헌
1. Zander HA, Polson AM, Heijl LC. Goals of periodontal therapy. J Periodontol 1976;47:261-6.
2. Karring T, Nyman S, Lindhe J. Healing following im- plantation of periodontitis affected roots into bone tissue. J Clin Periodontol 1980;7:96-105.
3. Aukhil I, Simpson DM, Schaberg TV. An experimental study of new attachment procedure in beagle dogs. J Periodontal Res 1983;18:643-54.
4. Nyman S. Bone regeneration using the principle of guided tissue regeneration. J Clin Periodontol 1991;18:494-8.
5. Stahl SS, Froum S. Histologic healing responses in human vertical lesions following the use of osseous allografts and barrier membranes. J Clin Periodontol 1991;18:149-52.
6. Lekovic V, Klokkevold PR, Camargo PM, et al. Evaluation of periosteal membranes and coronally positioned flaps in the treatment of Class II furcation defects: a comparative clinical study in humans. J Periodontol 1998;69:1050-5.
7. Lindhe J, Karring T, Lang NP. Clinical periodontology and implant dentistry. 3rd ed. Copenhage: Munksgaard, 1998, 1997.
8. Marx RE. Clinical application of bone biology to man- dibular and maxillary reconstruction. Clin Plast Surg 1994;21:377-92.
9. Mellonig JT, Bowers GM, Bailey RC. Comparison of bone graft materials. Part I. New bone formation with autografts and allografts determined by Strontium-85. J Periodontol 1981;52:291-6.
10. Guillemin G, Patat JL, Fournie J, Chetail M. The use of coral as a bone graft substitute. J Biomed Mater Res 1987;21:557-67.
11. Dragoo MR, Sullivan HC. A clinical and histological eval- uation of autogenous iliac bone grafts in humans. I. Wound healing 2 to 8 months. J Periodontol 1973;44:599-613.
12. Levin MP, Getter L, Cutright DE. A comparison of iliac marrow and biodegradable ceramic in periodontal defects. J Biomed Mater Res 1975;9:183-95.
13. Yukna RA, Yukna CN. A 5-year follow-up of 16 patients treated with coralline calcium carbonate (BIOCORAL) bone replacement grafts in infrabony defects. J Clin Periodontol 1998;25:1036-40.
sulphate on the healing of periodontal intrabony defects. Int Dent J 1998;48:330-7.
15. Reynolds MA, Aichelmann-Reidy ME, Branch-Mays GL, Gunsolley JC. The efficacy of bone replacement grafts in the treatment of periodontal osseous defects. A systematic review. Ann Periodontol 2003;8:227-65.
16. Wikesjo UM, Lim WH, Thomson RC, et al. Periodontal re- pair in dogs: evaluation of a bioabsorbable space-providing macroporous membrane with recombinant human bone morphogenetic protein-2. J Periodontol 2003;74:635-47.
17. Souyris F, Pellequer C, Payrot C, Servera C. Coral, a new biomedical material. Experimental and first clinical inves- tigations on Madreporaria. J Maxillofac Surg 1985;13:64-9.
18. Issahakian S, Ouhayoun JP. [Clinical and histological eval- uation of a new filling material: natural coral]. J Parodontol 1989;8:251-9.
19. Im SY, Chai JK. The effect of Pours resorbable calcium carbonatein healing intrabony defect in the dog. J Korean Acad Periodontol 1991;21:365-375.
20. Jung YS, Kim CK. calcium sulfate bonegraft material bind- er regeneration guidedtissue regeneration barrier porous re- sorbable calcium carbonate. J Korean Acad Periodontol 1996;26:605-621.
21. Gottlow J, Nyman S, Karring T, Lindhe J. New attachment formation as the result of controlled tissue regeneration. J Clin Periodontol 1984;11:494-503.
22. Pontoriero R, Nyman S, Lindhe J, et al. Guided tissue re- generation in the treatment of furcation defects in man. J Clin Periodontol 1987;14:618-20.
23. Fleisher N, de Waal H, Bloom A. Regeneration of lost at- tachment apparatus in the dog using Vicryl absorbable mesh (Polyglactin 910). Int J Periodontics Restorative Dent 1988;8:44-55.
24. Galgut PN. Oxidized cellulose mesh used as a bio- degradable barrier membrane in the technique of guided tis- sue regeneration. A case report. J Periodontol 1990;61:766-8.
25. Selvig KA, Kersten BG, Chamberlain AD, et al.
Regenerative surgery of intrabony periodontal defects using ePTFE barrier membranes: scanning electron microscopic evaluation of retrieved membranes versus clinical healing. J Periodontol 1992;63:974-8.
26. Robert P, Mauduit J, Frank RM, Vert M. Biocompatibility and resorbability of a polylactic acid membrane for perio- dontal guided tissue regeneration. Biomaterials 1993;14:353-8.
27. Orsini M, Orsini G, Benlloch D, et al. Comparison of cal- cium sulfate and autogenous bone graft to bioabsorbable membranes plus autogenous bone graft in the treatment of intrabony periodontal defects: a split-mouth study. J Periodontol 2001;72:296-302.
28. Weinmann JPaS, Sicher H. Bone and Bones ... Second edi- tion: pp. 508. Henry Kimpton: London; St. Louis printed, 1955.
29. Bell WH. Resorption Characteristics of Bone and Bone Substitutes. Oral Surg Oral Med Oral Pathol 1964;17:650-7.
30. Urist MR. Bone: formation by autoinduction. Science 1965;150:893-9.
31. Shaffer CD, App GR. The use of plaster of paris in treat- ing infrabony periodontal defects in humans. J Periodontol 1971;42:685-90.
32. Yamazaki Y, Oida S, Akimoto Y, Shioda S. Response of the mouse femoral muscle to an implant of a composite of bone morphogenetic protein and plaster of Paris. Clin Orthop Relat Res 1988:240-9.
33. Schallhorn RG, McClain PK. Combined osseous composite grafting, root conditioning, and guided tissue regeneration.
Int J Periodontics Restorative Dent 1988;8:8-31.
34. McClain PK, Schallhorn RG. Focus on furcation de- fects--guided tissue regeneration in combination with bone grafting. Periodontol 2000 2000;22:190-212.
35. Sottosanti JS. Calcium sulfate is a safe, resorbable barrier adjunct to implant surgical procedures. Dent Implantol Update 1993;4:69-73.
36. Choi MR, Cho KS, Chai JK, Kim CK. Effect of composite graft of calcium carbonate and calcium sulfate on the pe- riodontal regeneration of 3-wall intrabony defects of adult dogs. J Korean Acad Periodontol 1994;24:633-648.
37. Choi SH, Cho KS, Moon IS, et al. Calcium sulfate Membrane effects of wound repair in dehiscence defects in the dog. J Korean Acad Periodontol 1997;27:249-262.
38. Kim JS, Choi SH, Yoo YJ, et al. calcium sulfate plate- let-derived growth factor(PDGF) biocompatible vehicle pe- riodontal tissue regeneration. J Korean Acad Periodontol 1997;27:785-804.
39. Cho KS, Choi SH, Chai JK, et al. The Effects of Graft of DFDB combined with Calcium Sulfate membrane on the Periodontal Wound Healing of Horizontal Dehiscence Defects in Dogs. J Korean Acad Periodontol 1997;27:347-361.
40. Suh HY, Choi SH, Moon IS, et al. The Effects of calcium
sulfate on healing of 1 - wall intrabony defects in dogs. J Korean Acad Periodontol 1997:27:363-377.
41. Choi DH, Choi SH, Moon IS, et al. The Effect of Calcium Sulfate on the Periodontal Healing of 2 - Wall Intrabony Defects in Dogs. J Korean Acad Periodontol 1997;27:395-409.
42. Lee JH, Kim SY, Choi SH, et al. The effects of calcium sulfate on periodontal ligament cells. J Korean Acad Periodontol 1998;28:235-409.
43. Kim CK, Kim HY, Chai JK, et al. Effect of a calcium sul- fate implant with calcium sulfate barrier on periodontal healing in 3-wall intrabony defects in dogs. J Periodontol 1998;69:982-8.
44. Moon HI, Cho KS, Chai JK, Choi SH. The Effect of com- posite Graft of allogenic DFDB and Calcium Sulfate with and without Calcium Sulfate barrier in Periodontal 1 wall intrabony defects in Dogs. J Korean Acad Periodontol 1998;28:219-237.
45. Kim CK. Periodontal repair in dogs: effect of the modified calcium sulfate paste on the 1-wall intrabony defects. J Korean Acad Periodontol 1999;29:219-237.
46. Choi SH, Kim CS, Suh JJ, et al. The Effects of Enamel Matrix Derivative and Calcium Sulfate Paste on the Healing of 1 - Wall Intrabony Defects in Beagle Dogs. J Korean Acad Periodontol 2000;30:539-555.
47. Hyun SJ, Kim CS, Choi SH, et al. The Effects of Paste
Type Calcium Sulfate on the Periodontal Healing of 3-Wall Intrabony Defects in Dogs. J Korean Acad Periodontol 2002;32:1-25.
48. Kim TG, Hyun SJ, Jung UW, et al. effects of paste type calcium sulfate on the periodontal healing of 3-wall in- trabony defects in dogs. Key Engineering Materials 2006:309-311.
49. Yukna RA. Clinical evaluation of coralline calcium carbo- nate as a bone replacement graft material in human perio- dontal osseous defects. J Periodontol 1994;65:177-85.
50. Kim CK, Choi EJ, Cho KS, et al. Periodontal repair in in- trabony defects treated with a calcium carbonate implant and guided tissue regeneration. J Periodontol 1996;67:1301-6.
51. Bahn SL. Plaster: a bone substitute. Oral Surg Oral Med Oral Pathol 1966;21:672-81.
52. Frame JW, Rout PG, Browne RM. Ridge augmentation us- ing solid and porous hydroxylapatite particles with and without autogenous bone or plaster. J Oral Maxillofac Surg 1987;45:771-8.
53. Quintero G, Mellonig JT, Gambill VM, Pelleu GB, Jr. A six-month clinical evaluation of decalcified freeze-dried bone allografts in periodontal osseous defects. J Periodontol 1982;53:726-30.