Original Article
pISSN 2233-9019 · eISSN 2233-9116
Korean J Fam Pract. 2015;5(3, suppl. 2):1017-1023
KJFP
Korean Journal of Family PracticeOriginal Article
pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3, suppl. 2):PB-1
KJFP
Korean Journal of Family Practice서 론
세계보건기구( WHO )에서는 비만을 질병으로 분류하고 있으며 세 계적으로 소아청소년 비만의 유병률이 계속 증가함에 따라 미국, 영 국, 일본 등에서는 소아 청소년 비만 인구의 감소, 비만 합병증의 예 방을 목표로 비만관리 가이드라인을 제시하고 있다.
소아비만은 성인비만으로 이어지며 여러 신체적, 정신적 합병증 을 동반하고 고혈압, 고지혈증, 당뇨병 등의 만성 질환이 일찍 나타 나며 더 심하게 나타난다고 알려져 있다.
1)따라서 소아 청소년의 과 체중과 비만을 예방하고 비만을 조기에 진단하여 합병증을 평가하고
관리하는 것이 중요하다.
우리나라 소아비만 유병률은 2007 년 한국 소아청소년 성장도표
2)
에 의하면 9 . 7 %였고, 1997 년과 비교하여 최근 10 년간 1 . 7 배 증가 하였으며,
3)비만할수록 대사증후군의 유병률이 높아진다고 보고되 었다.
4)소아청소년의 비만은 동일 연령 및 성별의 체질량지수( body mass index , BMI )를 기준으로 비만과 관련된 질환과 고혈압, 지질 이상의 비율이 의미 있게 높기 때문에,
5)현재 95 백분위수 이상을 비 만으로, 85 백분위수 이상을 과체중으로 가장 많이 사용되고 있다.
하지만 소아는 성장발달단계에 따라 체질량지수가 신장의 변화에 영 향을 받을 뿐만 아니라 근육과 체지방량의 분포가 성성숙도와 성별
한국 청소년에서 DEXA로 측정한 비만과
복부비만 지방률의 절단점: 2008~2011년 국민건강영양조사
백래인, 이정운
*, 이동률, 이주현, 김동후, 김성종, 고경진
원광대학교 산본병원 가정의학과.
Cut-off value of percent body fat of obesity and abdominal obesity measured by Dual Energy X-ray Absorptiometry in korean adolescents: Korean National Health and Nutrition Examination Survey (KNHANES) 2008~2011
???
???
Background: Childhood obesity leads to a higher prevalence of adulthood obesity which increases the risk of metabolic syndrome. Recently, the prevalence of obesity and metabolic syndrome is rapidly increasing among children and adolescents in South Korea. The aim of this study was to estimate the accurate cutoff value for percent body fat and trunk fat measured by dual energy X-ray absorptiometry (DEXA) in adolescents.
Methods: Among 3,895 participants, aged 10~18 years, 2648 participants were selected from the Korea National Health and Nutrition Examination Survey from 2008 to 2011 and evaluated by DEXA . The cutoff value for body fat percentage was set to maximize the sum of sensitivity and specificity for detecting obesity using the Receiver Operating Characteristics (ROC) curve. The relationship between percent body fat and trunk fat with metabolic risk factors was assessed after controlling for sex and age.
Results: The cutoff value for the percent body fat used to define obesity was 32.1% in boys aged 10~12 years, 28.7% in boys aged 13~15 years, 22.8% in boys aged 16~18 years, 37.0% in girls aged 10~12 years, 35.8% in girls aged 13~15 years, and 36.2% in girls aged 16~18 years. The cutoff value of percentage trunk fat for abdominal obesity was 31.5% in boys aged 10~12 years, 24.2% in boys aged 13~15 years, 23.1% in boys aged 16~18 years, 35.4% in girls aged 10~12 years, 34.8% in girls aged 13~15 years, and 33.3% in girls aged 16~18 years.
Conclusion: The cutoff values of percent body fat and trunk fat in Korean adolescents were lower than those suggested in previous studies . Keywords: childhood obesity, percentage body fat, dual-energy X-ray absorptiometry, cutoff value
Received February 28, 2015 Revised September30, 2015 Accepted October 1, 2015 Corresponding Author Young Eun Choi
Tel: +82-?-????-????, Fax: +82-?-????-????
E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
?????
Korean Journal of Family Practice
KJFP
에 따라 다르기 때문에
6)대사증후군 등의 유병률이 높아지는 체지 방률의 적절한 진단과 그에 따른 중재가 중요하다. 소아에서도 성 인에서처럼 지방의 분포와 심혈관계 위험인자들과의 관련성이 있 으므로
7)소아의 지방분포를 정확히 평가하는 위해 여러 방법들이 소아에서도 사용되고 있다.
현재 임상에서 소아청소년의 과체중과 비만을 진단하기 위 해 지방의 분포를 평가하는데 사용할 수 있는 방법은 허리둘레 측정, 컴퓨터 단층촬영( computed tomography , CT ), 자기공명 영상( magnetic resonance image , MRI ), 생체전기저항측정법 ( bioelectrical impedance analysis , BIA ), 이중에너지 방사선 흡수계 측법( dual - energy X - ray absorptiometry , DEXA ) 등이 있다.
8)복부내장지방량을 정확히 측정하기 위해 현재 사용하는 전산화 단층촬영법( computed tomography , CT )은 내장지방과 피하지방을 분리하여 측정할 수 있는 장점이 있으나, 방사선 노출의 위험이 높 고 비용이 많이 든다는 단점이 있다.
9, 10)이에 비하여 이중에너지 방 사선 흡수 계측법 ( dual - energy X - ray absorptiometry , DEXA )은 뼈광물질량을 측정하는 방법이지만, 이를 이용하면 전신의 뼈광물 질, 지방체중, 제지방 체중뿐 아니라, 상지, 하지 및 몸통의 국소지 방량을 각각 구할 수 있고 피하지방과 내장지방을 직접적으로 구별 하지는 않지만, 몸통 부위의 지방량을 측정하여 내장 지방량을 추 정할 수 있으며 전산화단층촬영법에 비해 방사선 조사량이 적다.
11,12)
그리고 체성분 측정의 높은 재현성과 정확성이 입증되어 최근 널 리 사용되고 있다.
13, 14)일부 연구에서 DEXA 를 이용하여 소아청소년에서 남녀의 차이 를 관찰한 연구가 있었고,
15)BIA 를 이용하여 비만의 체질량률의 절 단점을 구한 연구는 있었으나,
16, 17)DEXA 를 이용한 소아청소년 비 만과 복부비만의 절단점에 관한 연구는 없었다. 그리고 미발행된 한국 청소년에서의 DEXA 로 측정한 비만과 복부비만 지방률의 절 단점을 구하려는 시도가 있었으나 그 수가 너무 적어 통계적의 의미 를 부여하기는 부족했다.
따라서 본 연구는 2008 ~ 2011 년 국민건강영양조사를 바탕으로 DEXA 를 이용하여 10 세 이상 18 세 이하 소아청소년에서 체지방량 과 몸통지방량을 측정한 것을 이용하여 우리나라 소아청소년에서 비만과 복부비만을 반영하는 체지방률과 복부지방률의 절단점을 알아보고자 본 연구를 시행하였다.
방 법
1. 연구대상
본 연구는 제 4 기 2 차년도 2008 년도, 제 4 기 3 차년도 2009 년, 제 5 기 1 차년도 2010 년도, 제 5 기 2 차년도 2011 년도 국민건강영양조 사 자료를 이용하였다. 국민건강영양조사는 건강면접조사, 보건의
식행태조사, 검진조사 및 영양조사로 구성되어 있다. 국민건강영양 조사에 참여한 10 세이상 18 세 이하의 청소년은 3895 명이고, 이중 에서 DEXA 를 시행한 사람은 2648 명이었으며, 10 세이상 18 세 이 하의 청소년 3895 명을 최종 연구대상자로 하였다.
2. 측정방법
본 연구에서 청소년의 비만은 2007 년 소아청소년 표준 성장도 표
1)를 이용하여 진단하였다. 비만은 2007 년 소아청소년 표준 성장 도표에서 성별, 연령별 체질량지수 95 백분위수 이상 또는 체질량 지수 25kg / m
2이상, 과체중은 성별 연령별 체질량지수 85 백분위 수 이상에서 95 백분위수 미만 또는 체질량지수 23kg / m
2이상에서 25kg / m
2미만으로 진단하였다. 소아비만도( obesity index )는 2007 년 소아청소년 표준 성장도표에서 신장별 체중의 50 백분위수를 표 준체중으로 하여 측정체중에서 신장에 따른 표준체중을 뺀 후 신장 에 따른 표준체중을 나눈 값에서 100 을 곱한 후 다시 100 을 더하여 계산하였다. 소아 복부비만은 2005 년 소아청소년 백분위수 분포
18)에서 성별 연령별 허리둘레 90 백분위수 이상으로 정의하였다.
3. 분석방법 및 통계
소아청소년의 일반적인 특성은 2008 년도부터 2011 년도 국민건 강영양조사 표본설계를 고려하여, 1 차 추출단위, 층화변수, 가중치 를 지정한 후 분석하였다.
DEXA 로 측정한 지방률과 비만 관련 지수와 대사 지표와의 연관 성은 성별과 연령을 보정한 후 Pearson ’ s correlation 을 이용하여 측 정하였고, 대사 지표 중에서 중성지방 측정치는 정규분포를 보이지 않아 자연로그로 변환한 값을 이용하였다.
DEXA 로 측정한 복부지방률은 몸통지방률( Trunk fat %)으로 추 정 간주하였고, 2005 년 소아청소년 백분위수 분포
18)에서 성별 연령 별 허리둘레 90 백분위수 이상을 정의하여 비교 분석하였다. DEXA 로 측정한 지방률의 비만과 복부비만의 절단점은 각 성별, 나이별 로 나누어 구하였다. 비만과 복부비만에 해당하는 체지방률과 몸통 지방률의 절단점을 찾기 위해 Receiver Operating Characteristics ( ROC ) curve 를 이용하였으며, 민감도와 특이도의 합이 가장 큰 지 점을 그 절단점으로 선택하였다.
19)통계분석은 SPSS for Windows 20 . 0 ( SPSS inc ., Chicago , IL , USA )을 이용하였으며, P 값이 0 . 05 미만인 경우 통계적으로 유의 한 것으로 정의하였다.
결 과
1. 일반적인 특징
총 3895 명의 10 ~ 18 세의 남녀가 대상이었고, 남아 2072 명
백래인 외. 한국 청소년에서 DEXA로 측정한 비만과 복부비만 지방률의 절단점:2008~2011년 국민건강영양조사 Korean Journal of Family Practice
KJFP
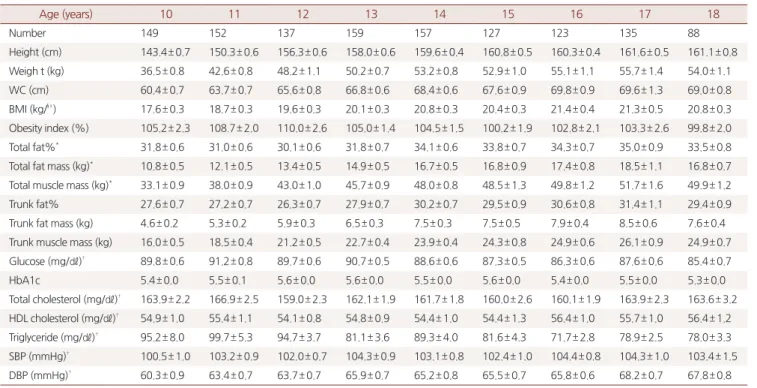
( 53 . 2 %), 여아 1823 명( 46 . 8 %)이었다. 체지방량과 몸통지방률은 남 아에서는 연령이 증가함에 따라 감소하는 경향을 보였고, 여아에서 는 연령이 증가함에 따라 증가하는 경향을 보였다. ( Table 1 , 2 ).
2. DEXA로 측정한 지방률과 비만 관련 지표와 대사증후군 간의 연관성 성과 나이를 보정한 후 체지방률, 몸통지방률과 다른 비만 관련 지표와의 상관관계를 보았을 때, 모든 비만 관련 지표에서 몸통지 방률이 체지방률보다 더 높은 관련성을 보였다. 체지방률과 몸통지 방률의 대사 관련 지표와의 상관관계를 보았을 때도, 몸통지방률 이 체지방률보다 더 높은 관련성을 보였고, 중성지방, 공복혈당, 수 축기 혈압은 양의 상관관계를 보였으며, High density lipoprotein ( HDL ) 콜레스테롤은 음의 상관관계를 보였다. 이는 몸통지방률이 체지방률보다 심혈관계 위험 인자에 보다 큰 영향을 미친다는 것을 알 수 있다.( Table 3 ).
3. 비만과 복부비만의 절단점
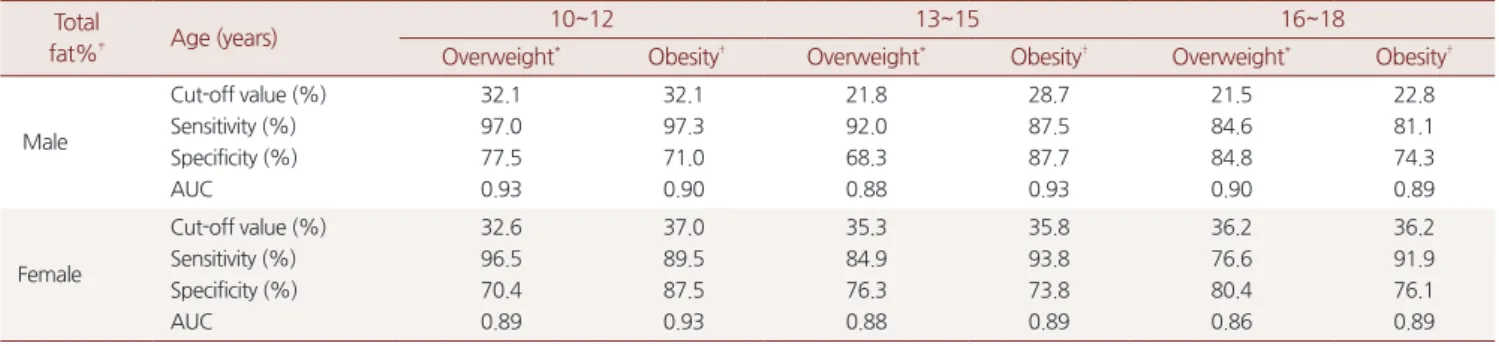
비만에 해당하는 체지방률은 남아 10 ~ 12 세에서 32 . 1 %, 13 ~ 15 세에서 28 . 7 %, 16 ~ 18 세에서 22 . 8 % 여아 10 ~ 12 세에서 37 . 0 %, 13 ~ 15 세에서 35 . 8 %, 16 ~ 18 세에서 36 . 2 %로 연령이 증가할수록 비만의 체지방률 절단점은 감소하였다. 비만에 해당하는 몸통지 방률은 남아 10 ~ 12 세에서 31 . 5 %, 13 ~ 15 세에서 24 . 2 %, 16 ~ 18
세에서 23 . 1 %이었고, 여아 10 ~ 12 세에서 35 . 4 %, 13 ~ 15 세에서 34 . 8 %, 16 ~ 18 세에서 33 . 3 %이었고, 복부 비만은 남아 10 ~ 12 세에 서 31 . 5 %, 13 ~ 15 세에서 24 . 3 %, 16 ~ 18 세에서 24 . 2 %이었고, 여아 10 ~ 12 세에서 35 . 0 %, 13 ~ 15 세에서 33 . 5 %, 16 ~ 18 세에서 33 . 3 %이 었다. 남녀 모두에서 체질량지수를 기준으로 한 비만과 복부둘레를 기준으로한 복부비만의 절단점은 거의 같은 양상을 보였다 ( Table 4 , 5 ).
고 찰
우리나라 소아청소년의 성별간 DEXA 로 측정한 체지방량과 체 지방률을 비교한 연구에서 체지방률은 남아는 12 세에 20 %로 정점 을 이루며 이후 성인 수준으로 감소하여 12 %가 된 반면에, 여아는 17 세경에 28 %로 정점을 이루며 이후 25 %로 안정화되었다.
14)또한 BIA 를 이용하여 부산 지역 7 ∼ 18 세의 소아청소년 1 , 083 명을 대상 으로 체지방률의 절단점을 연구한 결과를 살펴보면
17)남아는 24 % 이상, 여아는 30 % 이상을 비만의 절단점으로 보고하였다. 최근 BIA 를 이용하여 10 세에서 18 세 사이의 청소년들의 국민건강영양조사 자료를 분석한 연구 결과를 보면 남아에서는 연령이 증가함에 따라 체지방률은 감소하고 있고, 여아에서는 증가하는 보이고 있다.
19)그 러나 본 연구는 연령이 증가함에 따라 남녀 모두 감소하는 양상이나
Table 1. Characteristics of study subjects for maleAge (years) 10 11 12 13 14 15 16 17 18
Number 180 179 189 147 184 147 133 138 124
Height (cm) 142.3± 0.5 149.7± 0.7 156.4± 0.6 162.2± 0.7 169.2± 0.6 172.2± 0.6 173.6± 0.5 173.9± 0.6 173.7± 0.6 Weight (kg) 39.2± 0.8 45.4± 0.7 49.4± 1.0 54.5± 1.0 60.7± 1.1 62.4± 1.2 65.2± 1.1 66.5± 1.1 67.0± 1.1
WC (cm) 64.6± 0.8 67.7± 0.7 68.6± 0.9 69.8± 0.9 72.1± 0.8 72.5± 0.9 73.9± 0.8 74.8± 0.9 76.1± 0.9
BMI (kg/m2) 19.2± 0.3 20.1± 0.2 20.0± 0.3 20.6± 0.4 21.1± 0.3 20.9± 0.6 21.6± 0.3 22.0± 0.3 22.2± 0.3 Obesity index(%) 104.2± 2.2 112.7± 1.7 108.6± 2.2 107.5± 2.0 110.0± 1.6 105.1± 2.3 104.5± 1.8 103.1± 1.7 101.8± 1.7 Total fat%* 29.3± 1.0 29.8± 0.7 27.1± 1.2 24.2± 1.0 22.2± 0.8 19.4± 0.8 20.4± 0.9 20.6± 0.8 20.5± 0.7 Total fat mass (kg)* 10.7± 0.6 12.6± 0.4 12.7± 0.8 12.5± 0.7 13.2± 0.7 11.6± 0.7 12.9± 0.8 12.9± 0.7 12.6± 0.6 Total muscle mass (kg)* 34.3± 0.9 40.3± 0.8 44.6± 1.0 49.5± 1.1 56.0± 1.2 56.0± 1.3 59.7± 1.2 60.0± 1.2 59.3± 0.9 Trunk fat% 26.4± 1.1 26.9± 0.8 24.8± 1.2 22.0± 1.1 20.5± 0.8 18.1± 0.9 19.4± 0.9 19.7± 0.9 19.9± 0.7 Trunk fat mass (kg) 4.7± 0.4 5.6± 0.2 5.7± 0.4 5.5± 0.4 6.0± 0.4 5.3± 0.4 6.2± 0.4 6.2± 0.4 6.2± 0.3 Trunk muscle mass (kg) 16.6± 0.5 19.4± 0.4 21.4± 0.5 23.7± 0.6 27.1± 0.6 27.1± 0.7 29.6± 0.6 29.7± 0.6 29.7± 0.5 Glucose (mg/㎗)† 91.3± 0.4 92.1± 0.7 91.6± 0.5 91.5± 0.5 89.3± 0.4 89.7± 0.6 88.5± 0.6 88.5± 0.7 86.7± 0.7
HbA1c 5.4± 0.0 5.7± 0.1 5.5± 0.4 5.6± 0.0 5.4± 0.1 5.5± 0.0 5.4± 0.7 5.5± 0.0 5.4± 0.0
Total cholesterol (mg/㎗)† 170.6± 2.1 164.1± 2.8 155.5± 2.4 151.2± 2.0 146.0± 2.2 149.0± 2.7 152.5± 2.4 145.9± 2.3 152.9± 2.3 HDL cholesterol (mg/㎗)† 57.3± 0.9 55.3± 1.1 54.7± 1.0 51.8± 0.8 51.5± 0.8 50.3± 1.0 50.3± 1.2 50.0± 0.8 51.8± 0.7 Triglyceride (mg/㎗)† 85.3± 4.7 87.1± 4.8 79.3± 4.4 89.1± 5.5 81.3± 4.0 93.2± 5.4 94.7± 6.4 83.3± 4.5 83.2± 3.4 SBP (mmHg)† 100.9± 1.0 103.2± 0.7 105.0± 0.7 109.8± 0.8 109.8± 0.8 110.6± 0.8 112.1± 1.2 113.2± 1.1 114.5± 1.4 DBP (mmHg)† 61.1± 0.7 62.5± 0.7 63.1± 0.7 66.0± 0.9 66.7± 0.8 69.3± 0.7 71.4± 0.9 71.7± 0.8 73.3± 0.9 WC: waist circumference, BMI: body mass index
All value are mean±standard error except number.
*Total fat%, total fat mass and total muscle mass covered whole body except the head area.
† Some people were missing from the raw data.
?????
Korean Journal of Family Practice
KJFP
남아가 보다 더 감소하는 양상을 보였다.
기존 연구를 보면, 지방 분포에 따른 지방률이 체질량지수보다 도 비만 관련 지표나 대사 관련 지표와 연관성이 높다는 보고가 있 었다. 이탈리아의 5 ~ 19 세의 건강한 소아청소년을 대상으로 한 연 구에서는 같은 체질량지수라도 지방분포( Regional adiposity )의 차 이가 다양하였으며,
20)그리스의 연구에서는 허리둘레가 체질량지 수보다 심혈관 질환 위험인자를 더 잘 반영하였다고 하였다. 그리 고 스페인의 5 ~ 14 . 9 세의 소아청소년을 대상으로 한 연구에서도 복 부 지방이 심혈관 질환 위험인자와 관련이 있다고 보고하고 있다.
21)또한 일본에서 성인을 대상으로 한 연구에서 복부 내장지방의 양 이 체질량지수를 비롯한 다른 신체계측지표보다 대사 증후군에 더 유의한 위험 요소라는 보고
22)와 미국에서 14 명의 비만 여아와 10 명의 정상 여아를 대상으로 MRI 로 지방 분포를 계측하여 성별과 Tanner ’ s stage 등의 보정한 연구에서도 복부 지방이 비만 여아에 서 정상 여아에 비해 2 ~ 3 배 높았고, 대사 관련 지표와 연관성이 높 았으며, BMI 가 아닌 복부 지방과 허리엉덩이 둘레가 대사 관련 지 표와 연관성이 높았다.
23)우리나라에서 평균 연령 14 ∼ 15 세의 175 명의 청소년을 대상으로 한 연구에서 내장 지방은 혈압, 중성지방, HDL 콜레스테롤, 공복 인슐린과 homeostatic model assessment – insulin resistance ( HOMA - IR )와 독립적인 연관성이 있다는 보고
19)
등을 미루어 볼 때, 체지방률과 허리둘레가 체질량지수보다 비만 의 진단력을 더욱 높일 수 있다고 생각된다.
24)이번 연구는 우리나라 소아청소년에서 최초로 남녀 각 연령군의 비만과 복부비만에 해당하는 체지방률과 몸통지방율의 절단점을 제시하였다. 전국민을 표본 추출한 국민건강영양조사의 자료를 이 용하였기 때문에 기존의 조사 결과와 비교해서 우리나라 소아청소 년을 대표할 수 있는 장점이 있다. 하지만 제한점으로는, 첫째 국민 건강영양조사에서 3895 명의 소아청소년 중에서 2648 명이 DEXA 를 시행하여 연령별 집단의 숫자가 크지 않아 연령별로 비만, 과체 중의 분포가 차이가 있어 비만의 진단기준점을 초등학교 고학년, 중학생, 고등학생 3 그룹으로 나누어 구하였다. 둘째 사춘기 전이
Table 2. Characteristics of study subjects for female.Age (years) 10 11 12 13 14 15 16 17 18
Number 149 152 137 159 157 127 123 135 88
Height (cm) 143.4± 0.7 150.3± 0.6 156.3± 0.6 158.0± 0.6 159.6± 0.4 160.8± 0.5 160.3± 0.4 161.6± 0.5 161.1± 0.8 Weigh t (kg) 36.5± 0.8 42.6± 0.8 48.2± 1.1 50.2± 0.7 53.2± 0.8 52.9± 1.0 55.1± 1.1 55.7± 1.4 54.0± 1.1
WC (cm) 60.4± 0.7 63.7± 0.7 65.6± 0.8 66.8± 0.6 68.4± 0.6 67.6± 0.9 69.8± 0.9 69.6± 1.3 69.0± 0.8
BMI (kg/§³) 17.6± 0.3 18.7± 0.3 19.6± 0.3 20.1± 0.3 20.8± 0.3 20.4± 0.3 21.4± 0.4 21.3± 0.5 20.8± 0.3 Obesity index (%) 105.2± 2.3 108.7± 2.0 110.0± 2.6 105.0± 1.4 104.5± 1.5 100.2± 1.9 102.8± 2.1 103.3± 2.6 99.8± 2.0 Total fat%* 31.8± 0.6 31.0± 0.6 30.1± 0.6 31.8± 0.7 34.1± 0.6 33.8± 0.7 34.3± 0.7 35.0± 0.9 33.5± 0.8 Total fat mass (kg)* 10.8± 0.5 12.1± 0.5 13.4± 0.5 14.9± 0.5 16.7± 0.5 16.8± 0.9 17.4± 0.8 18.5± 1.1 16.8± 0.7 Total muscle mass (kg)* 33.1± 0.9 38.0± 0.9 43.0± 1.0 45.7± 0.9 48.0± 0.8 48.5± 1.3 49.8± 1.2 51.7± 1.6 49.9± 1.2 Trunk fat% 27.6± 0.7 27.2± 0.7 26.3± 0.7 27.9± 0.7 30.2± 0.7 29.5± 0.9 30.6± 0.8 31.4± 1.1 29.4± 0.9 Trunk fat mass (kg) 4.6± 0.2 5.3± 0.2 5.9± 0.3 6.5± 0.3 7.5± 0.3 7.5± 0.5 7.9± 0.4 8.5± 0.6 7.6± 0.4 Trunk muscle mass (kg) 16.0± 0.5 18.5± 0.4 21.2± 0.5 22.7± 0.4 23.9± 0.4 24.3± 0.8 24.9± 0.6 26.1± 0.9 24.9± 0.7 Glucose (mg/㎗)† 89.8± 0.6 91.2± 0.8 89.7± 0.6 90.7± 0.5 88.6± 0.6 87.3± 0.5 86.3± 0.6 87.6± 0.6 85.4± 0.7
HbA1c 5.4± 0.0 5.5± 0.1 5.6± 0.0 5.6± 0.0 5.5± 0.0 5.6± 0.0 5.4± 0.0 5.5± 0.0 5.3± 0.0
Total cholesterol (mg/㎗)† 163.9± 2.2 166.9± 2.5 159.0± 2.3 162.1± 1.9 161.7± 1.8 160.0± 2.6 160.1± 1.9 163.9± 2.3 163.6± 3.2 HDL cholesterol (mg/㎗)† 54.9± 1.0 55.4± 1.1 54.1± 0.8 54.8± 0.9 54.4± 1.0 54.4± 1.3 56.4± 1.0 55.7± 1.0 56.4± 1.2 Triglyceride (mg/㎗)† 95.2± 8.0 99.7± 5.3 94.7± 3.7 81.1± 3.6 89.3± 4.0 81.6± 4.3 71.7± 2.8 78.9± 2.5 78.0± 3.3 SBP (mmHg)† 100.5± 1.0 103.2± 0.9 102.0± 0.7 104.3± 0.9 103.1± 0.8 102.4± 1.0 104.4± 0.8 104.3± 1.0 103.4± 1.5 DBP (mmHg)† 60.3± 0.9 63.4± 0.7 63.7± 0.7 65.9± 0.7 65.2± 0.8 65.5± 0.7 65.8± 0.6 68.2± 0.7 67.8± 0.8 WC: waist circumference, BMI: body mass index All value are mean±standard error except number.
* Total fat%, total fat mass and total muscle masscovered whole body except the head area.
† Some people were missing from the raw data.
Table 3. Partial correlation coefficients between DEXA fat% and other obesity variables, factors of metabolic syndrome after controlling for sex and age.
Total fat%* Trunk fat%
correlation P-value correlation P-value Waist circumference 0.653 <0.001 0.721 <0.001
Glucose† 0.086 <0.001 0.102 <0.001
lnTriglyceride† 0.242 <0.001 0.286 <0.001 HDL cholesterol† - 0.161 <0.001 - 0.199 <0.001
SBP 0.117 <0.001 0.158 <0.001
DBP 0.022 0.353 0.044 0.056
BMI: body mass index, BP: blood pressure, lnTriglyceride: log transformed triglyceride, HDL: high density lipoprotein,
Pearson’s correlation adjusted for sex and age.
* Total fat% covered whole body except the head area.
† Some people were missing from the raw data.
백래인 외. 한국 청소년에서 DEXA로 측정한 비만과 복부비만 지방률의 절단점:2008~2011년 국민건강영양조사 Korean Journal of Family Practice
KJFP
나 후 남녀 간의 체지방 분포가 다르게 변하기 때문
15, 24)에 Tanner ’ s stage 등의 보정이 필요하다. 이는 향후 추가로 진행되는 국민건 강영양조사 결과를 합쳐서 분석한다면 DEXA 체지방의 정확한 분 포와 비만의 진단기준점을 구할 수 있을 것이다. 셋째 소아청소년 의 특성을 고려하지 않은 성별, 연령별 체질량지수 95 백분위수 이 상 또는 체질량지수 25kg / m
2이상을 비만의 기준으로 삼았다는 점 을 들 수 있다. 그리고 넷째 몸통 지방율으로 복부 지방량과 복부둘 레를 추정할 수는 있으나 복부 지방률 그리고 내장 지방으로 완전히 간주할 수는 없다는 점이다.
본 연구에서 우리나라 소아청소년에서 비만과 복부비만의 지방 률을 남녀에서 연령대별로 구하였다. 향후 연구에서는 소아청소년 에서 성, 연령, 성성숙도 등을 보정하여 체지방률과 복부지방률의 비만 기준점에 대한 연구가 필요하며, 좀 더 나아가 체질량지수가 아니라 심혈관질환의 발생위험을 기준으로 한 비만 기준점에 대한 전향적 연구가 필요할 것으로 판단된다.
요 약
연구배경: 소아기 비만은 성인 비만의 유병율을 높인다. 최근 한국 소아 청소년의 비만의 유병율이 높아지고 있어, 소아청소년에서 이 중에너지 방사선 흡수계측법( duel - energy X - ray absorptiometry , DEXA )으로 성별, 연령별 비만과 복부비만의 체지방률과 복부비만 률의 절단점을 알아보고자 하였다.
방법: 2008 ~ 2011 년 국민건강영양조사 자료를 이용하여, DEXA 로 체지방을 측정한 10 ~ 18 세의 소아청소년 2648 명을 포함한 10 ~ 18 세의 소아청소년 3895 명을 대상으로 체지방율, 몸통지방율을 측 정하여 성별, 연령별로 따른 체질량지수와 허리둘레를 표준( Gold standard )으로 하여 Receiver Operating Characteristics ( ROC ) curve 를 통해 비만과 복부비만 진단에 대한 민감도와 특이도가 가 장 높은 절단점을 구하였다. 또한 성과 연령을 보정 후 체지방률, 몸통지방율과 대사 관련 지표인 공복혈당, 중성지방, HDL 콜레스 테롤, 혈압과의 상관관계를 조사하였다.
Table 4. The accuracy of the diagnosis for obesity using total fat% by DEXA compared with the obesity diagnosed by BMI.
Total
fat%‡ Age (years) 10~12 13~15 16~18
Overweight* Obesity† Overweight* Obesity† Overweight* Obesity†
Male
Cut-off value (%) Sensitivity (%) Specificity (%) AUC
32.1 97.0 77.5 0.93
32.1 97.3 71.0 0.90
21.8 92.0 68.3 0.88
28.7 87.5 87.7 0.93
21.5 84.6 84.8 0.90
22.8 81.1 74.3 0.89
Female
Cut-off value (%) Sensitivity (%) Specificity (%) AUC
32.6 96.5 70.4 0.89
37.0 89.5 87.5 0.93
35.3 84.9 76.3 0.88
35.8 93.8 73.8 0.89
36.2 76.6 80.4 0.86
36.2 91.9 76.1 0.89 DEXA: duel energy X-ray absorptiometry, BMI: body mass index, AUC: area under the curve
* Overweight: BMI¡Ã 85th percentile or BMI¡Ã 23
† Obesity: BMI¡Ã 95th percentile or BMI¡Ã 25
‡ Total fat% covered whole body except the head area.
Table 5. The accuracy of the diagnosis for obesity using trunk fat% by DEXA compared with the obesity diagnosed by BMI and abdominal obesity by waist circumference.
Age (years) 10~12 13~15 16~18
Obesity* Abd. obesity† Obesity* Abd. obesity† Obesity* Abd. obesity†
Male
Cut-off value (%) Sensitivity (%) Specificity (%) AUC
31.5 100 76.8 0.93
31.5 100 25.1 0.90
24.2 93.8 87.7 0.93
24.3 100 26.6 0.96
23.1 85.7 85.8 0.91
24.2 100 21.1 0.94
Female
Cut-off value (%) Sensitivity (%) Specificity (%) AUC
35.4 100 90.8 0.96
35.0 69.6 11.3 0.89
34.8 90.6 85.0 0.93
33.5 93.8 21.7 0.91
33.3 91.9 79.2 0.91
33.3 90.9 22.2 0.91 DEXA: duel energy X-ray absorptiometry, BMI: body mass index, AUC: area under the curve
* Obesity: BMI¡Ã 95th percentile or BMI¡Ã 25
† Abdominal obesity: waist circumference ≥90th percentile for age
?????
Korean Journal of Family Practice
KJFP
결과: 비만에 해당하는 DEXA 의 체지방률은 남아 10 ~ 12 세에서 32 . 1 %, 13 ~ 15 세에서 28 . 7 %, 16 ~ 18 세에서 22 . 8 % 여아 10 ~ 12 세 에서 37 . 0 %, 13 ~ 15 세에서 35 . 8 %, 16 ~ 18 세에서 36 . 2 %로 연령이 증가할수록 비만의 체지방률 절단점은 감소하였다. 비만에 해당하 는 몸통지방률은 남아 10 ~ 12 세에서 31 . 5 %, 13 ~ 15 세에서 24 . 2 %, 16 ~ 18 세에서 23 . 1 %이었고, 여아 10 ~ 12 세에서 35 . 4 %, 13 ~ 15 세 에서 34 . 8 %, 16 ~ 18 세에서 33 . 3 %이었고, 복부 비만은 남아 10 ~ 12 세에서 31 . 5 %, 13 ~ 15 세에서 24 . 3 %, 16 ~ 18 세에서 24 . 2 %이었고, 여아 10 ~ 12 세에서 35 . 0 %, 13 ~ 15 세에서 33 . 5 %, 16 ~ 18 세에서 33 . 3 %이었다. 남녀 모두에서 체질량지수를 기준으로 한 비만과 허 리둘레를 기준으로한 복부비만의 절단점은 거의 같은 양상을 보였 다. 몸통지방률이 체지방률보다 대사 관련 지표에서 더 높은 상관 관계를 보였다.
결론: 우리나라 소아청소년 10 ~ 18 세에서 비만과 복부비만의 체지방 률과 몸통지방율의 절단점은 과거 연구에서 제시한 값보다 낮았다.
중심단어: 소아비만, 체지방률, 이중에너지 방사선 흡수계측, 절단점
REFERENCES
1. Mi Ae Chu, Byung-Ho Choe 2010 Obesity and Metabolic Syndrome among Children and Adolescents in Korea. J Korean Med Assoc 2010; 53(2): 142 - 152
2. Moon JS, Lee SY, Nam CM, Choi JM, Choe BK, Seo JW, et al. 2007 Korean National Growth Charts: review of developmental process and an outlook. Korean J Pediatr AID - 10.3345/kjp.2008.51.1.1 [doi]
2008;51(1):1-25.
3. Oh K, Jang MJ, Lee NY, Moon JS, Lee CG, Yoo MH, et al.
Prevalence and trends in obesity among Korean children and adolescents in 1997 and 2005. Korean J Pediatr AID - 10.3345/
kjp.2008.51.9.950 [doi] 2008;51(9):950-5.
4. Seo MJ, Seong JW, Sohn KJ, Ko BJ, Han JH, Kim SM. Prevalence of the Metabolic Syndrome in Korean Children and Adolescents:
Korea National Health and Nutrition Survey 2001. J Korean Acad Fam Med 2006;27(10):798-806.
5. Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The relation of overweight to cardiovascular risk factors among children and adolescents: the Bogalusa Heart Study. Pediatrics 1999;103(6 Pt 1):1175-82.
6. Veldhuis JD, Roemmich JN, Richmond EJ, Rogol AD, Lovejoy JC, Sheffield-Moore M, et al. Endocrine control of body composition in infancy, childhood, and puberty. Endocr Rev 2005;26(1):114-46.
7. Caprio S, Hyman LD, McCarthy S, Lange R, Bronson M, Tamborlane WV. Fat distribution and cardiovascular risk factors in obese adolescent girls: importance of the intraabdominal fat depot.
Am J Clin Nutr 1996;64(1):12-7.
8. Kim DG, Lee KM, Jung SP. Clinical Significance of Abdominal
Deep Subcutaneous Adipose Tissue in the Obese: Associations with Cardiovascular and Risk Factors. J Korean Acad Fam Med 2007;28(2):100-5.
9. Van der Kooy K, Seidell JC. Techniques for the measurement of visceral fat: a practical guide. Int J Obes Relat Metab Disord 1993;17(11):187-96.
10. Plourde G. The role of radiologic methods in assessing body composition and related metabolic parameters. Nutr Rev 1997;55(8):289-96.
11. Kim CW, Park KH, Ju YS, Song HJ, Paek YJ, Choi JW, et al. Percent Body Fat and Abdominal Circumference Cutoff Points Accounted for 85th and 95th Percentile of Body Mass Index in One City of Gyeonggi Province. J Korean Acad Fam Med 2008;29(7):492-8.
12. Lee K, Lee S, Kim SY, Kim SJ, Kim YJ. Percent body fat cutoff values for classifying overweight and obesity recommended by the International Obesity Task Force (IOTF) in Korean children. Asia Pac J Clin Nutr 2007;16(4):649-55.
13. Svendsen OL, Haarbo J, Hassager C, Christiansen C. Accuracy of measurements of body composition by dual-energy x-ray absorptiometry in vivo. Am J Clin Nutr 1993;57(5):605-8.
14. Jebb SA. Measurement of soft tissue composition by dual energy X-ray absorptiometry. Br J Nutr 1997;77(2):151-63.
15. Lim JS, Hwang JS, Cheon GJ, Lee JA, Kim DH, Park KD, et al.
Gender differences in total and regional body composition changes as measured by dual-energy x-ray absorptiometry in Korean children and adolescents. J Clin Densitom 2009;12(2):229-37.
16. Kim CW, Park KH, Ju YS, Song HJ, Paek YJ, Choi JW, et al. Percent Body Fat and Abdominal Circumference Cutoff Points Accounted for 85th and 95th Percentile of Body Mass Index in One City of Gyeonggi Province. J Korean Acad Fam Med 2008;29(7):492-8.
17. Lee K, Lee S, Kim SY, Kim SJ, Kim YJ. Percent body fat cutoff values for classifying overweight and obesity recommended by the International Obesity Task Force (IOTF) in Korean children. Asia Pac J Clin Nutr 2007;16(4):649-55.
18. Korea Center for Disease Control and Prevention, The Korean Pediatric Society, The Committee for the Development of Growth Standard for Korean
Children and Adolescents. 2007 Korean Children and Adolescents Growth Standard (commentary for the development of 2007 growth chart). [Government report online]. Seoul: Division of Chronic Disease Surveillance; 2007 Nov. Available from: URL:http://www.
cdc.go.kr/
19. Altman DG, Bland JM. Diagnostic tests 3: receiver operating characteristic plots. BMJ 1994;309(6948):188.
20. Pietrobelli A, Faith MS, Allison DB, Gallagher D, Chiumello G, Heymsfield SB. Body mass index as a measure of adiposity among children and adolescents: a validation study. J Pediatr 1998;132(2):204-10.
21. J. Revenga-Frauca1, E.M. Gonzalez-Gil1, G. Bueno-Lozano2,3, P.
De Miguel-Etayo et al Abdominal fat and metabolic risk in obese children and adolescents, J Physiol Biochem, 65 (4), 415-420, 2009 22. Matsushita Y, Nakagawa T, Yamamoto S, Takahashi Y, Yokoyama T,
Noda M et al. Associations of visceral and subcutaneous fat areas with the prevalence of metabolic risk factor clustering in 6,292 Japanese individuals: the Hitachi Health Study. Diabetes Care 2010;33(9):2117-9.
백래인 외. 한국 청소년에서 DEXA로 측정한 비만과 복부비만 지방률의 절단점:2008~2011년 국민건강영양조사 Korean Journal of Family Practice
KJFP
23. Sonia Caprio, Lauren D Hyman, Sherley McCarthy et.al. Fat distribution and cardiovascular risk factors in obese adolescent girls: importance of the intraabdominal fat depot. Am J Clin Nutr l996;64:12-7.
24. Ley CJ, Lees B, Stevenson JC. Sex- and menopause-associated changes in body-fat distribution. Am J Clin Nutr 1992;55(5):950- 4.
25. Clasey JL, Bouchard C, Teates CD, Riblett JE, Thorner MO, Hartman ML, et al. The use of anthropometric and dual-energy X-ray absorptiometry (DXA) measures to estimate total abdominal and abdominal visceral fat in men and women. Obes Res 1999;7(3):256-64.
26. Ito H, Nakasuga K, Ohshima A, Maruyama T, Kaji Y, Harada M, et al. Detection of cardiovascular risk factors by indices of obesity obtained from anthropometry and dual-energy X-ray absorptiometry in Japanese individuals. Int J Obes Relat Metab Disord 2003;27(2):232-7.
27. Kim JA, Park HS. Association of abdominal fat distribution and cardiometabolic risk factors among obese Korean adolescents.
Diabetes Metab 2008;34(2):126-30.
28. Ok-Kyeong Yu, Yang-Keun Rhee, Tae-Sun Park and Youn- Soo Cha. Comparisons of obesity assessments in over-weight elementary students using anthropometry, BIA, CT and DEXA, Nutrition Research and Practice (Nutr Res Pract) 2010;4(2):128-135 29. Williams DP, Going SB, Lohman TG, Harsha DW, Srinivasan SR,
Webber LS, et al. Body fatness and risk for elevated blood pressure, total cholesterol, and serum lipoprotein ratios in children and adolescents. Am J Public Health 1992;82(3):358-63.
30. Savva SC, Tornaritis M, Savva ME, Kourides Y, Panagi A, Silikiotou N, et al. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int J Obes Relat Metab Disord 2000;24(11):1453- 8.