Introduction
The trigeminal nerve is the largest of the cranial nerves and it mainly serves in facial sensory function.
Patients with facial paresthesia or pain are often referred to an electromyography clinic for evaluation of trigeminal neuropathy. The annual incidence of trigeminal neuralgia is 4 to 13 per 100,000 people, but the incidence of posttraumatic trigeminal neuropathy is unknown.1
A trigeminal nerve can be injured by the following mechanisms; traumatic events, vasculitis, cancer, metabolic disorders, during surgical procedure, etc.
삼차신경 각 분지의 체성감각 유발전위에 대한 비교 및 고찰
이의창, 김이진, 박찬혁, 홍상은, 김명옥
인하대병원 재활의학과
Somatosensory Evoked Potentials from the Three Branches of the Trigeminal Nerve and Clinical Correlation
Eui Chang Lee, Ee Jin Kim, Chan Hyuk Park, Sang Eun Hong, Myeong Ok Kim
Department of Physical Medicine and Rehabilitation Medicine, Inha University Hospital, Incheon, Korea
Received May 11, 2016
Revised (1st) May 28, 2016, (2nd) June 7, 2016 Accepted June 8, 2016
Corresponding Author: Myeong Ok Kim
Department of Physical Medicine and Rehabilitation, Inha University Hospital, 7-206, 3-ga, Shinheung-dong, Jung-gu, Incheon 22332, Korea
Tel: 82-32-890-2480, Fax: 82-32-890-2486, E-mail: [email protected]
Objective: To obtain the reference value of latency on each branch in a trigeminal nerve SEP study and to apply the SEP values in patients with injury of a specific branch of trigeminal nerve.
Method: Thirty-two healthy volunteers and four patients with a specific branch of trigeminal nerve injury were enrolled at SEP study. A stimulation site was determined based on the most reliable waveform found according to the path of each branch of trigeminal nerve.
Results: In healthy subjects, latencies for right N1, P1 were 11.5 ± 1.6, 15.3 ± 1.9 for V1, 12.0 ± 1.4, 15.8 ± 1.7 for V2, 12.2 ± 1.9, and 16.1 ± 2.0 msec for V3 branch of trigeminal SEP. Moreover, the latency for left N1, P1 were 11.4 ± 1.9, 15.1 ± 2.0 for V1, 12.4 ± 1.7, 15.7 ± 1.8 for V2, and 12.8 ± 1.6, 16.6 ± 1.8 msec for V3 branch of trigeminal SEP. The R-L difference of latency was not significant (p > 0.05). Four patients revealed abnormal latencies in the site of their lesion.
Conclusion: This was the study charting reference values of each branch of the trigeminal SEP and applying it to the patients with trigeminal nerve injury. The injury to a specific branch of trigeminal nerve can be assessed by a SEP study using each branch of the trigeminal nerve.
Key Words: trigeminal nerve, trigeminal nerve injuries, evoked potentials, somatosensory
Copyright © by Korean Association of EMG Electrodiagnostic Medicine
This is an Open Ac cess article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ISSN 1229-6066 http://dx.doi.org/10.18214/jkaem.2016.18.1.11 J Korean Assoc EMG Electrodiagn Med 18(1):11-17, 2016
J Korean Assoc
Electrodiagn MedEMG
Recently, facial trauma by assaults, falls, motor vehicle
accidents, and sports injuries have contributed to the big proportion of the causes of the lesion.2-4 Generally, the diagnosis of posttraumatic trigeminal neuropathy tends to rely on the clinical manifestations in clinics.
The trigeminal nerve has three major branches: the ophthalmic (V1), the maxillary (V2), and the mandi- bular (V3) divisions.5 There are a few possible options to clarify lesions of the trigeminal nerve; the blink reflex, which examines only the supraorbital (V1) branch, a M-wave study on master and digastric muscles, and/or a somatosensory evoked potential (SEP) study, which is only confined to measure the mental branch (V3) of the nerve.4
Technically, trigeminal nerve conduction study is considered difficult to elicit reliable data. Most of sensory fibers of the nerve lie deep in the skull,6 so stimulation is supposed to cause myogenic artifacts.7,8
In addition, the mandibular nerve is the only division that contains axons of the motor division of the trigeminal nerve.6 Thus, both trigeminal sensory and motor conduction study is not appropriate to examine damage of a specific branch of the trigeminal nerve.
Even though there were a few previous studies on trigeminal SEP for the evaluation of V1 and V2 branches, the SEP had not been compared with other branches of the trigeminal nerve within a same subject.
When it comes to the injury of the ophthalmic or maxillary branch, the current method of a SEP study for the trigeminal nerve, which stimulates the mental nerve of the V3 branch, is considered inappropriate to evaluate a true site of injury. As mentioned above, the development of a non-invasive, objective technique for measuring an each division of the nerve is necessary since the incidence for injury of specific branch of trigeminal nerve is increasing.2
The purpose of this study is to obtain the reference value of latency on each branch in a trigeminal SEP (TSEP) study, making a standardized protocol.
Additionally, we demonstrate the differences of SEP values between a control group and the patients with injury of a specific branch of the trigeminal nerve.
Materials and Methods
This study was conducted in accordance with the principles of the International Declaration of Helsinki.
Ethical approval was granted by the institutional review board.
1) Subjects
During a period of 1 year from October 2014 through May 2016, thirty-two healthy volunteers and four subjects who reported facial hypoesthesia or paresthesia on a specific region of a face were enrolled in the study. Four subjects were suspected to have trigeminal nerve injury. The diagnosis of trigeminal neuropathy was based on clinical manifestations, consideration of the patient’s history (no evidence of metabolic or viral disease), and the results of a neurological examination. The mechanisms of each injury were all traumatic: 1) orbital wall and mandibular fracture, 2) zygomatic fracture, 3) temporal bone fracture, and 4) orbitofrontal bone fracture.
Abnormalities in the central nervous system, and any history of metabolic or connective tissue disease were not observed in any subject. Every procedure in detail was explained to all subjects before the examination.
2) Methods
An electromyography recording system, DantecTM KEYPOINT® (Alpine Biomed Aps, Skovlunde, Denmark) was used for analysis of the potentials. Rectangular pulses of 0.2 ms and 4.5~7.0 mA were applied at a rate of 3.2 Hz for stimulation. The stimulus intensity was twice that of sensory threshold. Any visible contraction of muscles was avoided by decreasing the intensity. The polarity was altered every 200 stimuli to reduce any artifact that was caused by the current. Six hundred responses were averaged for TSEP. The recording electrode was placed contralaterally to the stimulation site at the C5’ and C6’
electrode position overlying the primary face region of the somatosensory cortex according to the international 10~20 system.4,6,9 The reference electrode was positioned at
Fz. In addition, the ground electrode was positioned at the inion. Traces were replicated at least twice and superimposed to gather reproducible responses.
Measurements were made bilaterally in every subject for comparison purposes.
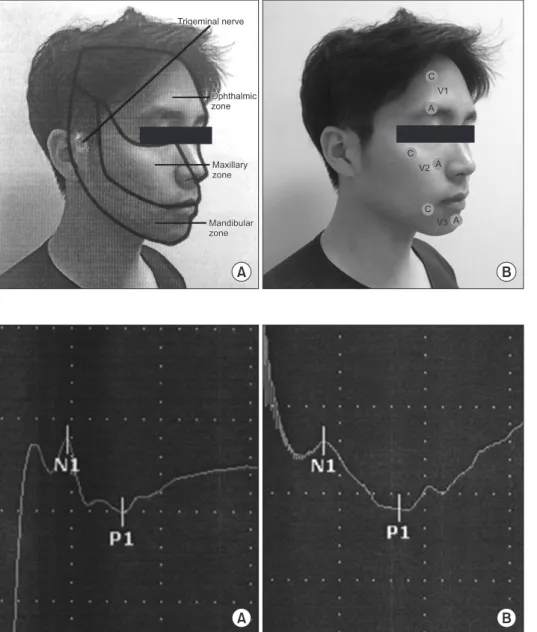
The stimulation site was determined based on the most reliable waveform which was found according to the path of each branch of the trigeminal nerve.5 The cathode was put over the supraorbital notch 4 cm above, the anode was located over the supraorbital notch 1 cm above for the ophthalmic branch (V1).
The cathode was put below the infraorbital margin along the zygomatic bone, and the anode being just
lateral to the ala of the nose for the maxillary branch (V2). Moreover, the cathode was put 1cm lateral & 0.5 cm below the commissure of the lip, with the anode being over the mentolabial sulcus 0.5 cm above for the mental branch (V3) (Fig. 1).
To eliminate the influence of electromagnetic waves on the TSEP record from room illumination, all electrical appliances were turned off.
The first negative peak can be referred to as N1, and the first positive peak as P1 (Fig. 2). The TSEP were assessed by the latency of P1 and N1 and peak-to-peak amplitudes because these produce an accurate figure and have a tendency of higher reproducibility among
Trigeminal nerve Trigeminal nerve
Ophthalmic zone Ophthalmic zone
Maxillary zone Maxillary zone
Mandibular zone Mandibular zone
V1
V2
V3 C
A
C
C A
A
A B
Fig. 1. (A) Distribution of the trigeminal nerve: the ophthalmic branch (V1), the maxillary branch (V2), and the mandibular branch (V3), (B) The stimulation points of each V1, V2, V3 branch of trigeminal nerve SEP.
B A
Fig. 2. Trigeminal somatosensory evoked potential following stimulation of (A) V1 branch and (B) V2 branch, respectively. Sweep speed 5 ms/D, Sensitivity 20 mV/D.
healthy volunteers.
3) Statistical analysis
Korean version of SPSS 21.0 for Windows (IBM SPSS, Armonk, NY, USA) was used as a means of statistical analysis. We analyzed the statistical significance of the difference between the trigeminal SEP values of latency and amplitude on right and left side with an independent t-test. Statistical significance was defined when p < 0.05.
Results
The TSEP was consistently recorded following stimulation of each branch of the trigeminal nerve from all subjects investigated. The TSEP was found to comprise two components and to show a significant contralateral dominance.
Thirty-two healthy subjects (16 women) were enrolled for normal data collection. The mean age of the subjects was 40 ± 11 years (age ranged from 26 to 58 years) showing normal distribution. The peaks N1 and P1 could be determined in all healthy subjects.
As shown in Table 1, normal values have been
Table 1. Reference Values Used for the Analysis of TSEP* Latencies and Amplitudes
V1 branch V2 branch V3 branch
N1* P1* N1-P1* N1 P1 N1-P1 N1 P1 N1-P1
Rt. 11.5 ± 1.6
(9.2~16.2)
15.3 ± 1.9 (11.1~19.5)
1.5 ± 1.1 (0.2~2.9)
12.0 ± 1.4 (9.2~13.9)
15.8 ± 1.7 (12.9~19.6)
2.2 ± 1.9 (0.4~5.8)
12.2 ± 1.9 (9.1~17.6)
16.1 ± 2.0 (12.9~20.7)
2.5 ± 1.7 (0.5~6.3)
Lt. 11.4 ± 1.9
(9.1~15.5)
15.1 ± 2.0 (12.8~19.4)
1.9 ± 1.4 (0.2~6.1)
12.4 ± 1.7 (9.9~14.3)
15.7 ± 1.8 (12.9~18.7)
2.0 ± 1.6 (0.4~4.8)
12.8 ± 1.6 (10.1~17.3)
16.6 ± 1.8 (13.9~20.5)
2.4 ± 1.8 (0.4~5.3) Both* 11.4 ± 1.6 15.2 ± 1.7 1.7 ± 1.4 12.2 ± 1.6 15.7 ± 1.6 2.1 ± 1.7 12.5 ± 1.7 16.4 ± 1.7 2.5 ± 1.9
*R-L Diff. 0.865 0.668 0.159 0.274 0.739 0.668 0.163 0.300 0.800
Unit: latency (msec), amplitude (mvolt), N1*, P1*: latency (range), N1-P1*: amplitude (range), TSEP*: Trigeminal somatosensory evoked potentials, Both*:
summation of right and left side, *R-L Diff.: p-value of right - left side difference
Table 2. Reference Values Used for the Analysis of TSEP* Latencies According to the Age
Age group (*) V1 branch V2 branch V3 branch
N1 P1 N1 P1 N1 P1
20~29 (N = 8) 11.4 ± 1.1 15.0 ± 0.8 12.4 ± 1.6 15.5 ± 1.3 12.4 ± 1.5 15.6 ± 1.1
30~39 (N = 8) 11.1 ± 1.0 14.7 ± 0.5 11.8 ± 1.4 15.5 ± 1.1 11.9 ± 1.3 16.1 ± 0.9
40~49 (N = 8) 12.6 ± 2.0 16.4 ± 1.9 12.4 ± 1.5 15.8 ± 2.1 12.5 ± 1.6 16.0 ± 1.7
50~59 (N = 8) 10.7 ± 1.9 14.6 ± 2.7 12.4 ± 1.6 16.2 ± 2.0 13.2 ± 2.1 17.7 ± 2.5
Unit: latency (msec), TSEP*: Trigeminal somatosensory evoked potentials
*Number of subjects
Table 3. TSEP* Values for Four Cases Cases
Rt. Lt.
V1 branch V2 branch V3 branch V1 branch V2 branch V3 branch
N1 P1 N1 P1 N1 P1 N1 P1 N1 P1 N1 P1
1* 9.4 10.5 9.4 10.5 NE* 8.6 11.0 12.0 14.3 NE*
2* 16.1 19.5 12.7 16.5 12.7 16.5 NE* 18.3* 21.7* 14.4 16.3
3* 13.8 17.4 16.4* 21.9* 9.5 13.3 14.2 18.7 12.2 13.7 9.4 13.8
4* NE* NE* 12.6 14.8 NE* 12.5 14.8 10.1 12.8
Unit: latency (msec), TSEP*: Trigeminal somatosensory evoked potentials, Case*: Mechanism of injury/Date of examination (Post traumatic days), 1*:
Bilateral mandibular fracture by trauma/82d, 2*: Left zygomatic fracture by trauma/64d, 3*: Right temporal bone fracture by trauma/126d, 4*: Both orbitofrontal fracture by trauma/45d, NE*: not evoked
established. No significant difference was found following stimulation of each branch between the right and left side. Differences in latency of all branches of the trigeminal nerve according to the age of subjects were not significant (p > 0.05) (Table 2). The variability of a peak-to-peak amplitude (N1-P1) for each subject was widely present, but the R-L difference of amplitude were not significant (p > 0.05) (Table 1).
As shown in Table 3, four patients had delayed or no TSEPs on a specific branch according to the sites of facial hypoesthesia and the location of lesion, compared to the normal values.
Delayed latency was determined when its value exceeded above mean + 2.5 SD.
Discussion
The neural impairment of the trigeminal nerve is thought to be influenced by multiple causal factors, including facial bone fracture by trauma, demyelinating lesions, tumor compressing along the trigeminal nerve pathway, or systemic disease such as connective tissue disease. In addition, recently, traumatic accidents along with surgical operations, suggest the incidence of postoperative trigeminal sensory nerve hypoesthesia remains relatively high.2,3
Due to the above reasons, the percentage of patients with suspected trigeminal neuropathy and those referred to the electromyography lab is increasing.2
Clinicians must be aware of the relevant anatomy, along with accurate sensory and motor testing to localize lesions more accurately.
TSEP has proven to be an objective, noninvasive measurement of trigeminal nerve injury.6 Since 1970, a number of studies have been performed, yet the results of the studies varied considerably in many aspects.
In terms of stimulation sites, TSEPs were obtained stimulating supraorbital (of the V1 branch), infraorbital (of the V2 branch), and mental nerves (of the V3 branch), respectively in various studies.10 Mental branches were most often examined among the three
branches of the trigeminal nerve.10-12
In contrast, the infraorbital branch was less frequently operated on.13,14 The mental nerve was less susceptible to myogenic artifacts than other branches of the trigeminal nerve during TSEP study.6 However, considerable changes could occur according to the site of stimulation and recording electrode.
As mentioned above, there has been a growing need to investigate each branch of the trigeminal nerve in order to find out specific lesions of the trigeminal nerve following trauma or postoperative complications.2 When it comes to the injury of the V1 or V2 branch, the existing method of SEP study for the trigeminal nerve, which stimulates the mental branch, is considered to be inappropriate to evaluate the true site of injury.
There have been many attempts to figure out reference values of the trigeminal nerve.
Stöhr M et al.8 stated the importance of stimulating mental nerve (of V3 branch) as a measurement of TSEP.
The corner of the lips (of V3 branch) was preferred in that stimulus artifact and was far less when comparing to other branches. It is because recording is efficient due to its great receptor density and wide cortical representation. This theory had been held for many researchers since then.2-4,11,15,16 Park et al.4 presented the normal values of TSEP in 24 healthy Koreans.
Progrel MA et al.16 Drechsler F et al.11 and many other researchers conducted a research on finding the normal values of TSEPs. Yet, the results showed considerable variations among the studies due to following reasons. First, even with superficial cutaneous stimulation, stimulus artifacts can be caused directly by the compound muscle action potential following stimulation of facial muscles which are inevitable in many trials.6-8,14,17 Second, reflex activation can also cause myogenic potentials which are inevitably supposed to contaminate cortical signals.10,14,17 Third, it is difficult to acquire a constant waveform of the TSEP study due to a broad homunculus area for facial proprioception.18 Finally, anatomic variations exist among individuals.8,18
In a number of previous studies, the corner of the
mouth was considered a proper site to be stimulated.
However, since the V2 and V3 branch overlap in the area, it is in fact not an appropriate site for stimulation.
In our study, the first negative peak can be referred to as N1, and the first positive peak as P1. These two peaks were distinct in most cases and were found to be very reproducible. Varying the stimulus strength significantly affected the amplitudes but not the peak latencies. In agreement with the previous literature,4,8 the variability of the peak-to-peak amplitude for each subject was widely present. Therefore, it is found that amplitudes are not of great diagnostic importance.
Whereas, Latencies are reasonably constant within all groups. The waveform was maintained irrespective of repetition of tests. Thus, the results of this study confirmed the intra-rater reliability.
Four patients with trigeminal nerve injury revealed absent evoked potential or distinct prolongation of latency in a specific branch according to the sites of facial hypoesthesia and the location of lesion. Further, even subclinical impairment of sensory function could be detected and quantified.
The results showed that clear and reliable TSEPs can be conveniently generated with stimulation at proper sites by an experienced examiner.
As mentioned above, a number of studies examined and failed to produce uniform findings. Therefore, TSEP is difficult to analyze and may be subject to debate by different observers.
Although multiple controversies still exist regarding appropriate location of stimulating a specific branch of trigeminal nerve, this study makes important findings in an attempt to standardize the reference values for the TSEP in all three branch of the trigeminal nerve.
Conclusion
We reported on the usefulness of trigeminal somatosensory evoked potential in finding lesions of the trigeminal nerve and its branches and to estimate neurologic condition. Even
more importantly, we documented reference values of each branch of TSEP and applied it to the patients with trigeminal nerve injury. In four patients with trigeminal nerve injury, the damaged branch of TSEP was not evoked at all or showed delayed latency.
Therefore, the clinical application of TSEPs has helped in treatment planning for patients with lesions of branches of the trigeminal nerve.
References
1. Katusic S, Williams DB, Beard CM, Bergstralh EJ, Kurland LT:
Epidemiology and clinical features of idiopathic trigeminal neuralgia and glossopharyngeal neuralgia: similarities and differences, Rochester, Minnesota, 1945-1984. Neuroe- pidemiology 1991: 10: 276-81
2. Tay AB, Lai JB, Lye KW, Wong WY, Nadkarni NV, Li W, Bautista D: Inferior Alveolar Nerve Injury in Trauma-Induced Mandible Fractures. J Oral Maxillofac Surg 2015: 73: 1328- 40
3. Nakagawa K, Ueki K, Takatsuka S, Takazakura D, Yamamoto E: Somatosensory-evoked potential to evaluate the trigeminal nerve after sagittal split osteotomy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001: 91: 146-52
4. Park HS, Lee KM: A Study of Trigeminal Somatosensory Evoked Potentials in 24 Healthy Koreans. Ann Rehabil Med 1988: 12: 192-6
5. Liu GT: The Trigeminal Nerve and its Central Connections.
Walsh and Hoyt's Clinical Neuro-Ophthalmology 2005: 25:
1233-51
6. Bennett MH, Jannetta PJ: Trigeminal evoked potentials in human. Electroenceph Clin Neurophysiol 1980: 48: 517-526 7. Cruccu G, Inghilleri M, Manfredi M, Meglio M: Intracranial
stimulation of the trigeminal nerve in man. III. Sensory potentials. J Neurol Neurosurg Psychiatry 1987: 50: 1323-30 8. Stöhr M, Petruch F: Somatosensory Evoked Potentials
Following Stimulation of the Trigeminal Nerve in Man. J Neurol 1979: 220: 95-98
9. Chatrian GE, Lettich E, Nelson PL: Modified nomenclature for the “10%" electrode system. J Clin Neurphysiol 1988: 5:
183-6
10. Singh N, Sachdev KK, Brisman R: Trigeminal nerve stimulation: short latency somatosensory evoked potentials.
Neurology 1982: 32: 97-101
11. Drechsler F, Wickboldt G, Neuhauser B: Somatosensory
trigeminal evoked potentials in normal subjects and in patient with trigeminal neuralgia before and after thermocoagulation of the Ganglion Gasseri. Electroenceph Clin Neurophysiol 1977: 43: 496
12. Findler G, Feinsod M: Sensory evoked response to electrical stimulation of the trigeminal nerve. J Neurosrug 1982: 56:
545-9
13. Park HR, Lee YS, Jang KE, Lee SJ: Electrodiagnostic Study for the Trigeminal Nerve. Ann Rehabil Med 1992: 16: 431-7 14. Leandri M, Parodi CI, Zattoni J, Favale E: Subcortical and
cortical responses following infraorbital nerve stimulation in man. Electroenceph Clin Neurophysiol 1987: 66: 253-6
15. Seki Y: Somatosensory evoked potentials in response to trigeminal nerve activation by electrically stimulating the lip in humans. Osaka City Med J 1987: 33: 1-17
16. Progrel MA, Mouhabaty D, Dodson T, Rampil I, Grecco M:
Trigeminal somatosensory evoked potentials: a normal value study. J Dent 1992: 20: 298-301
17. Leandri M, Parodi CI, Favale E: Contamination of trigeminal evoked potentials by muscular artifacts. Ann Neurol 1989:
25: 527-8
18. Fagade OO, Wastell DG: Trigeminal somatosensory evoked potentials: technical parameters, reliability and potential in clinical dentistry. J Dent 1990: 18: 137-41