58
소아외과:제 15 권 제 1 호 2009년 Vol. 15, No. 1, June 2009
Tubular Hindgut Duplication with Rectovaginal Fistula, Dysplastic Kidney and Ectopic Ureter
- case report -
울산대학교 의과대학 서울아산병원 외과학교실
남소현․김대연․김성철․김인구
Submission : 08 / 12 / 31 Acceptance : 09 / 2 / 10 Correspondence:In-Koo Kim, M.D.
Department of Surgery, University of Ulsan College of Medicine, Asan Medical Center, 388-1, Poognap-dong, Songpa-gu, Seoul 138-736, Korea
Tel : 02)3010-3484, Fax : 02)474-9027 E-mail: ikkim@amc.seoul.kr
INTRODUCTION
Alimentary tract duplication is a rare congenital malformation that can be found anywhere from mouth to anus1,2, with about one-half being in the ileum and ileocecal junction3,4. Duplications are usually single and of variable size4,5. About 90 % are cystic, with the remaining being tubular6. The duplication usually shares a common smooth muscle wall and blood supply with the proper bowel5. Rectal duplications are especially rare, and their symptoms may be confused with those of other types of anorectal pathology, resulting in the necessity for multiple surgical procedures7. Here, we describe a tubular hindgut duplication with rectovaginal fistula, dysplastic kidney and
ectopic ureter in a 16-month-old girl.
CASE REPORT
A 9-month-old girl was referred to our hospital due to stooling from vagina after an enema. She was born at term with ventricular septal defect, atrial septal defect and pulmonary stenosis, diagnosed prenatally. From birth, she had two bowel movements per week with a weekly enema. At 4 months of age, her mother observed that her rectum prolapsed at straining. We couldn’t find any abnor- mality by physical examination, colon study and vaginography except the right dysplastic kidney and ectopic ureter opening into vagina at 9 months of age (Fig. 1). At 11 months of age, she underwent corrective surgery for con- genital heart disease in our hospital.
Although she suffered from the same symptoms for 5 months, repeated colon study didn’t document the fistula. We did
Fig. 1. Vaginography showing the right ectopic kidney and ureter opening into the vagina.
Fig. 2. The colon study via the anus and fistula showing tubular duplication of the rectum.
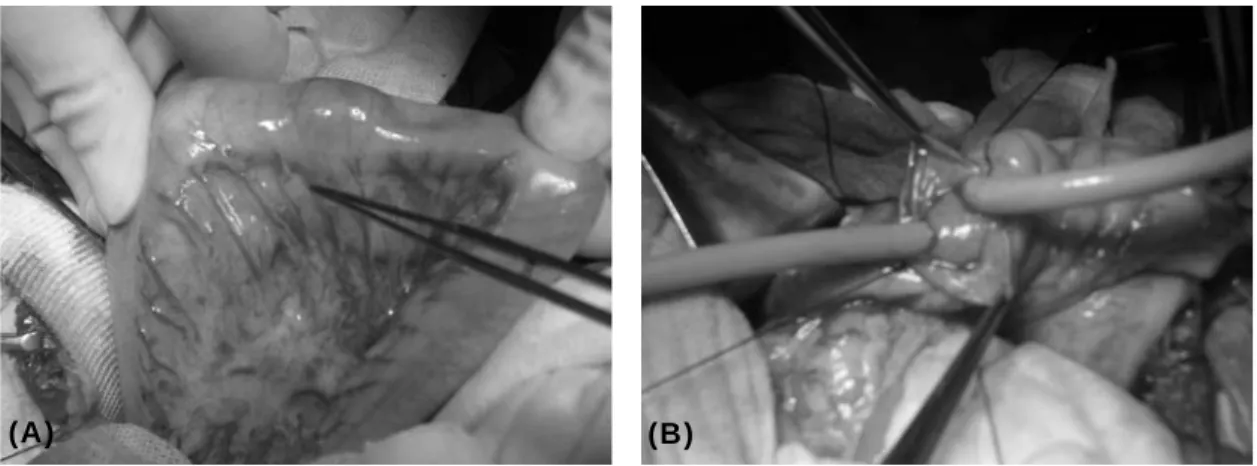
an examination under the anesthesia and identified the rectovaginal fistula at 16 months of age. A contrast study via the anus and fistula with a catheter showed tubular duplication of rectum with fistula (Fig. 2). Computed tomography and DMSA scan showed non-functioning right kidney. For impression of rectal dupli- cation we decided the exploration. An enterotomy at the sigmoid colon showed two separate intestinal lumens sharing a mesenteric vessel with a common wall (Fig. 3-a,b). The duplication extended from the distal third of the transverse colon to the distal rectum with proximal communication. In prone position, we could find out the fistula between duplicated rectum and vagina, and repaired
the fistula on the vaginal side. Through the fistula site of the duplicated rectum, we incised the septum using a GIA stapler 80 mm, allowing the duplication to communicate with the proper rectum.
After septotomy, we repaired the fistula site of the duplicated rectum and perineal body. After repositioning the patient to the supine position, we made another septotomy using the GIA stapler 80 mm from distal transverse colon to descending colon through the previous enterotomy site (Fig. 4), and we removed the right atrophic kidney and ureter for prevention of infection. The patient recovered uneventfully. To date, 3 years after surgery, she has been in good health, with one or two bowel movements a day.
60 소아외과 제 15 권 제 1 호 2009년
(a) (b)
Fig. 3. (a),(b) Two separate intestinal lumens share a mesenteric vessel with a common wall.
rectum bladder
Duplicated hindgut
GIA 80
GIA 80 Rectovaginal fistula division
sacrum
rectum bladder
Duplicated hindgut
GIA 80
GIA 80 Rectovaginal fistula division
sacrum
bladder Duplicated hindgut
GIA 80 GIA 80
GIA 80 GIA 80 Rectovaginal fistula division
Rectovaginal fistula division
sacrum
Fig. 4. Surgical procedure
DISCUSSION
Digestive tract duplication, which occurs in 1 of 4000 births8, is the term used to describe cystic or tubular structures lined with intestinal type mucosa and muscle fibers arranged in two layers in a similar pattern of adjacent viscera6,9. Although several theories have been put forward, the origin of these duplications remains obscure10,11,12.
The presentation of a rectal duplication depends on five factors7: size, fistulization
13, infection in the duplication, the presence of ectopic gastric mucosa with ulceration1 and malignant degeneration 11,14,15. As the duplicated rectum enlarges, local symptoms, such as tenderness, low back pain, suprapubic pain, constipation, dysuria, dystocia, or sciatic pain, may develop16. A complete duplication of the colon either terminates in a blind pouch or opens via rectourinary or rectovaginal fistulas17. The blind pouch can cause obstructive symptoms or rupture as the duplicated colon distends massively11,17. Bleeding from an ulceration, either within the duplication itself or in the adjacent normal intestine, has been described, occurring in approximately 20 % of these patients11,18. In addition, heterotopic gastric mucosa has been identified in 29 % of duplications5.
To prevent these complications, early and correct diagnosis and treatment are
(A) (B)
needed7. Prenatal USG has shown improved diagnostic accuracy. It shows hyperechoic mucosa surrounded by hypoechoic muscular layers and the presence of debris within the lesion.
Careful history taking and physical examination, including examination under general anesthesia, can be important in the diagnosis of duplications, such as in our patient.
Treatment can and should be instituted expeditiously before the onset of symptoms or complications19. Although definitive excision is curative7, in some cases the location and anatomical complexity of the duplication may preclude surgical resection. Excision of total colonic or rectal duplications is especially hazardous. Therapy should be directed toward relief of symptoms in accordance with the anatomic arrangement in each patient3. Definite excision is recommended if possible, but adequate internal drainage may be the treatment of choice in patients with rectal or total colonic duplications13. In addition, the surgical correction of total hindgut abnormalities will require individualized treatment because of the concomitant extensive genitourinary anom- alies. If there is no common wall distally, greater ingenuity is needed to create a connection to the patent bowel by means of a “window”, a side-to-side anas- tomosis2,3. We adopted a septotomy via the
proper rectum and the fistula site of the duplication using automatic instruments and division of the fistula. This simplified surgical correction was adequate for this patient. Although most duplications require early complete excision to avoid compli- cations and late malignancy, these risks must be balanced against the reported rarity of malignant changes and the hazards of overzealous surgery5.
Here, we have described a patient with hindgut duplication, rectovaginal fistula, ectopic ureter and dysplastic kidney.
Diagnosis and treatment was difficult and long time-saving, but the patient was relieved from constipation and rectovaginal fistula. An adequate drainage procedure and fistula division was the proper treatment for our patient. Due to possible complications such as bleeding, malignant changes and recurrent fistula, the patient should be followed-up for a long time.
REFERENCES
1. Ladd WE, Gross RE: Surgical treatment of duplications of the alimentary tract:
enterogenous cysts, enteric cysts, or ileum duplex. Surg Gynecol Obst 70:295-307, 1940
2. Bower RJ, Sieber WK, Kiesewetter WB:
Alimentary tract duplications in children.
Ann Surg 188:669-674, 1978
3. Soper RT: Tubular duplication of the colon and distal ileum: case report and discussion. Surgery 63:998-1004, 1968
62 소아외과 제 15 권 제 1 호 2009년
4. 김태우, 정풍만: 장중복증의 임상적 고 찰. 소아외과 10:9-16, 2004
5. Stringer MD, Spitz L, Abel R, Kiely E, Drake DP, Agrawal M, Stark Y, Brereton RJ: Management of alimentary tract duplication in children. Br J Surg 82:74-78, 1995
6. Payne CE, Deshon GE Jr, Kroll JD, Sumfest J: Colonic duplication: an unusual cause of enterovesical fistula.
Urology 46:726-728, 1995
7. La Quaglia MP, Feins N, Eraklis A, Hendren WH: Rectal duplications. J Pediatr Surg 25:980-984, 1990
8. Potter EL: Pathology of the fetus and infant, 2nd ed. Chicago, Yearbook Medical Publishers, 1969
9. Carvalho F, Pereira F, Enes C: Cystic duplication of the rectum-report of two clinical cases. Eur J Pediatr Surg 8:170-173, 1998
10. Iyer CP, Mahour GH: Duplications of the alimentary tract in infants and children. J Pediatr Surg 30:1267-1270, 1995
11. Orr MM, Edwards AJ: Neoplastic change in duplications of the alimentary tract. Br J Surg 62:269-274, 1975
12. Stockman JM, Jenkins AL: Duplication of
the rectum containing gastric mucosa.
JAMA 173:1223-1225, 1960
13. Kraft RO: Duplication anomalies of the rectum. Ann Surg 155:230-232, 1961 14. Ballantyne EN: sacrococcygeal tumors:
adenocarcinoma of a cystic congenital embryonal remnant. Arch Pathol 14:1-9, 1932
15. Crowly LV, Page HG: Adenocarcinoma arising in presacral enterogenous cyst.
Arch Pathol 69:64-66, 1960
16. Custer BS, Kellner A, Escue HM:
Enterogenous cysts: report of case involving the rectum. Ann Surg 124:508-518, 1946
17. Azmy AF: Complete duplication of the hindgut and lower urinary tract with diphallus. J Pediatr Surg 25:647-649, 1990
18. Kleinhaus S, Boley SJ, Winslow P:
Occult bleeding from a perforated gastric duplication in an infant. Arch Surg 116:122, 1981
19. Puligandla PS, Nguyen LT, St-Vil D, Flageole H, Bensoussan AL, Nguyen VH, Laberge JM: Gastrointestinal duplications.
J Pediatr Surg 38:740-744, 2003
직장-질 누공을 동반한 관형 뒤창자 중복
울산대학교 의과대학 서울아산병원 외과학교실 남소현․김대연․김성철․김인구
환아는 4개월부터 직장 탈출증과 심한 변비를 보였으며, 9개월에 질로부터 대변이 배출되는 증상 을 나타냈으나 검사상 우측 이상 형성 콩팥 및 이소성 요관 이외 특이 소견이 없어 경과 관찰을 시 행하였다. 16개월에 전신 마취하에 이학적 검사를 시행하여 누공을 확인하였고 이를 통한 대장 조 영술에서 직장 중복증을 진단하여 수술을 시행하였다. 수술 시야에서 직장부터 횡행 결장에 이르는 관형의 뒤창자 중복을 확인하고, 직장-질 누공을 분리하고 결장 및 직장에는 중격절개술을 시행하 였으며, 동반된 기형인 이소성 요관과 무기능 우측 신장은 절제하였다. 환아는 수술 후 3년간 잘 지 내고 있다. 직장-질 누공을 동반한 관형의 뒤창자 중복은 매우 드문 선천성 기형으로 저자들의 경 험을 문헌 고찰과 함께 보고하는 바이다.
(J Kor Assoc Pediatr Surg 15(1):58~63), 2009.
Index Words:Hindgut, Duplication, Rectovaginal fistula
본 논문의 요지는 2006년 11월 서울에서 개최된 제 58회 대한외과학회 추계학술대회에서 구연되었음.
교신저자:김인구, 138-736 서울시 송파구 풍납2동 388-1 울산대학교 의과대학 서울아산병원 외과학교실 Tel : 02)3010-3484, Fax : 02)474-9027
E-mail: ikkim@amc.seoul.kr