경골 간부 쐐기형 골절
송상준 윤형구 한수홍 박형근 이인석
포천중문의과대학교 분당차병원 정형외과학교실
목 적: 경골 간부 쐐기형 골절로 교합성 골수강 내 금속정 고정술을 시행한 환자의 골유합 기간을 조사하고 이에 영향을 미치는 인자를 분석하고자 한다.
대상 및 방법: 경골 간부 쐐기형 골절로 교합성 골수강 내 금속정 고정술을 시행 받은 후 1년 이상 추시가 가능하였던 32예를 대상으로 하였다. 방사선 사진상 쐐기형 골편의 직경 (%)과 길이 (mm)를 측정하였고, 수술 전, 후 쐐기형 골편의 전위 정도 (mm)를 측정하였다.
주골편과 쐐기형 골편의 골유합 기간을 조사하였고 (paired t-test), 쐐기형 골편의 직경, 길이, 수술 전,후 전위 정도에 따른 골유합 기간을 비교하였다 (상관분석).
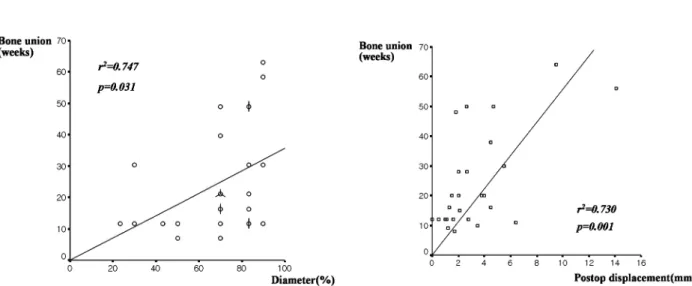
결 과: 주골편 사이의 골유합 기간은 평균 술 후 15.3주 (6∼56주)였고, 주골편과 쐐기형 골편 사이의 골유합 기간은 술 후 평균 24.2주 (8∼64주)였다 (p=0.005). 쐐기형 골편의 길이와 골유합 기간의 상관 관계는 유의하지 않았으나 (p=0.681), 쐐기형 골편의 직경이 클수록 쐐기형 골편의 골유합 기간이 길었다 (r2=0.747, p=0.031), 쐐기형 골편의 수술 전 전위와 골유합 기간의 상관 관계는 유의하지 않았으나 (p=0.574), 수술 후 전위가 클수록 쐐기형 골편의 골유합 기간이 길었다 (r2=0.730, p=0.001).
결 론: 폐쇄성 골수강 내 금속정 고정술로 경골 간부 쐐기형 골절의 치료 시 쐐기형 골편의 직경이 클 경우 골편의 전위에 대한 세심한 주의가 필요하리라 생각된다.
색인 단어: 경골, 간부, 쐐기형 골절, 골수강 내 금속정 삽입술
Wedge Tibial Shaft Fractures Treated with Interlocking IM Nailing
Sang Jun Song, M.D., Hyung Ku Yoon, M.D., Soo Hong Han, M.D., Hyung Kun Park, M.D., In Seok Lee, M.D.
Department of Orthopedic Surgery, Bundang CHA Hospital, College of Medicine, Pochon CHA University, Seongnam, Gyeonggi-do, Korea
Purpose: To investigate the bone union time of patients treated with interlocking intramedullary nailing in wedged tibial shaft fracture and to evaluate the factors that influence this result.
Materials and Methods: 32 patients treated with interlocking intramedullary nailing for wedge tibial shaft fracture were reviewed with a follow-up period of more than 1 year. Radiographic results were assessed with diameter (%) and length (mm) of wedge fragment, pre and postoperative displacement (mm) of wedge fragment. We also checked the bone union time of the main fragment and the wedge fragment (paired t-test). We investigated the bone union time acocording to the diameter, length of wedge fragment, pre and postopertvie displacement (correlation analysis).
Results: Bone union time of the main fragments averaged 15.3 weeks (6∼53 weeks) and that of wedge fragment averaged 24.2 weeks (8∼64 weeks) (p=0.005). There was no correspondence between wedge fragment diameter and bone union time (p=0.681), but the bone union time of wedge fragment increased in proportion to its diameter (r
2=0.747, p=0.031). There was no correspondence between preoperative displacement of wedge fragment and bone union time (p=0.574), but the bone union time increased in proportion to postoperative displacement of wedge fragment (r
2=0.730, p=0.001).
Conclusion: Wedge fragments need longer time for bone union than main fragments in interlocking intramedullary nailing for wedge tibial shaft fractures. We need to pay attention to the displacemet of fragments in treating tibial shaft fractures with large wedge fragment.
Key Words: Tibia, Shaft, Wedge fracture, Interlocking intramedullary nailing
322 통신저자:한 수 홍
경기도 성남시 분당구 야탑동 351
포천중문의과대학교 분당차병원 정형외과학교실 Tel:031-780-6085․Fax:031-708-3578 E-mail:Tesstore@empal.com
*본 논문의 요지는 2005년도 대한정형외과학회 추계학술대회에서 발표되었음.
Address reprint requests to:Soo Hong Han, M.D.
Department of Orthopedic Surgery, Bundang CHA Hospital, College of Medicine, Pochon CHA University, Seongnam 463-712, Korea Tel:82-31-780-6085․Fax:82-31-708-3578
E-mail:Tesstore@empal.com
서 론
경골 골절은 장관골 골절 중 가장 빈도가 높은 골절로써 해부학적 위치 및 기능상 외상에 노출되기가 쉬우며 산업 재 해와 교통사고의 증가에 따라 그 빈도가 증가하는 추세이 다8). 골수강 내 금속정 고정술은 경골 간부 골절의 치료를 위해 보편적으로 사용되고 있고, 그 결과 또한 양호한 것으 로 알려져 있다9,11,19). 그러나, 경골 간부 쐐기형 골절에서 폐 쇄성 골수강 내 금속정 고정술은 쐐기형 골편이 고정되지 않 으며, 쐐기형 골편의 분쇄, 전위, 혈행 감소와 연부조직 손상 등이 동반되어 단순 골절에 비해 치료기간이 길고 지연유합, 불유합 및 부정유합 등과 같은 합병증을 초래할 수 있다7). 저 자들도 쐐기형 골편의 과도한 전위와 불안정성 등으로 쐐기 형 골편의 골유합이 지연되는 것을 종종 경험하였다 (Fig. 1).
이에 저자들은 경골 간부 쐐기형 골절에서 교합성 골수강 내 금속정 고정술로 치료한 환자의 임상적, 방사선학적 결과와 골유합 기간을 조사하고 이에 영향을 미치는 인자를 분석하 고자 하였다.
대상 및 방법
1. 연구대상
2000년 5월부터 2004년 9월까지 경골 간부 쐐기형 골절로 교합성 골수강 내 금속정 고정술을 시행 받은 후 1년 이상 추시가 가능하였던 32예를 대상으로 하였다. 나이는 평균 42
세 (16∼77세)였고 남자가 23예, 여자가 9예였다. 추시 기간 은 평균 2년 1개월 (1년∼4년 6개월)이었다. 우측이 18예, 좌측이 14예였고 수상 원인은 교통사고 19예, 낙상 7예, 스 포츠 손상 3예, 기타 3예였다. 비개방성 골절이 20예, 개방성 골절이 12예였고, Gustilo-Anderson 분류8)상 I형이 3예, II형 이 5예, IIIa형이 4예였다. 골절의 형태는 AO 분류상 B1 9예, B2 12예, B3 11예였다. 금속정의 삽입은 비확공성 삽입술 16예, 확공성 삽입술 16예 시행하였고, 개방성 골절 12예는 모두 비확공성 삽입술로 시행하였고, 비개방성 골절 20예 중 16예는 확공성 삽입술, 4예는 비확공성 삽입술을 시행하 였다.
2. 수술 방법 및 수술 후 처치
모든 예에서 골절면의 안정성을 위하여 근위 두 개, 원위 두개 이상의 교합나사를 사용하였다. 동반된 비골 골절이 원 위부에 위치하여 골절 및 족관절의 불안정성이 예상될 때는 금속판으로 비골을 고정하였다. 수술 후 2일째부터 족근 관 절 및 슬관절의 관절 운동을 시행하였고, 수술 후 2주부터 부분 체중 부하를 허용하였다. 완전 체중 부하 보행은 수술 후 8∼12주에 시행하였고, 수술 후 매 2주에서 4주 간격으로 추시 관찰을 하였다.
3. 연구방법
방사선 사진상 영상 저장 전송 체계 (PACS, Picture Ar- Fig. 1. (A) The preoperative radiograph of a 52-year-old female shows wedge tibial shaft fracture.
(B) The postoperative radiograph shows the fixation of the tibia fracture with a locked intramedullary nailing. The wedge fragment is not fixed and have moderate displacement.
(C) The proximal and distal main fragments are united (M), but the wedge fragment with a large amount of displacement (W) is not united to main fragments at POD 1 year 2 months.
chiving and Communications System)를 이용하여 쐐기형 골편의 직경 (%)과 길이 (mm)를 측정하였고, 수술 전, 후 쐐 기형 골편의 전위 정도 (mm)를 측정하였다 (Fig. 2). 임상적 평가는 슬관절과 족근관절의 관절운동범위를 조사하였고, 방 사선학적 평가는 내외반각과 전후굴각을 측정하였다. 골유합 은 임상적으로 골절 부위에 동통 및 압통이 없고, 골절부의 가동성이 없으며, 방사선학적으로 골소주가 연결된 경우로 정의하였다. 근위 주골편과 원위 주골편 사이의 골유합 기간 (M time)을 조사하였고, 근위 및 원위 주골편과 쐐기형 골편 사이의 골유합 기간 (W time)을 조사하여 이를 비교하였다 (paired t-test) (Fig. 1C). 쐐기형 골편의 양 단면을 경골 영 양 동맥에 가까운 단면과 먼 단면, 그리고 전위가 큰 단면과 작은 단면으로 분류하였고, 먼저 골유합되는 단면을 조사하 였다. 쐐기형 골편의 직경, 길이, 수술 전, 후 전위 정도에 따른 골유합 기간을 비교하였다 (상관분석). 비개방성 골절 과 개방성 골절에 따른 골유합 기간을 비교하였고, 비확공성 과 확공성 골수강내 금속정 고정술에 따른 골유합 기간을 비 교하였다 (Student t-test). 수술 후 합병증과 골수강내 금속 정 고정술 후 추가적인 수술이 필요했던 경우를 조사하였다.
결 과
1. 골절의 양상
쐐기형 골편의 직경 비율은 평균 69.0±18.5% (20.0∼
90.0%)이었고, 길이는 평균 49.9±53.5 mm (11.2∼106.0 mm)이었다. 쐐기형 골편의 수술 전 전위는 평균 8.6±7.7 mm (0.5∼32.0mm)이었고, 수술 후 전위는 평균 3.2±2.8 mm (0.0∼14.1mm)이었다 (Table 1).
2. 임상적 결과
슬관절과 족근관절의 관절운동범위는 30예에서 건측과 동 일한 관절운동범위를 보였고, 슬관절의 운동범위 감소 (0∼
120o)가 1예, 족근관절의 운동범위 감소 (신전 10∼굴곡 30o) 가 1예 있었다 (Table 1).
3. 방사선학적 결과
최종 추시 시 경골 간부의 내외반각은 평균 외반 1.7±
3.2o (내반 5∼외반 8o)이었고, 5o이상의 변형이 1예 있었다 (Table 1). 최종 추시 시 전후굴각은 평균 전굴 1.2±3.8o (전굴 9∼후굴 7o)이었고, 5o 이상의 변형이 1예 있었다 (Table 1).
4. 골유합 기간
M time은 평균 술 후 15.3주 (6∼56주)였고, W time은 평 균 술 후 24.2주 (8∼64주)이었다 (p=0.005). 경골 영양 동 맥을 중심으로 쐐기형 골편의 위치에 따른 골편 양 단면의 골유합 순서는 경골 영양 동맥에 가까운 단면이 먼저 골유합 되는 경우 18예, 먼 단면이 먼저 골유합 되는 경우 10예, 동 시에 골유합 되는 경우 4예였다. 전위 정도에 따른 쐐기형 골편 양 단면의 골유합 순서는 전위가 작은 단면이 먼저 골 유합 되는 경우 28예, 동시에 골유합 되는 경우 4예였다. 쐐 기형 골편의 길이와 골유합 기간의 상관 관계는 유의하지 않 았으나 (p=0.681), 쐐기형 골편의 직경이 클수록 쐐기형 골 편의 골유합 기간이 길었다 (r2=0.747, p=0.031) (Fig. 3A).
쐐기형 골편의 수술 전 전위와 골유합 기간의 상관 관계는 Fig. 2. The length, diameter and displacement of wedge fragment is measured in anteroposterior and lateral views of X-ray.
(A) The length of wedge fragment is measured by “a (mm)”, and the diameter of wedge fragment is measured by “b/c (%)”.
(B) The preoperative displacement is measured by “d (mm)”, and the postoperative displacement is measured by “e (mm)”.
유의하지 않았으나 (p=0.574), 수술 후 전위가 클수록 쐐기형 골편의 골유합 기간이 길었다 (r2=0.730, p=0.001) (Fig. 3B).
개방성 골절군의 M time과 W time은 비개방성 골절군에 비해 길었고 (p<0.05) (Table 2), 비확공성 금속정 고정술 시행군의 M time과 W time은 확공성 금속정 고정술 시행군 에 비해 길었다 (p<0.05) (Table 3A), 비개방성 골절군 만 의 비교 시 비확공성 금속정 고정술 시행군 (4예)은 M time 과 W time이 각각 평균 16.4주, 21.7주로 확공성 금속정 고
정술 시행군보다 길었으나, 통계적으로 유의하지는 않았다 (p>0.05) (Table 3B).
5. 합병증
합병증으로 심부 감염 1예, 교합 나사의 파단 2예, 주 골 편의 지연 유합 1예, 쐐기형 골편의 지연 유합 2예 있었다.
추가적인 수술로 심부 감염이 있었던 1예에서 변연절제술과 Table 1. The types of wedge fractures, modality of intramedullary nailing, clinical and radiographic results
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
R AO Closed Modality of a b/c d e Knee Ankle Postop Postop
/L /Open IM nailing (mm) (%) (mm) (mm) ROM ROM valgus AP
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 F/52 L B1 Open I Unreamed 90 55.5 3.2 2.8 Full Full 2o 4o
2 M/64 R B1 Closed Reamed 20 77.4 12.2 3.5 Full Full 4o 3o
3 F/34 R B2 Closed Unreamed 70 11.6 4 3.8 Full Full -2o 3o
4 F/23 R B2 Closed Reamed 50 11.2 2.3 0.5 Full Full 3o 1o
5 M/38 L B2 Open IIIa Unreamed 90 54 7.7 5.5 120o Full 5o 4o
6 F/54 R B3 Closed Reamed 70 32.6 14 3.8 Full Full -1o -4o
7 M/47 R B3 Closed Reamed 70 76 4.1 1 Full Full 4o -3o
8 F/67 L B1 Closed Reamed 40 83 5 1.6 Full Full -2o -4o
9 M/18 L B2 Closed Unreamed 80 32.9 18.6 6.4 Full Full 1o 4o
10 M/42 R B1 Closed Reamed 30 63.3 0.5 0 Full Full -4o 4o
11 M/31 L B2 Open IIIa Unreamed 70 78.5 1 1.3 Full Full 8o -7o
12 M/61 L B3 Closed Reamed 80 43.9 12.5 2 Full Full 2o 3o
13 M/47 R B3 Open II Unreamed 70 22.3 6 4 Full Full 3o 5o
14 F/44 L B1 Closed Reamed 30 35 4 2 Full Full -1o 2o
15 M/23 L B3 Open IIIa Unreamed 70 65 6.4 4.5 Full Full 2o 2o
16 M/32 R B1 Closed Reamed 69 49.9 8.6 3.2 Full Full 4o 4o
17 M/34 L B3 Closed Unreamed 90 69.5 27.4 14.1 Full 40o -3o 5o
18 M/41 R B3 Closed Reamed 80 106 5.1 4.5 Full Full -5o 9o
19 M/27 R B2 Open II Unreamed 70 23.5 2.3 1.5 Full Full 2o -4o
20 M/46 L B2 Closed Reamed 70 34.7 4.5 3 Full Full 2o 3o
21 M/48 R B3 Open II Unreamed 80 48.6 6.3 1.8 Full Full 2o -4o
22 M/77 R B2 Open I Unreamed 90 36.4 9.2 2.1 Full Full 5o 2o
23 F/52 R B1 Closed Reamed 90 94.2 13.1 9.5 Full Full 4o -5o
24 M/59 R B3 Open II Unreamed 80 35.2 6.3 4.7 Full Full 2o 4o
25 M/21 L B2 Open II Unreamed 80 16.3 3.8 1.5 Full Full 4o 3o
26 F/28 R B3 Open I Unreamed 70 35.3 24.7 1.7 Full Full 5o 2o
27 M/55 L B2 Closed Reamed 80 40.2 7.3 2.7 Full Full -4o 3o
28 F/24 R B2 Closed Unreamed 70 43.8 5.3 2.1 Full Full 3o 5o
29 M/35 L B2 Closed Reamed 60 53.9 5.4 2.6 Full Full -3o -1o
30 M/28 L B1 Closed Reamed 70 61.2 10.7 2.6 Full Full 4o -5o
31 M/58 R B3 Open IIIa Unreamed 50 43.4 32 1.2 Full Full 3o 3o
32 M/35 R B1 Closed Reamed 80 62 2.6 1.1 Full Full 4o -4o
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ AO: AO classification, Open: Gustilo-Anderson classification, a: Length of wedge fragment, b/c: Diameter of wedge fragment, d:
Preoperative displacement of wedge fragment, e: Postoperative displacement of wedge fragment, Postop valgus: Postoperative varus-valgus angle (varus angulation represents by negative number), Postop AP: Postoperative anterior-posterior angle (posterior angulation represents by negative number).
연부 조직 피판술을 시행하였고, 주 골편의 지연 유합이 있 었던 1예는 술 후 12주에 역동화를 시행하였고, 쐐기형 골편 의 지연 유합이 있었던 2예는 자가골 이식을 시행하였다.
고 찰
경골 간부의 쐐기형 골절은 하나 이상의 중간 골편 (inter- mediate fragment)을 가지고 근위 주골편과 원위 주골편 사 이에 접촉이 있는 AO 분류 B 골절로 정의된다. AO 분류 B1 의 나선상 골절은 소위 나비형 골편 (butterfly fragment)을 가지며 회전력에 의해 나선상 골절이 발생하고, 환자가 앞으 로 쓰러질 때 전방에, 뒤로 쓰러질 때 후방에 나비형 골편이 발생한다고 한다6). AO 분류 B2의 bending 골절은 압력과 굴곡력이 같이 작용하여 사횡상 골절을 이루고, 사상 골편이 원위부 골편에 감입될 때 부러지면서 쐐기형 골편이 생길 수 있다24). 직접 외상에 의해 발생하는 경우가 많으므로 심한
연부 조직 손상을 동반하는 고에너지 손상으로 분류한다16). AO 분류 B3 fragmented 골절은 쐐기형 골편의 분쇄를 보이 지만 주 골편 사이의 접촉이 남아 있어 AO 분류 C 골절과 구분한다.
골유합은 골절면의 접촉, 골절의 해부학적 안정성, 원활한 혈액 순환에 의해 영향을 받으며, 골절면의 과도한 전위, 부 정확한 정복, 부족한 혈액 공급은 지연 유합이나 불유합의 원인이 된다3,20). 경골 간부 쐐기형 골절에서 쐐기형 골편은 Fig. 3. Bone union time is correlated to the diameter and postoperative displacement of wedge fragments.
(A) Bone union time of wedge fragment is increased in proportion to its diameter (r2=0.747, p=0.031).
(B) Bone union time is increased in proportion to postoperative displacement of wedge fragment (r2=0.730, p=0.001).
Table 2. Bone union time between closed and open fractures (weeks) ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
M time W time
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Closed fractures (n=20) 13.5±12.1 20.9±14.3 Open fractures (n=12) 17.6±10.9 25.1±15.6
p-value 0.040 0.031
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ M time: Bone union time between proximal and distal main fragments, W time: Bone union time between main fragment and wedge fragment.
Table 3. (A) Bone union time between unreamed and reamed
nailings in all cases (weeks)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
M time W time
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Unreamed nailings (n=16) 18.5±14.0 28.9±18.8 Reamed nailings (n=16) 9.1±2.1 15.0±7.1
p-value 0.023 0.023
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ (B) Bone union time between unreamed and reamed nailings
in closed fractures (weeks)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
M time W time
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Unreamed nailings (n=4) 16.4±17.7 21.7±17.1 Reamed nailings (n=16) 9.1±2.1 15.0±7.1
p-value 0.214 0.247
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ M time: Bone union time between proximal and distal main fragments, W time: Bone union time between main fragment and wedge fragment.
폐쇄성 골수강 내 금속정 고정술 시 고정되지 않으며, 쐐기 형 골편의 분쇄, 과도한 전위, 혈행 감소와 연부조직 손상 등 이 동반되어 단순 골절에 비해 골유합 기간이 길고 지연유합, 불유합 및 부정유합 등과 같은 합병증을 초래할 수 있다7,15). 경골 간부 분쇄 골절에서 골수강 내 금속정 고정술 시 골 절부위의 고정은 금속정이 골수강 내로 진입되면서 간접적 으로 골절이 정복된다. 따라서 간부의 분쇄 정도는 각형성보 다는 단축에 더 영향을 미치지만 분쇄 정도가 심한 골절은 주골편간의 접촉이 적어 금속정과 피질골간의 견고한 고정 이 힘들고 금속정의 삽입이 골편의 장축에 평행이 덜 되게 삽입되는 수가 있어 각 변형이 증가되는 결과를 가져온다10). 저자들의 경우 내외반각은 평균 외반 1.7±3.2o (내반 5∼외 반 8o)이었고, 전후굴각은 평균 전굴 1.2±3.8o (전굴 9∼후 굴 7o)이었으며, 5o 이상의 내외반 각변형을 보인 경우는 1 예, 5o 이상의 전후굴 각변형을 보인 경우는 2예 있었다.
경골 간부 단순 골절의 골수강 내 금속정 삽입술 후 골유 합 기간은 14∼16주18,21)로 보고되고 있고, 경골 간부 분절 골절의 골유합 기간은 4.5∼6.5개월로 보고되고 있으며3,13,25), 이 등15)은 경골 간부 분쇄 골절의 골유합 기간은 평균 6.4개 월이었다고 보고하였다. 저자들의 경골 간부 쐐기형 골절의 골유합 기간은 주골편의 골유합 기간은 15.3주로 경골 간부 단순 골절의 골유합 기간과 유사하였고, 쐐기형 골편의 골유 합 기간은 24.2주로 분절 골절의 골유합 기간과 유사하였다.
저자들의 경우 쐐기형 골편의 직경과 골유합 기간은 통계 적으로 유의한 상관 관계가 있었으며, 이는 경골 간부 분쇄 골절에서 쐐기형 골편의 직경이 클수록 주골편에 비해 쐐기 형 골편이 크고 유합되어야 할 골절면이 크므로 골유합 기간 이 길어졌다고 생각하였다. 저자들은 쐐기형 골편의 길이가 길수록 횡골절 보다는 나선형 골절일 가능성이 높고 골절면 이 경골 횡축과 큰 각을 이루고 큰 수평 전단력을 가지게 되 어 각변형이나 지연유합을 일으키기 쉬울 것으로 생각하였 다. 그러나, 쐐기형 골편의 길이와 골유합 기간과의 상관 관 계는 없었다.
저자들의 경우 골절 정복 후 쐐기형 골편의 전위 정도와 골유합 기간은 통계적으로 유의하게 상관 관계가 있었다. 주 골편의 정복을 위해 비확공성 골수강 내 금속정의 삽입이나 확공성 금속정을 위한 유도 강선의 삽입 시 쐐기형 골편은 더욱 전위되기 쉬우며 이는 폐쇄성 골수강 내 금속정 고정술 시라도 쐐기형 골편과 주골편의 접촉면을 넓히기 위해 mal- leolar clamp나 towel clip 등을 이용하여 일시적으로 고정한 상태에서 금속정을 삽입하는 등의 추가적인 노력이 필요하 다고 생각하였다.
개방성 골절은 외상의 강도가 크고 동반하는 연부 조직의 손상과 골절편으로의 혈액 순환 장애로 비개방성 골절에 비 해 골유합 기간이 길다고 알려져 있으며4), 저자들의 경골 간
부 쐐기형 골절에서도 개방성 골절시 골유합 기간이 길었다.
Schemitsch 등23)과 Ziran 등26)은 확공성과 비확공성 골수 강 내 금속정 삽입술에 따른 골유합이 차이를 보이지 않는다 고 보고하였고, Braten 등2)과 Kessler 등12)은 확공으로 인해 골절 치유 과정이 지연될 수 있음을 보고하였다. 그러나, 비 개방성 경골 간부 골절에서 확공성 골수강 내 금속정 삽입술 은 골 유합률1), 골유합 기간14), 합병증의 발생5)에 있어 비확 공성 골수강 내 금속정 삽입술보다 유리하다는 보고가 많으 며, 골수강 내 확공 직후 골수강 내 혈관은 완전히 파괴되 지만 수 주 간의 재혈관화로 피질골의 혈액 공급이 회복되
고17,22) 충분한 기계적인 안정성을 얻을 수 있는 장점으로22)
심한 분쇄나 분절 골편을 동반한 비개방성 경골 간부 골절에 서 확공성 금속정 고정술이 추천된다.
저자들의 경골 간부 쐐기형 골절의 비교에서 확공성 금속 정 삽입술 시 골유합 기간이 짧았으며, 이는 확공성 골수강 내 금속정 삽입술을 사용한 16예는 모두 비개방성 골절이었 던 영향과 확공으로 인한 골이식 효과, 보다 두꺼운 금속정 의 사용을 통한 working length의 단축과 고정력의 증가가 영향을 미쳤을 것으로 생각하였다.
결 론
경골 간부 쐐기형 골절은 폐쇄성 골수강 내 금속정 고정 술로 만족할 만한 임상적, 방사선학적 결과를 얻을 수 있으 나, 쐐기형 골편은 주골편에 비해 긴 골유합 기간을 보였다.
폐쇄성 골수강 내 금속정을 이용하여 경골 간부 쐐기형 골절 의 치료시 쐐기형 골편의 직경이 클 경우 골편의 전위에 대 한 세심한 주의가 필요하리라 생각된다.
참 고 문 헌
1) Bhandari M, Guyatt GH, Tong D, Adili A and Shau- ghnessy SG: Reamed versus nonreamed intramedullary nail- ing of lower extremity long bone fractures: a systematic overview and meta-analysis. J Orthop Trauma, 14: 2-9, 2000.
2) Braten M, Terjesen T, Svenningsen S and Kibsgaard L:
Effects of medullary reaming on fracture healing. Tibial osteotomies in rabbits. Acta Orthop Scand, 61: 327-329, 1990.
3) Wu CC and Shih CH: Segmental tibial shaft fractures treated with interlocking nailing. J Orthop Trauma, 7: 468- 472, 1993.
4) Court-Brown CM, Christie J and McQueen MM: Closed intrameduallary tibial nailing. Its use in closed and type I open fractures. J Bone Joint Surg, 72-B: 605-611, 1990.
cance of posterior boot edge fracture in Alpine skiing?
Sportverletz Sportschaden, 1: 161-167, 1987.
7) Greitbauer M, Heinz T, Gaebler C, Stoik W and Vecsei V: Unreamed nailing of tibial fractures with the solid tibial nail. Clin Orthop, 350: 105-114, 1998.
8) Gustilo RB and Anderson JT: Prevention of infection in the treatment of one thousand and twenty-five open fractures of the long bones: retrospective and prospective analysis. J Bone Joint Surg, 58-A: 453-458, 1976.
9) Henley MB: Intramedullary devices for tibial fracture stabili- zation. Clin Orthop, 240: 87-96, 1989.
10) Jeong HJ, Kim KC, Choi JY, Koo BS and Oh JH: The angular deformity of interlocking nailing in tibial fractures. J Korean Fracture Soc, 13: 905-911, 2000.
11) Karlstrom G and Olerud S: Fractures of the tibial shaft: a critical evaluation of treatment alternatives. Clin Orthop, 105:
82-115, 1974.
12) Kessler SB, Hallfeldt KKJ, Perren SM and Schweiberer L: The effect of reaming and intramedullary nailing on the fracture healing. Clin Orthop, 212: 18-25, 1986.
13) Kim KS, Song JY, Shon KS and Kim JH: Interlocking nailing in segmental tibial fractures -The Problems of the fractures involving proximal portion-. J Korean Fracture Soc, 13: 912-920, 2000.
14) Larsen LB, Madsen JE, Hoiness PR and Ovre S: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years' follow-up. J Orthop Trauma, 18: 144-149, 2004.
15) Lee KH, Kim HM, Moon CW, Kim YS and Mun WS:
Augmenatation plate fixation of the management of long- bone nonunion after intramedullary nailing. J Korean Frac- ture Soc, 17: 265-270, 2004.
16) Lerner A, Chezar A, Haddad M, Kaufman H, Rozen N and Stein H: Complications encountered while using thin-
2005.
17) Nakamura T, Itoman M and Yokoyama K: Cortical reva- scularization after reamed and unreamed intramedullary nail- ing in the rabbit femur: a microangiographic histometric analysis. J Trauma, 47: 744-751, 1999.
18) Pankovich AM, Tarabishy IE and Yelda S: Flexible intra- medullary nailing of tibial-shaft fractures. Clin Orthop, 160:
185-195, 1981.
19) Pantazopoulos T, Galanos P, Agoropoulos Z and Harto- filakidis-Garofalidi: Treatment of double tibial fractures by blind intramedullary nailing. Clin Orthop, 84: 137-143, 1972.
20) Park IH, Lee KB, Lee JY, Song KW and Lee SY: Treat- ment using unreamed intramedullary nailing for open tibial fractures. J Korean Fracture Soc, 10: 886-891, 1997.
21) Sarmiento A: Functional below-the-knee brace for tibial fractures. A report on its use in one hundred thirty-five cases. J Bone Joint Surg, 52-A: 295-311, 1970.
22) Schemitsch EH, Kowalski MJ, Swiontkowski MF and Senft D: Cortical bone blood flow in reamed and undreamed closed intramedullary nailing: a fractured tibia model in sheep. J Orthop Trauma, 8: 373-382, 1994.
23) Schemitsch EH, Turchin DC, Kowalski MJ and Swiont- kowski MF: Quantitative assessment of bone injury and repair after reamed and undreamed locked intramedullary nailing. J Trauma, 45: 250-255, 1998.
24) Schmidt AH, Finkemeier CG and Tornetta P III: Treat- ment of closed tibial fractures. J Bone Joint Surg, 85-A:
352-368, 2003
25) Song KJ, Hwang BY, Kim JR and Lee YG: Interlocking intramedullary nailing for the treatment of segmental tibial shaft fractures. J Korean Fracture Soc, 12: 69-75, 1999.
26) Ziran BH, Darowish M, Klatt BA, Agudelo JF and Smith WR: Intramedullary nailing in open tibia fractures: a com- parison of two techniques. Int Orthop, 28: 235-238, 2004.