Korean J Gastroenterol Vol. 63 No. 6, 369-372 http://dx.doi.org/10.4166/kjg.2014.63.6.369 pISSN 1598-9992 eISSN 2233-6869
CASE REPORT
Korean J Gastroenterol, Vol. 63 No. 6, June 2014 www.kjg.or.kr
복통을 일으키는 벽측 복막 지방종 1예
방창석, 김연수, 백광호, 한상학1
한림대학교 의과대학 내과학교실, 병리학교실1
A Case of Lipoma of Parietal Peritoneum Causing Abdominal Pain
Chang Seok Bang, Yeon Soo Kim, Gwang Ho Baik and Sang Hak Han1
Departments of Internal Medicine and Pathology1, Hallym University College of Medicine, Chuncheon, Korea
Lipomas are common benign tumors of mature adipose tissue, enclosed by thin fibrous capsules. They can occur on any part of the body; however, peritoneal lipoma is extremely rare. We encountered a case of a 75-year-old man presenting with intermittent abdominal pain, who had undergone right hemicolectomy due to colon cancer. Abdominal computerized tomography showed a well-defined heterogenous fatty mass measuring 4.5×3.5 cm in size, suggesting fat necrosis located in the abdominal wall. Laparotomy showed a very large soft mass of peritoneum. Pathologically, the tumor was diagnosed as lipoma containing fat necrosis located in parietal peritoneum not fixed to any organs, but with small bowel adhesion. Due to its rare etiologic origin and obscure cause of development, we report on a case of lipoma of parietal peritoneum causing abdominal pain.
(Korean J Gastroenterol 2014;63:369-372) Key Words: Lipoma; Peritoneum
Received October 5, 2013. Revised November 28, 2013. Accepted November 29, 2013.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
교신저자: 김연수, 200-704, 춘천시 삭주로 77, 한림대학교춘천성심병원 내과
Correspondence to: Yeon Soo Kim, Department of Internal Medicine, Hallym University Chuncheon Sacred Heart Hospital, 77 Sakju-ro, Chuncheon 200-704, Korea.
Tel: +82-33-240-5821, Fax: +82-33-241-8064, E-mail: kimyeonsoo@hallym.or.kr Financial support: None. Conflict of interest: None.
INTRODUCTION
Lipomas are the most common and benign soft tissue neo- plasms occurring throughout the entire body.1-3 Most lip- omas rarely cause symptoms due to their superficial location and small size, therefore, surgical resection is required only under conditions of pain, cosmesis, rapid growth rate, and concerns over diagnosis.2-6 However, lipomas of the abdomi- nal cavity such as mesentery, omentum, retroperoneum, and peritoneum are rare.6-9 Among them, lipoma of the peri- toneum is extremely rare. To the best of our knowledge, only one case of lipoma of the parietal peritoneum has been reported.10 We describe herein a case of lipoma located in the parietal peritoneum causing abdominal pain, which was proven by surgery.
CASE REPORT
A 75-year-old male presented to our hospital complaining of a one-week history of intermittent right lower abdominal pain. For three years, the patient had been free of symptoms after having undergone right hemicolectomy for treatment of colon cancer. Initial vital signs were blood pressure 110/60 mmHg, temperature 98.6oF, respiratory rate 22/min, and pulse rate 70 beats/min. The BMI of the patient was 26.8 kg/m2 (162 cm, 70.3 kg). A soft mass on the right lower quad- rant abdomen was detected on palpation. Mild tenderness, but no rebound tenderness, was observed. Laboratory tests showed no specific findings, including CRP of 1.13 mg/dL and CEA of 2.3 ng/mL. No lesions were observed on endo- scopic examination; however, colon polyps were observed.
370 방창석 등. 벽측 복막 지방종
The Korean Journal of Gastroenterology
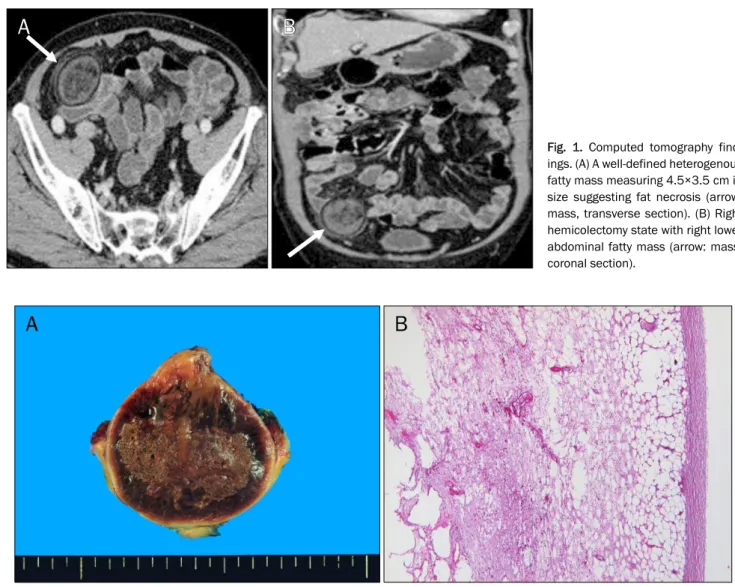
Fig. 1. Computed tomography find- ings. (A) A well-defined heterogenous fatty mass measuring 4.5×3.5 cm in size suggesting fat necrosis (arrow:
mass, transverse section). (B) Right hemicolectomy state with right lower abdominal fatty mass (arrow: mass, coronal section).
Fig. 2. Histologic findings. (A) Macroscopic finding. The cut surface of the mass shows a brownish tan hemorrhagic color with a peripheral yellow capsule. (B) Microscopic finding shows mature adipose tissue with no evidence of malignancy (H&E, ×100).
Abdominal computed tomography showed a well-defined heterogenous fatty mass measuring 4.5×3.5 cm in size sug- gesting fat necrosis (Fig. 1). Epiploic appendagitis and fat containing tumors such as dermoid, lipoma, and lip- osarcoma were suspected initially. However, the symptoms did not respond to pain management. For the definite diag- nosis and relief of symptoms, surgical management was decided. Laparotomy showed a very large soft mass of the ab- dominal wall which was not fixed to any organs. Small bowel adhesion was also observed.
Complete excision and adhesiolysis were performed successfully. The resected specimen showed an ovoid fatty mass measuring 6.5×5.5×4.5 cm in size, which was at-
tached to the parietal peritoneum. The external surface showed a well encapsulated appearance. On section of the resected specimen, the cut surface showed a brownish tan hemorrhagic appearance with a peripheral yellow capsule (Fig. 2A). On microscopic examination, there was no obvious evidence of malignancy, implying recurrence of colon cancer (Fig. 2B). Pathologically, the tumor was diagnosed as a lip- oma containing fat necrosis. The cause of fat necrosis was thought to be associated with ischemia due to post-operative adhesion of colon cancer. The symptoms showed improve- ment after surgery and the patient has remained in good con- dition for over one year.
Bang CS, et al. Lipoma of Parietal Peritoneum 371
Vol. 63 No. 6, June 2014
DISCUSSION
Lipomas are common benign tumors of mature adipose tissue, enclosed by thin fibrous capsules. They are sub- classified according to their histopathologic characteristics as conventional lipoma, fibrolipoma, angiolipoma, fusiform cell lipoma, myelolipoma, and pleomorphic lipoma.11 Differen- tial diagnosis includes lipoblastoma, lymphangioma, sarco- ma, lymphoma, and liposarcoma. Radiologic, histologic, and clinical findings are important in differentiation of soft tissue tumors. The diagnosis is usually made incidentally due to slow growth of the tumors, which rarely cause symptoms. The finding of lipoma on CT is a homogenous fat containing mass with a thin capsule. Other fat containing masses such as an- giomyolipoma, myelolipoma, or trauma should be consid- ered in the differential diagnosis. Treatment is usually un- necessary; however, surgical treatments are occasionally re- quired due to pain, cosmetic reasons, rapid growth rate, and unclear diagnosis.2-6 Endoscopic treatments are possible if they are located in the accessible area of the gastrointestinal tract. Recurrence of an excised lipoma is not common.4-6 Lipomas in the abdominal cavity, such as mesentery, omen- tum, and retroperitoneum, are rare. They can produce vari- ous symptoms, including indigestion, abdominal pain, diar- rhea, constipation, ulcer, intestinal obstruction and even in- tussusception, requiring surgical or endoscopic treat- ments.6-9 In addition, lipoma of the parietal peritoneum is ex- tremely rare. Only one case has been reported so far.10 According to the case report, abdominal pain was the chief complaint and diagnostic laparotomy showed a lipoma measuring 6×4×2 cm in size, similar to our case in symptom and size.10
Besides its rarity, lipoma of the parietal peritoneum is ob- scure in its origin and pathogenesis. First, there is some de- bate with regard to whether lipoma of the parietal peritoneum is a primary peritoneal tumor.12 In fact, some reports have loosely classified subperitoneal lipoma as primary peritoneal tumors, whereas others did not.12,13 However, regarding the normal existence of adipose tissue of the peritoneum, lipoma can theoretically develop from peritoneal fat tissue. In addi- tion, fat seeding by peritoneal fluid from any other sub- peritoneal area can lead to development of lipoma of the peritoneum. Second, the pathogenesis of lipoma is not com- pletely understood. Although little is known about the patho-
genesis of lipoma, the following possible theories have been proposed.14-16 The first theory is that lipoma develops from misplaced embryonic adipose tissue. The next theory is that hyperproliferation of adipose tissue simply leads to develop- ment of lipoma. The third theory is that trauma-related fat herniation through tissue planes subsequently leads to de- velopment of lipoma- and trauma-induced cytokine release, triggering pre-adipocyte differentiation and maturation. The fourth theory is that infection, chronic stimulation, and obe- sity could be a potential etiology. Although lipoma consists of an overgrowth of fat tissue, the association with triglyceride and cholesterol is not certain. In addition, the association with diabetes or atherosclerosis has not been investigated.
Finally, the final debate is not a theory but genetic evidence that rearrangements of chromosome 12q13q15 with chro- mosome 3 was observed in approximately 50-60% of lipomas. Due to the rearrangements, some fusion genes were reported, represented by LPP-HMGA2 (lipoma pre- ferred partner-high mobility group A2), but are not available clinically.17,18
In this case, regarding the patient’s history of right hemi- colectomy three years ago, operation as trauma or adipose tissue seeding during surgery may be a possible cause of lip- oma development. Regarding the slow growth rate of lipoma, the excised lipoma is very large, and, therefore, the lipoma may be of primary peritoneal origin already existing prior to right hemicolectomy. In addition, regarding the most reliable cause of adhesion of lipoma with the small intestine as right hemicolectomy, lipoma may be the primary peritoneal tumor.
A patient’s high BMI supports this hypothesis of idiopathic development.
We are uncertain as to whether the lipoma of the peri- toneum is a primary peritoneal tumor and whether it is the cause among trauma, adipose tissue seeding, and idiopathic reason. There is no way to prove the cause of development of lipoma except with clinical assumption. The benign course of the disease and few treatment indications may further lim- it investigation regarding the pathophysiology of the lipoma.
In conclusion, as a rare cause of abdominal pain, lipomas could be listed for differential diagnosis.
REFERENCES
1. Piattelli A, Fioroni M, Iezzi G, Rubini C. Osteolipoma of the
372 방창석 등. 벽측 복막 지방종
The Korean Journal of Gastroenterology tongue. Oral Oncol 2001;37:468-470.
2. Thompson WM, Kende AI, Levy AD. Imaging characteristics of gastric lipomas in 16 adult and pediatric patients. AJR Am J Roentgenol 2003;181:981-985.
3. Rapidis AD. Lipoma of the oral cavity. Int J Oral Surg 1982;
11:30-35.
4. Pfeil SA, Weaver MG, Abdul-Karim FW, Yang P. Colonic lipomas:
outcome of endoscopic removal. Gastrointest Endosc 1990;36:
435-438.
5. Tascilar O, Cakmak GK, Gün BD, et al. Clinical evaluation of sub- mucosal colonic lipomas: decision making. World J Gastroenterol 2006;12:5075-5077.
6. Tamura S, Yokoyama Y, Morita T, Tadokoro T, Higashidani Y, Onishi S. "Giant" colon lipoma: what kind of findings are neces- sary for the indication of endoscopic resection? Am J Gastroen- terol 2001;96:1944-1946.
7. Singaporewalla RM, Thamboo TP, Rauff A, Cheah WK, Mukherjee JJ. Acute abdominal pain secondary to retroperitoneal bleeding from a giant adrenal lipoma with review of literature. Asian J Surg 2009;32:172-176.
8. Wolko JD, Rosenfeld DL, Lazar MJ, Underberg-Davis SJ. Torsion of a giant mesenteric lipoma. Pediatr Radiol 2003;33:34-36.
9. Ilhan H, Tokar B, Işiksoy S, Koku N, Pasaoglu O. Giant mesenteric lipoma. J Pediatr Surg 1999;34:639-640.
10. Barut I, Tarhan OR, Cerci C, Ciris M, Tasliyar E. Lipoma of the pari-
etal peritoneum: an unusual cause of abdominal pain. Ann Saudi Med 2006;26:388-390.
11. de Visscher JG. Lipomas and fibrolipomas of the oral cavity. J Maxillofac Surg 1982;10:177-181.
12. Levy AD, Arnáiz J, Shaw JC, Sobin LH. From the archives of the AFIP: primary peritoneal tumors: imaging features with patho- logic correlation. Radiographics 2008;28:583-607.
13. Pickhardt PJ, Bhalla S. Primary neoplasms of peritoneal and sub-peritoneal origin: CT findings. Radiographics 2005;25:983- 995.
14. Weinberg T, Feldman M Sr. Lipomas of the gastrointestinal tract.
Am J Clin Pathol 1955;25:272-281.
15. Haller JD, Roberts TW. Lipomas of the colon: a clinicopathologic study of 20 cases. Surgery 1964;55:773-781.
16. Signorini M, Campiglio GL. Posttraumatic lipomas: where do they really come from? Plast Reconstr Surg 1998;101:699-705.
17. Moretti-Ferreira D, Koiffmann CP, Souza DH, Diament AJ, Wajntal A. Macrocephaly, multiple lipomas, and hemangiomata (Bannayan-Zonana syndrome): genetic heterogeneity or autoso- mal dominant locus with at least two different allelic forms? Am J Med Genet 1989;34:548-551.
18. Zhang H, Erickson-Johnson M, Wang X, et al. Molecular testing for lipomatous tumors: critical analysis and test recommen- dations based on the analysis of 405 extremity-based tumors.
Am J Surg Pathol 2010;34:1304-1311.