Comparison of Dietary Habit and Food Consumption
among Elementary School Students with or without Rhinitis and Sinusitis
Ji-Hyun Kwon1 and Jihyeung Ju2+
1Graduate School of Education, Chungbuk National University
2Department of Food and Nutrition, Chungbuk National University
Abstract
Rhinitis and sinusitis are among the most common medical conditions in Korea, as well as Western societies. Environmental factors may influence both rhinitis and sinusitis; however, the role of dietary factors in rhinitis and sinusitis is not clear. The present study aims to compare the dietary habit, food consumption frequency, and food preference of elementary school students with or without rhinitis and sinusitis. The demand of their parents for an education program for the dietary prevention against rhinitis and sinusitis was also examined.
The survey was conducted with a total of 200 subjects recruited from two elementary schools located in Gyeonggi area of Korea. The subjects consisted of 101 students with rhinitis and/or sinusitis (RS group) and 99 without rhinitis and sinusitis (control group). The students of the RS group were more likely to have habits of eating-out and street food use, to consume bean, peanut, walnut, almond, yogurt, egg, snack, and French fries frequently, and to prefer the types of foods prepared by stir-frying and deep-frying than the control group. The parents who recognized 'school nutrition teachers or food/nutrition-majored specialists' as the most appropriate educator for the dietary education program in the RS group (48.5% of their parents) were less than those in the control group (67.7% of their parents). The present study suggest that students with rhinitis and/or sinusitis may be different from those without the disease(s) in their dietary habit, frequently consumed foods, and preferred type of foods. More epidemiological, intervention, and laboratory studies are needed in order to elucidate the role of dietary factors in the development and prevention of rhinitis and sinusitis, which will have a significant implication to public health.
Key words : dietary habit, food consumption, rhinitis, sinusitis, elementary school student
I. Introduction
1)Rhinitis is an inflammation occurring in the mucous membrane of the nose and usually accompanied with several characteristic symptoms such as rhinorrhea, nasal congestion, itching, and sneezing (Tan RA and Corren J 2011, Dykewicz MS and Hamilos DL 2010). Rhinitis can be allergic or non-allergic, but the most common condition is likely allergic and non-allergic rhinitis in combination (Dykewicz MS and
†Corresponding author : Jihyeung Ju, Department of Food and Nutrition, Chungbuk National University, Cheongju, 361-763, Korea Tel: +82-43-261-2681
Fax: +82-43-267-2742 E-mail: [email protected]
Hamilos DL 2010, Wallace DV et al. 2008, Settipane RA and Charnock DR 2007). Sinusitis is an inflammation occurring in the sinus, a cavity in the substance of a bone of the skull (Tan RA and Corren J 2011, Dykewicz MS and Hamilos DL 2010). Characteristic symptoms of sinusitis involve nasal obstruction, headache, and post nasal drip. Sinusitis rarely occurs in the absence of rhinitis because rhinitis frequently extends into sinusitis, for instance by exacerbating acute allergic rhinitis to chronic sinusitis (Tan RA and Corren J 2011, Dykewicz MS and Hamilos DL 2010). The co-existing status of both rhinitis and sinusitis is often termed as rhinosinusitis, and sinusitis and rhinosinusitis are occasionally regarded as synonymous terms (Tan RA and Corren J 2011, Dykewicz MS and Hamilos DL 2010, Van Crombruggen K et al. 2011, Meltzer EO et al. 2004). Rhinitis and sinusitis are among the most common medical conditions in Korea as http://dx.doi.org/10.9724/kfcs.2012.28.6.847
well as Western societies (Dykewicz MS and Hamilos DL 2010, Ministry of Health & Welfare 2010, National Health Insurance Corporation 2011). The prevalence of rhinitis is estimated to 26% in Korea (Ministry of Health & Welfare 2010) and 10 to 25% in Western societies (Dykewicz MS and Hamilos DL 2010). Chronic sinusitis is one of the highly frequent diseases submitted to surgery in Korea (National Health Insurance Corporation 2011) and affects an estimated 31 million people annually in US (Dykewicz MS and Hamilos DL 2010). Chronic rhinosinusitis also affects 6 to 7% of the population in Korea (Ministry of Health & Welfare 2010, Kim YS et al. 2011) and 13 % of the population in US (Hamilos DL 2011). Both rhinitis and sinusitis can decrease quality of life, aggravate comorbid conditions, and account for substantial health care expenditures. It is, therefore, important to understand the etiology of the diseases and develop effective and safe strategies for the prevention against rhinitis and sinusitis.
Inflammatory and allergic types of diseases are regarded as a multi-factorial disease, and environmental factors, including diet, are considered to play an important role in the etiology (Novak N and Leung DY 2005, Tricon S et al. 2006, Galland L 2010, Calder PC et al. 2009). The association between allergic types of rhinitis and dietary factors has been reported in a few studies. In a study with children, the frequent consumption of nuts and butter were associated with an increased risk of allergic rhinitis (Farchi S et al. 2003). In another study with children, Mediterranenan diet, characterized by a high consumption of cereals as well as a low consumption of junk food and fat, was associated with a decreased risk of allergic rhinitis (De Batlle J et al. 2008). In the study with adolescents, the frequent consumption of animal liver and fruits were associated with an increased risk of allergic rhinitis (Huang SL et al. 2001). In the study with adults, high intakes of alpha-linolenic, eicosapentaenoic, and docosahexaenoic acids were associated with a decreased risk of allergic rhinitis (Hoff S et al. 2005, Miyake Y et al. 2007).
There has been an inconsistency in the association of milk consumption and allergic rhinitis; one study showed an inverse association (Farchi S et al. 2003), but the other showed a positive association (Huang SL et al. 2001).
Importantly, there have been no reports on dietary factors associated with sinusitis as well as rhinitis including both allergic and non-allergic types. Since dietary modification in early life was suggested to be effective in preventing and alleviating allergic diseases (Devereux G and Seaton A 2005), it is crucial to determine dietary factors associated with rhinitis and sinusitis in populations at the early stage of life.
The present study was designed to investigate dietary habits and food consumption in elementary school students with either rhinitis or sinusitis, or both, in comparison to those without rhinitis and sinusitis. The results from this study will help design a large scale of epidemiological studies
that are aimed to identify dietary pattern, single food factors, and nutrients that critically contribute to the development or prevention of rhinitis and sinusitis. In the present study, the demand of the parents for a dietary education program was also investigated, which is expected to provide motivation as well as basic information for initiating the development of an effective education program on the dietary prevention against rhinitis and sinusitis.
Ⅱ. Methods
Subjects and study period
This study followed principles in the Declaration of Helsinki. Subjects were recruited among the students in two elementary schools located in Gyeonggi area of Korea. In order to select the subjects, two questions were used; the one was whether or not they had ever been diagnosed for rhinitis and/or sinusitis medically; the other was whether or not they had one or more symptoms of the diseases at the time of survey performed. Those students that gave positive answers for both questions were classified into the group of subjects with rhinitis and/or sinusitis (RS group), whereas those students that gave negative answers for both questions were classified into the control group. Since the present study aimed to compare the dietary habit and food preference between the subjects with or without rhinitis and/or sinusitis, the subjects were intentionally balanced by genders and school grades within and between groups. The survey was conducted on September 2010 using the questionnaire developed for this study as described in the following section. The response rate to the survey was 88.9
% (240 out of 270 students). Out of 240 questionnaires, 40 questionnaires were excluded due to their incompleteness, and the rest 200 questionnaires (101 questionnaires from the RS group and 99 questionnaires from the control group) were used for final analyses.
Questionnaire development
The questionnaire for this study was developed to investigate dietary habit, food consumption, and food preference of elementary school students with rhinitis and/or sinusitis in comparison to the students without rhinitis and sinusitis. The demand of their parents for an education program on dietary prevention against rhinitis and sinusitis was also examined. A pilot study was conducted prior to the main survey to verify the suitability of the questionnaire, and then it was revised according to the results. The final questionnaire consisted of general characteristics, disease-related characteristics, dietary habits, and food
consumption frequency, and food preference of students as well as demands of their parents on dietary education program. General characteristics were assessed with 9 different questions on gender, school year, exercise frequency, presence of pets and plants home, lactation methods and period, baby food type, and family member with the diseases. Disease-related characteristics (Dykewicz MS and Hamilos DL 2010, Kim YS et al. 2011) were assessed with 5 different questions on rhinitis and/or sinusitis diagnosed and carried, onset age, seasonal prevalence involvement, self-reporting severity level, and manifestation of other types of allergy. Dietary habits (Kweon N and Koh B 2005, Lee B 2004) were assessed with 6 different questions on meal frequency, breakfast-skipping frequency, eating-out frequency, street-food consumption frequency, late-night meal frequency, and levels of balanced diet. Food consumption frequency was assessed with questions on 33 different food items that had been known for the most probable allergy-induced foods (Waserman S and Watson W 2011, Cingi C et al. 2010). The frequency was recorded as 'never', 'once a month', 'twice to three times a week', 'once a week', 'twice to three times a week', 'four to six times a week', or 'once to three times a day'. Food preference was assessed with questions on the levels of preference (five levels from 'very low' to 'very high') for foods in 7 different preparation types and 7 different food groups. Demands of the parents for a dietary education program were assessed with 4 different questions on the intention level of attendance as well as preferred place, educator, and types for the program. All of the questionnaires on the students were instructed to complete by themselves with the help of their parents for accuracy of the data.
Statistical analyses
Data were analyzed using SPSS software (version 12.0).
Frequency for the general characteristics, disease-related characteristics, dietary habits, and the demand for the dietary education program was calculated in percentages. The difference in the frequency between the RS and control groups was determined by chi square test. The food consumption frequency and preference data were converted semi-quantitatively to the scores ranging from 0 to 3 and 1 to 5, respectively. Mean and standard deviation were then calculated, and the difference in the mean between the RS and control groups was determined by two-tailed student t-test. The p< 0.05 was considered significant.
Ⅲ. Results
General characteristics of the subjects
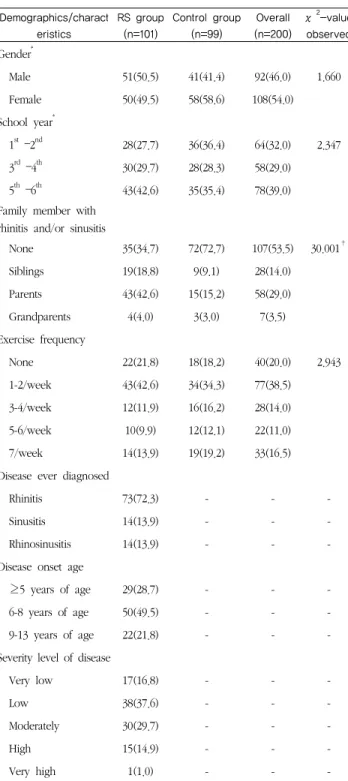
The general characteristics of the students who participated in this study are shown in Table 1. As indicated in the Methods, genders and school grades of the subjects were intentionally balanced based on the study aim when those subjects were recruited. Among the 200 students, 46.0% were male, and 54.0% were female. The ratio of male to female in the RS group was similar to that in the control group.
School years (the 1st to 2nd year, the 3rd to 4th year, and the 5th to 6th year) of the students were evenly distributed within a group as well as between the RS and control groups.
The family history of the students in the RS was statistically different from that in the control group (P <
0.001). In the RS group, the students having a family member with rhinitis and/or sinusitis (65.3%) were more than those not having such family members (34.7%). In the control group, however, showed the opposite results; the students with a family member with rhinitis and/or sinusitis (27.3%) were much less than those without such family members (73.7%). Among the family member with rhinitis and/or sinusitis, the parents made up the majority. The other characteristics, such as exercise frequency, percentages of the students in the presence or absence of pets and plants at home, lactation method, lactation period, and baby food types, in the RS group were not statistically different from those in the control groups.
Disease-related characteristics
Disease-related characteristics of the RS group are shown in Table 1. Among a total of 101 students in the RS group, the students with only rhinitis were the majority, accounting for 72.3%. Approximately half of the students in the RS group (49.5%) began to have the disease at their age of 6-8 years. Approximately half of the students in the RS group (58.4%) were involved with seasonal prevalence of the disease. Most of the students in the RS group (84%) had experienced very low to moderate level of severity of the disease while only 16% of the students had experienced high to very high level of severity. The number of students having manifestation of other types of allergic symptoms (45.6%) was similar to those not having such manifestation (55.4%).
Among the students with other allergic symptoms, the students with atopic dermatitis were the majority, accounting for 30.7% of the students in the RS group.
Demographics/charact eristics
RS group (n=101)
Control group (n=99)
Overall (n=200)
χ2-value observed Gender*
Male 51(50.5) 41(41.4) 92(46.0) 1.660
Female 50(49.5) 58(58.6) 108(54.0)
School year*
1st –2nd 28(27.7) 36(36.4) 64(32.0) 2.347 3rd –4th 30(29.7) 28(28.3) 58(29.0) 5th –6th 43(42.6) 35(35.4) 78(39.0) Family member with
rhinitis and/or sinusitis
None 35(34.7) 72(72.7) 107(53.5) 30.001†
Siblings 19(18.8) 9(9.1) 28(14.0)
Parents 43(42.6) 15(15.2) 58(29.0)
Grandparents 4(4.0) 3(3.0) 7(3.5)
Exercise frequency
None 22(21.8) 18(18.2) 40(20.0) 2.943
1-2/week 43(42.6) 34(34.3) 77(38.5)
3-4/week 12(11.9) 16(16.2) 28(14.0)
5-6/week 10(9.9) 12(12.1) 22(11.0)
7/week 14(13.9) 19(19.2) 33(16.5)
Disease ever diagnosed
Rhinitis 73(72.3) - - -
Sinusitis 14(13.9) - - -
Rhinosinusitis 14(13.9) - - -
Disease onset age
≥5 years of age 29(28.7) - - -
6-8 years of age 50(49.5) - - -
9-13 years of age 22(21.8) - - -
Severity level of disease
Very low 17(16.8) - - -
Low 38(37.6) - - -
Moderately 30(29.7) - - -
High 15(14.9) - - -
Very high 1(1.0) - - -
*Factors balanced intentionally when the subjects were recruited
†P < 0.001 by χ2-test
Table 1. General demographics and characteristics of the elementary school students with or without rhinitis
and sinusitis N(%)
Dietary habits
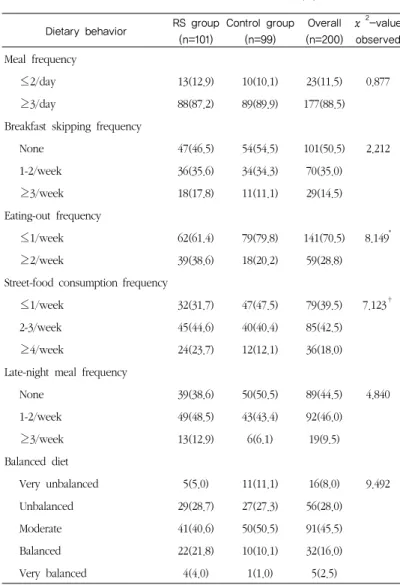
Six different dietary habits were investigated, and the results are shown in Table 2. Both eating-out and street-food
consumption frequencies of the RS group were significantly different from the corresponding frequencies of the control group (P < 0.01). The proportion of students whose eating-out frequency was ≥2/week in the RS group (38.6%) was greater than that in the control group (20.2%), resulting in significantly difference between these two groups (P <
0.01). The proportion of students whose street-food consumption frequency was ≥4/week in the RS group (23.7%) was greater than that in the control group (12.1%), resulting in statistical difference between these two groups (P
< 0.05). The other 4 dietary habits were comparable between those two groups.
Food consumption frequency
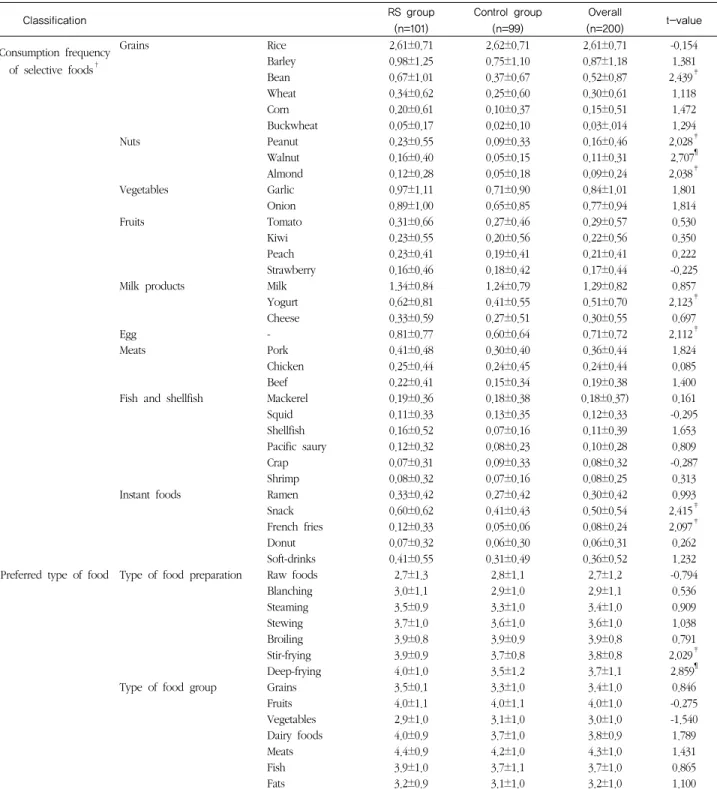
The consumption frequencies for a total of 33 food items in 9 different categories were investigated, and the results are shown in Tables 3. The highest overall consumption frequency was scored for rice (2.61±0.71). The score 2.61 reflects that rice is consumed approximately 2.61 times per day. Frequencies of barley, garlic, onion, milk and egg consumption were also high, ranging the mean score, 0.71-1.29. The lowest consumption frequency was found for buckwheat (0.05±0.17). A significant difference of the consumption frequency between the RS and control groups was found for bean (P < 0.05), peanut (P < 0.05), walnut (P < 0.01), almond (P < 0.05), yogurt (P < 0.05), egg (P <
0.05), snack (P < 0.05), and French fries (P < 0.05); the RS group showed greater frequencies than the control group.
Food preference
The preference of students for the foods in different types of preparation or groups was investigated, and the results are shown in Tables 3. Among 7 different types of food preparation, steaming, stewing, broiling, stir-frying, and deep-frying types were scored to 3-4 out of 5 points, indicating a moderate to high level of preference. The preference to both raw and blanching types of preparation was scored below 3 points, indicating a relatively low level of preference. There was a significant difference in the preference of the RS and control group for both stir-frying (P
< 0.05) and deep frying (P < 0.01) types of food preparation;
the RS groups showed higher levels of preference than the control group.
Among 7 different food groups, the overall preference for both fruit and meat groups was scored above 4 points, indicating a relatively high level of preference. The preference for vegetables, however, was scored below 3 points, indicating a relatively low level of preference. There was no significant difference in the preference for the 7 different subgroups of food between the RS and control groups.
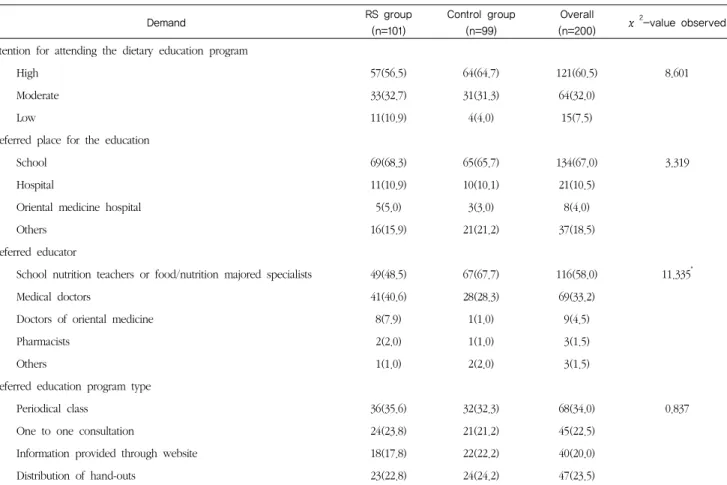
Demands of the parents for dietary education program Demands of parents of the subjects for the dietary education program were investigated, and the results are shown in Table 4. Approximately, 57% of the parents of the RS group reported a high level of intention for attending a dietary education program, and there was no statistical difference in the level of intention between the RS and control groups. The most preferred place and type for the education were 'schools' (67.0%) and 'periodical class' (34.0%), respectively, without a statistical difference between the RS and control groups. The most appropriate educators were recognized as 'school nutrition teachers or food/nutrition-majored specialists' (58.0%). There was a statistical difference between the RS and control groups in the recognition (P < 0.05). In the RS group, the number of parents recognizing 'school nutrition teachers or food/nutrition majored specialists' as the most appropriate educator (48.5%) was similar to those recognizing 'medical doctors' (40.6%). In the control group, the parents recognizing 'school nutrition teachers or food/nutrition majored specialists' as the most appropriate educator (67.7%), however, were much more than those recognizing 'medical doctors' (28.3%).
Ⅳ. Discussion and Conclusion
Diet may influence both inflammatory and allergic diseases in general, but the role of diet particularly in rhinitis and sinusitis is not clearly understood although a few studies have been reported on the association between dietary factors and allergic type of rhinitis (De Batlle J et al. 2008, Farchi S et al. 2003, Huang SL et al. 2001, Hoff S et al. 2005, Miyake Y et al. 2007). The mixed condition of allergic and non-allergic types is most common in rhinitis (Dykewicz MS and Hamilos DL 2010,Wallace DV et al. 2008, Settipane RA and Charnock DR 2007), and sinusitis frequently occurs with rhinitis (Tan RA and Corren J 2011, Dykewicz MS and Hamilos DL 2010, Van Crombruggen K et al. 2011, Meltzer EO et al. 2004).
Therefore, we intended in the present study to allocate the subjects with either rhinitis or sinusitis, or both, together in the RS group and then examined dietary habits, food consumption, and food preference of the subjects in comparison to those without rhinitis and sinusitis. The subjects of this study were a total of 200 students (101 students in the RS group and 99 students in the control group) aged approximately 6 to 12 years (the first to sixth school year) from two elementary schools located in Gyeonggi area of Korea.
In the present study, we investigated whether or not dietary habits of the students in the RS group differ to those
in the control group. Our results indicated the frequent eating-out and street-food use of the students in the RS group (Table 2). The reason for such findings is not clear.
Since dust often mediates the development of allergic rhinitis (Pala G et al. 2010, Kim JH et al. 2010, Hernandez M et al.
1999), this finding might be partially attributed to the presence of dust in the environment or in the foods consumed outdoors. Further studies are needed to determine precise factors that confer those habits to be frequently found in the subjects with rhinitis and/or sinusitis.
Dietary behavior RS group (n=101)
Control group (n=99)
Overall (n=200)
χ2-value observed Meal frequency
≤2/day 13(12.9) 10(10.1) 23(11.5) 0.877
≥3/day 88(87.2) 89(89.9) 177(88.5)
Breakfast skipping frequency
None 47(46.5) 54(54.5) 101(50.5) 2.212
1-2/week 36(35.6) 34(34.3) 70(35.0)
≥3/week 18(17.8) 11(11.1) 29(14.5)
Eating-out frequency
≤1/week 62(61.4) 79(79.8) 141(70.5) 8.149*
≥2/week 39(38.6) 18(20.2) 59(28.8)
Street-food consumption frequency
≤1/week 32(31.7) 47(47.5) 79(39.5) 7.123†
2-3/week 45(44.6) 40(40.4) 85(42.5)
≥4/week 24(23.7) 12(12.1) 36(18.0)
Late-night meal frequency
None 39(38.6) 50(50.5) 89(44.5) 4.840
1-2/week 49(48.5) 43(43.4) 92(46.0)
≥3/week 13(12.9) 6(6.1) 19(9.5)
Balanced diet
Very unbalanced 5(5.0) 11(11.1) 16(8.0) 9.492
Unbalanced 29(28.7) 27(27.3) 56(28.0)
Moderate 41(40.6) 50(50.5) 91(45.5)
Balanced 22(21.8) 10(10.1) 32(16.0)
Very balanced 4(4.0) 1(1.0) 5(2.5)
*P < 0.01 by χ2-test
†P < 0.05 by χ2-test
Table 2. Dietary habit of the elementary school students with or without rhinitis and sinusitis N(%)
We selected 33 food items that have been known to induce allergic responses (Waserman S and Watson W 2011, Cingi C et al. 2010) and then examine whether or not the consumption frequency of the RS group is different to that of the control group. Our results indicated that the student of
Classification RS group (n=101)
Control group (n=99)
Overall
(n=200) t-value Consumption frequency
of selective foods†
Grains Rice 2.61±0.71 2.62±0.71 2.61±0.71 -0.154
Barley 0.98±1.25 0.75±1.10 0.87±1.18 1.381
Bean 0.67±1.01 0.37±0.67 0.52±0.87 2.439‡
Wheat 0.34±0.62 0.25±0.60 0.30±0.61 1.118
Corn 0.20±0.61 0.10±0.37 0.15±0.51 1.472
Buckwheat 0.05±0.17 0.02±0.10 0.03±.014 1.294
Nuts Peanut 0.23±0.55 0.09±0.33 0.16±0.46 2.028‡
Walnut 0.16±0.40 0.05±0.15 0.11±0.31 2.707¶
Almond 0.12±0.28 0.05±0.18 0.09±0.24 2.038‡
Vegetables Garlic 0.97±1.11 0.71±0.90 0.84±1.01 1.801
Onion 0.89±1.00 0.65±0.85 0.77±0.94 1.814
Fruits Tomato 0.31±0.66 0.27±0.46 0.29±0.57 0.530
Kiwi 0.23±0.55 0.20±0.56 0.22±0.56 0.350
Peach 0.23±0.41 0.19±0.41 0.21±0.41 0.222
Strawberry 0.16±0.46 0.18±0.42 0.17±0.44 -0.225
Milk products Milk 1.34±0.84 1.24±0.79 1.29±0.82 0.857
Yogurt 0.62±0.81 0.41±0.55 0.51±0.70 2.123‡
Cheese 0.33±0.59 0.27±0.51 0.30±0.55 0.697
Egg - 0.81±0.77 0.60±0.64 0.71±0.72 2.112‡
Meats Pork 0.41±0.48 0.30±0.40 0.36±0.44 1.824
Chicken 0.25±0.44 0.24±0.45 0.24±0.44 0.085
Beef 0.22±0.41 0.15±0.34 0.19±0.38 1.400
Fish and shellfish Mackerel 0.19±0.36 0.18±0.38 0.18±0.37) 0.161
Squid 0.11±0.33 0.13±0.35 0.12±0.33 -0.295
Shellfish 0.16±0.52 0.07±0.16 0.11±0.39 1.653
Pacific saury 0.12±0.32 0.08±0.23 0.10±0.28 0.809
Crap 0.07±0.31 0.09±0.33 0.08±0.32 -0.287
Shrimp 0.08±0.32 0.07±0.16 0.08±0.25 0.313
Instant foods Ramen 0.33±0.42 0.27±0.42 0.30±0.42 0.993
Snack 0.60±0.62 0.41±0.43 0.50±0.54 2.415‡
French fries 0.12±0.33 0.05±0.06 0.08±0.24 2.097‡
Donut 0.07±0.32 0.06±0.30 0.06±0.31 0.262
Soft-drinks 0.41±0.55 0.31±0.49 0.36±0.52 1.232
Preferred type of food Type of food preparation Raw foods 2.7±1.3 2.8±1.1 2.7±1.2 -0.794
Blanching 3.0±1.1 2.9±1.0 2.9±1.1 0.536
Steaming 3.5±0.9 3.3±1.0 3.4±1.0 0.909
Stewing 3.7±1.0 3.6±1.0 3.6±1.0 1.038
Broiling 3.9±0.8 3.9±0.9 3.9±0.8 0.791
Stir-frying 3.9±0.9 3.7±0.8 3.8±0.8 2.029‡
Deep-frying 4.0±1.0 3.5±1.2 3.7±1.1 2.859¶
Type of food group Grains 3.5±0.1 3.3±1.0 3.4±1.0 0.846
Fruits 4.0±1.1 4.0±1.1 4.0±1.0 -0.275
Vegetables 2.9±1.0 3.1±1.0 3.0±1.0 -1.540
Dairy foods 4.0±0.9 3.7±1.0 3.8±0.9 1.789
Meats 4.4±0.9 4.2±1.0 4.3±1.0 1.431
Fish 3.9±1.0 3.7±1.1 3.7±1.0 0.865
Fats 3.2±0.9 3.1±1.0 3.2±1.0 1.100
*Food consumption frequency was scored as 1-3 points for 1-3/day, 0.71 points for 4-6/week, 0.36 points for 2-3/week, 0.14 points for 1/week, 0.08 points for 2-3/week, 0.03 points for 1/month, and 0 points for none. Food preference was scored as 1-5 points for very low to very high preference.
†Foods that have been suggested to induce allergy
‡P < 0.05 by two-tailed student t-test
¶P < 0.01 by two-tailed student t-test
Table 3. Food consumption frequency and preference of the elementary school students with or without rhinitis and sinusitis*
Mean ± SD
RS group frequently consumed bean, peanut, walnut, almond, yogurt, egg, snack, and French fries compared to those of the control group (Table 3). The results on the frequent consumption of beans in the RS group are similar to the previous report on the high intake of soybeans and isoflavones associated with a reduced prevalence of allergic rhinitis in Japanese women (Miyake Y et al. 2005). The results on the frequent consumption of nuts in the RS group were also similar to the previous report on high intake of nuts associated with an increased risk of allergic rhinitis in children (Farchi S et al. 2003). The frequent yogurt consumption of the RS group, however, appears inconsistent to the previous report that suggested beneficial activities of probiotics against allergic diseases (Ozdemir O 2010, Boyle RJ and Tang ML 2006, Kalliomaki M et al. 2010, Yao TC et al.
2010), including allergic rhinitis (Vliagoftis H et al. 2008). The frequent consumption of yogurt in the RS group found in our study might be speculated as a result of the disease, rather than a cause. There is little known on the association of egg consumption with rhinitis and sinusitis although ingested food allergen may induce allergic rhinitis (Waserman S and Watson W 2011, Cingi C et al. 2010). Considering that allergic responses to cooked eggs was reported to resolve quickly compared to those to uncooked eggs (Clark A et al.
2011), it may be desirable to guide children with allergic rhinitis to consume well-cooked eggs rather than less or uncooked eggs. The frequent snack consumption of the RS group was found in our study. Influences of snack consumption on rhinitis and sinusitis are not known.
However, frequent snack consumption habit of people with was reported (Yang SH et al. 2009). Food additives and preservatives might be suspected for the reason behind this finding although they are known to rarely induce allergic responses (Waserman S and Watson W 2011). Previously, the frequent consumption of candies was reported to be positively associated with allergic rhinitis (Tamay Z et al.
2007). Relevance of food additives and preservatives present in foods such as snacks and candies with rhinitis and sinusitis remains to be clarified.
In the present study, we also examined food preference of the students in the RS group compared to those in the control group. Our results indicated that the preference of the RS group to both stir-frying and deep frying types of food preparation was prominent (Table 3). The frequent consumption of deep fried foods was reported to be associated with asthma, but not allergic rhinitis (Huang SL et al. 2001). Previously, a positive association between the frequent use of butter in sauces and allergic rhinitis was reported, but there was no association with the use of fats in cooking, such as olive oil, seed oil, butter, and margarine was reported (Farchi S et al. 2003). The present and
previous results suggest that more studies on the effects of dietary fats on rhinitis and sinusitis are needed. The preference for vegetables was scored below 3 points, indicating a relatively low level of preference. Similarly, the low preference of Korean elementary school students for vegetables was reported in previous studies (Kweon N and Koh B 2005, Kim Y and Seo J 2004, Lee B 2004). In our study, the preference for vegetables of the students in the RS group was not different to that in the control group. This finding was consistent to some of the previous reports showing no association between vegetable consumption and allergic rhinitis (Huang SL et al. 2001, Farchi S et al. 2003), but inconsistent to the other showing an inverse association between vegetable consumption and allergic rhinitis (Tamay Z et al. 2007). Despite of such inconsistency, vegetables and antioxidants have been shown to exert beneficial effects against inflammatory and allergic diseases in general. In this respect, children with rhinitis and sinusitis may be still guided to consume vegetables sufficiently. To enhance the consumption of vegetables in elementary school students, highly preferred recipes and menus using vegetables should develop and urge to be applied in school meal services (Ahn Y and Ro H 2009). Relevant culinary education programs will be useful for the parents who have elementary school students.
Our results revealed that the students of the RS group are more likely to have family members with rhinitis and/or sinusitis than those of the control group (Table 1).
Previously, a family history of atopic dermatitis is reported to be a risk factor of allergic rhinitis (Tamay Z et al. 2007).
There is a paucity of data, however, on family history of rhinitis and sinusitis affecting to rhinitis and sinusitis at the next generation. Interaction of genetic and environmental factors might contribute to the development of rhinitis and sinusitis, which offers another line of research.
Our results indicated that most of the parents had moderate to high level of intention in attending dietary education programs for the prevention of rhinitis and sinusitis without statistical difference in the level of intention between the RS and control groups (Table 4). In the present study, the parents of elementary school students were likely to prefer periodical classes offered in schools. To our knowledge, this is the first study that examined the demand of parents of elementary school students with or without rhinitis and sinusitis for attending dietary education programs for the prevention of rhinitis and sinusitis. More detailed studies will be needed in order to develop an effective dietary education program for the prevention against rhinitis and sinusitis.
The limitations of the present study should be considered when interpreting these results. Most of the subject in the RS group had rhinitis and/or sinusitis only at or below moderate level (Table 1), which is a limitation of the present study
Demand RS group (n=101)
Control group (n=99)
Overall
(n=200) χ2-value observed Intention for attending the dietary education program
High 57(56.5) 64(64.7) 121(60.5) 8.601
Moderate 33(32.7) 31(31.3) 64(32.0)
Low 11(10.9) 4(4.0) 15(7.5)
Preferred place for the education
School 69(68.3) 65(65.7) 134(67.0) 3.319
Hospital 11(10.9) 10(10.1) 21(10.5)
Oriental medicine hospital 5(5.0) 3(3.0) 8(4.0)
Others 16(15.9) 21(21.2) 37(18.5)
Preferred educator
School nutrition teachers or food/nutrition majored specialists 49(48.5) 67(67.7) 116(58.0) 11.335*
Medical doctors 41(40.6) 28(28.3) 69(33.2)
Doctors of oriental medicine 8(7.9) 1(1.0) 9(4.5)
Pharmacists 2(2.0) 1(1.0) 3(1.5)
Others 1(1.0) 2(2.0) 3(1.5)
Preferred education program type
Periodical class 36(35.6) 32(32.3) 68(34.0) 0.837
One to one consultation 24(23.8) 21(21.2) 45(22.5)
Information provided through website 18(17.8) 22(22.2) 40(20.0)
Distribution of hand-outs 23(22.8) 24(24.2) 47(23.5)
*P < 0.05 by χ2-test
Table 4. Parental demand for the dietary education program N(%)
since this might have prevented from finding clear differences between the RS and control groups. Also the disease severity was self-reported, and therefore the classification was not very clear. The heterogeneity of the subjects is another limitation, which might have resulted in the lack of specificity for identifying dietary factors important in particular subgroups. The number of subjects in this study was not large enough to reflect dietary habits and food consumption of elementary school students in Korea and to classify the RS group into different subgroups, which is also a limitation. A large scale of epidemiological studies need to be conducted, in which subjects may be classified into different subgroups by the severity of diseases or by such factors as the presence of rhinitis, sinusitis, or rhinosinusitis, allergic or non-allergic types, and chronic or acute types.
In summary, we found in the present study that the elementary school students with rhinitis and/or sinusitis were more likely to have eating-out habits, to frequently consume some of the allergy-induced foods, and prefer foods prepared by frying types. To our knowledge, this is the first study to compare dietary habits, food consumption, and food
preference of the elementary school students with or without rhinitis and sinusitis. The results are expected to provide basic information for further identifying protective and risk factors in diet for rhinitis and sinusitis, which will have a significant implication in public health.
Acknowledgement
This work was supported by the National Research Foundation of Korea grant funded by the Korea government (No. 2010-0025311). This work was the part of master's thesis of Ji-Hyun Kwon.
References
Ahn Y, Ro H. 2009. A survey on preferences for vegetable cooking methods and vegetable-aversion-related factors among elementary
school students in Kwangju and Chonman Regions. Korean J Comm Nutr 14(5):531-544
Boyle RJ, Tang ML. 2006. The role of probiotics in the management of allergic disease. Clin Exp Allergy 36(5):568-576
Calder PC, Albers R, Antoine JM, Blum S, Bourdet-Sicard R, Ferns GA, Folkerts G, Friedmann PS, Frost GS, Guarner F, Lovik M, Macfarlane S, Meyer PD, M'rabet L, Serafini M, Van Eden W, Van Loo J, Vas Dias W, Vidry S, Winklhofer-Roob BM, ZHAO J. 2009. Inflammatory disease processes and interactions with nutrition. Brit J Nutr 101(Suppl 1):S1-45
Cingi C, Demirbas D, Songu M. 2010. Allergic rhinitis caused by food allergies. Eur Arch Oto-Rhino-L 267(9):1327-1335
Clark A, Islam S, King Y, Deighton J, Szun S, Anagnostou K, Ewan P. 2011. A longitudinal study of resolution of allergy to well-cooked and uncooked egg. Clin Exp Allergy 41(5):706-712 National Health Insurance Corporation, N. H. I. 2011. The Major
Operation Statistics 2010
De Batlle J, Garcia-Aymerich J, Barraza-Villarreal A, Anto JM, Romieu I. 2008. Mediterranean diet is associated with reduced asthma and rhinitis in Mexican children. Allergy 63(10):1310-1316 Devereux G, Seaton A. 2005. Diet as a risk factor for atopy and
asthma. J Allergy Clin Immunol 115(6):1109-1117
Dykewicz MS, Hamilos DL. 2010. Rhinitis and sinusitis. J Allergy Clin Immunol 125(suppl 2):S103-115
Farchi S, Forastiere F, Agabiti N, Corbo G, Pistelli R, Fortes C, Dell'orco V, Perucci CA. 2003. Dietary factors associated with wheezing and allergic rhinitis in children. Eur Respir J 22(5):772-780
Galland L. 2010. Diet and inflammation. Nutr Clin Pract 25(6):634-640
Hamilos DL. 2011. Chronic rhinosinusitis: epidemiology and medical management. J Allergy Clin Immunol 128(4):693-707
Hernandez M, Sanchez-Hernandez MC, Moreno V, Guardia P, Delgado J, Maranon F, Fernandez-Caldas E, Conde J. 1999.
Occupational rhinitis caused by beech wood dust. Allergy 54(4):
405-406
Hoff S, Seiler H, Heinrich J, Kompauer I, Nieters A, Becker N, Nagel G, Gedrich K, Karg G, Wolfram G, Linseisen J. 2005. Allergic sensitisation and allergic rhinitis are associated with n-3 polyunsaturated fatty acids in the diet and in red blood cell membranes. Eur J Clin Nutr 59(9):1071-1080
Huang SL, Lin KC, Pan WH. 2001. Dietary factors associated with physician-diagnosed asthma and allergic rhinitis in teenagers:
analyses of the first Nutrition and Health Survey in Taiwan. Clin Exp Allergy 31(2):259-264
Kalliomaki M, Antoine JM, Herz U, Rijkers GT, Wells JM, Mercenier A. 2010. Guidance for substantiating the evidence for beneficial effects of probiotics: prevention and management of allergic diseases by probiotics. J Nutr 140(3):713S-721S
Kim JH, Kim JE, Choi GS, Hwang EK, An S, Ye YM, Park HS.
2010. A case of occupational rhinitis caused by rice powder in the grain industry. Allergy Asthma Immunol Res 2(2):141-143.
Kim Y, Seo J. 2004. Dietary pattern of children with an unbalanced diet in school feeding. J Korean Diet Assoc 10(3):345-355 Kim YS, Kim NH, Seong SY, Kim KR, Lee GB, Kim KS. 2011.
Prevalence and risk factors of chronic rhinosinusitis in Korea.
Am J Rhinol Allergy 25(3):117-121
Kweon N, Koh B. 2005. Dietary behaviors and vegetables intakes of elementary school students at Daegu and Gyeong-Sang Buk Do.
Korean J Food Cookery Sci 21(4):496-504
Lee B. 2004. A comparative study on dietary life and recognition of diet related factors in elementary, middle, and high school students. J Korean Diet Assoc 10(3):364-374
Meltzer EO, Hamilos DL, Hadley JA, Lanza DC, Marple BF, Nicklas RA, Bachert C, Baraniuk J, Baroody FM, Benninger MS, Brook I, Chowdhury BA, Druce HM, Durham S, Ferguson B, Gwaltney JM, Kaliner M, Kennedy DW, Lund V, Naclerio R, Pawankar R, Piccirillo JF, Rohane P, Simon R, Slavin RG, Togias A, Wald ER, Zinreich SJ. 2004. Rhinosinusitis: establishing definitions for clinical research and patient care". J Allergy Clin Immunol 114(Suppl 6):155-212
Ministry of Health & Welfare. 2010. The 2009 Korean National Health and Nutrition Examination Survey IV.
Miyake Y, Sasaki S, Ohya Y, Miyamoto S, Matsunaga I, Yoshida T, Hirota Y, Oda H. 2005. Soy, isoflavones, and prevalence of allergic rhinitis in Japanese women: the Osaka Maternal and Child Health Study". J Allergy Clin Immunol 115(6): 1176-1183 Miyake Y, Sasaki S, Tanaka K, Ohya Y, Miyamoto S, Matsunaga I,
Yoshida T, Hirota Y, Oda H, Osaka M. 2007. Fish and fat intake and prevalence of allergic rhinitis in Japanese females:
the Osaka Maternal and Child Health Study. J Am Coll Nutr 26(3):279-287
Novak N, Leung DY. 2005. Diet and allergy: you are what you eat?.
J Allergy Clin Immunol 115(6):1235-1237
Ozdemir O. 2010. Any benefits of probiotics in allergic disorders?
Allergy Asthma Proc 31(2):103-111
Pala G, Pignatti P, Perfetti L, Avanzini MA, Calcagno G, Preziosi D, Moscato G. 2010. Occupational rhinitis and asthma due to cabreuva wood dust. Ann Allergy Asthma Immunol 104(3):268-269
Settipane RA, Charnock DR. 2007. Epidemiology of rhinitis: allergic and nonallergic. Clin Allergy Immunol 19:23-34
Tamay Z, Akcay A, Ones U, Guler N, Kilic G, Zencir M. 2007.
Prevalence and risk factors for allergic rhinitis in primary school children. Int J Pediatr Otorhinolaryngol 71(3):463-471
Tan RA, Corren J. 2011. The relationship of rhinitis and asthma, sinusitis, food allergy, and eczema. Immunol Allergy Clin North Am 31(3):481-491
Tricon S, Willers S, Smit HA, Burney PG, Devereux G, Frew AJ, Halken S, Host A, Nelson M, Shaheen S, Warner JO, Calder PC. 2006. Nutrition and allergic disease. Clin Exp Allergy 6:117-188
Van Crombruggen K, Zhang N, Gevaert P, Tomassen P, Bachert C.
2011. Pathogenesis of chronic rhinosinusitis: inflammation. J Allergy Clin Immun 128(4):728-732
Vliagoftis H, Kouranos VD, Betsi GI, Falagas ME. 2008. Probiotics for the treatment of allergic rhinitis and asthma: systematic review of randomized controlled trials. Ann Allergy Asthma Immunol 101(6):570-579
Wallace DV, Dykewicz MS, Bernstein DI, Blessing-Moore J, Cox L, Khan DA, Lang DM, Nicklas RA, Oppenheimer J, Portnoy JM, Randolph CC, Schuller D, Spector SL, Tilles SA. 2008. The diagnosis and management of rhinitis: an updated practice parameter. J Allergy Clin Immun 122(suppl 2):S1-84
Waserman S, Watson W. 2011. Food allergy". Allergy Asthma Clin Immun 10:7 Suppl 1):S7
Yang SH, Kim EJ, Kim YN, Seong KS, Kim SS, Han CK, Lee BH.
2009. Comparison of eating habits and dietary intake patterns between people with and withouth allergy. Korean J Nutr 42(6):523-535
Yao TC, Chang CJ, Hsu YH, Huang JL. 2010. Probiotics for allergic diseases: realities and myths. Pediatr Allergy Immunol 21(6):900-919