Birth Weight Predicts Anthropometric and Body Composition Assessment Results in Adults:
A Population-Based Cross-Sectional Study
Issa Al Salmi
1,2,*, Suad Hannawi
31
Medicine Department, The Royal Hospital, Muscat;
2Medicine Department, Oman Medical Specialty Board, Muscat, Oman;
3Medicine Department, Ministry of Health and Prevention, Dubai, UAE
Background: A poor intrauterine environment is associated with increased risks of hypertension, chronic kid- ney disease, and/or diabetes. This study evaluated relationships between birth weight and body habitus in a representative sample of the general population.
Methods: Adult participants were asked to complete a birth weight questionnaire. Associations between vari- ous current anthropometric and body composition measurements and birth weight were investigated.
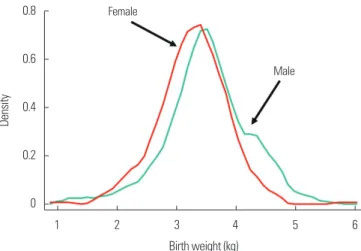
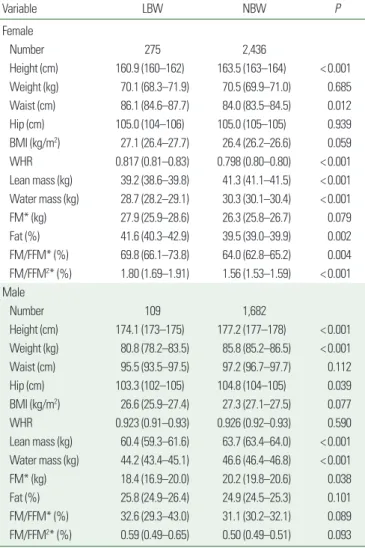
Results: Of 7,157 respondents, 4,502 reported their birth weight, which ranged from 0.4 to 7.0 kg with a mean and standard deviation of 3.37±0.7 kg; of these, 384 had low birth weights (LBWs; <2.5 kg). In females, lower birth weights were associated with lower height, weight, lean body mass (LBM), total body water (TBW), fat mass (FM), fat%, and fat-free mass (FFM) than those of higher older birth weights (quintiles); however, waist cir- cumference (WC), and hip circumference (HC) were similar across quintiles. In males, LBW was similarly associat- ed with lower height, weight, LBM, TBW, FM, fat%, and FFM, and also with lower WC and HC. The obesity mark- ers such as WC, WHR, and body mass index (BMI) were 47%, 61%, and 45% greater, respectively, in LBW females compared to normal birth weight females, while these associations showed non-significant trend in males with LBW.
Conclusion: In adult male and female respondents, LBW was associated with lower body habitus: central obe- sity and body fatness (BMI, FM, fat%, FFM, FM/FFM, and FM/FFM
2) were more pronounced in females than males, even after taking into account current physical activity and socioeconomic status. These findings indicate LBW may contribute to high blood pressure, dysglycemia and metabolic-abnormalities in adults.
Key words: Birth weight, Anthropometry, Body mass index, Body composition, Fat mass, Adiposity, Obesity
Received December 20, 2020 Reviewed April 6, 2021 Accepted April 19, 2021
* Corresponding author Issa Al Salmi
https://orcid.org/0000-0002-3443-5972 Medicine Department, The Royal Hospital, 23 July St., P.O. Box 1331, code 111, Muscat, Oman
Tel: +968-927-09000 Fax: +968-245-99966 E-mail: [email protected]
INTRODUCTION
Over the last few decades, the contribution of the intrauterine environment to the development of chronic and non-communica- ble diseases has been highlighted.
1-3Epidemiological studies have demonstrated that a poor intrauterine environment is associated with an increased risk of hypertension, chronic kidney disease, and/or diabetes. Since early 1980s, it has been hypothesized that
nutrient deprivation during distinct periods of prenatal organ de- velopment programs the offspring for cardiovascular diseaselater in life.
1-3Low birth weight (LBW), reflecting a poor intrauterine envi- ronment, is associated with diminished nephron endowment and other pathophysiological changes that may later lead to develop- ment of high blood pressure.
1,2,4LBW has been associated with the development of non-insulin- dependent diabetes and with a central pattern of fat distribution,
Copyright © 2021 Korean Society for the Study of Obesity
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
eISSN 2508-7576
2017-03-16 https://crossmark-cdn.crossref.org/widget/v2.0/logos/CROSSMARK_Color_square.svg