대 한 방 사 선 의 학 회 지 1991 ; 27(4) ‘ 567~571
Journal of Korean Radiological Society, July, 1991
척추 결핵 Gadolinium 조영증강 자기공명 영상*
서울대학교 의과대학 방사선과학교실
김성문·강흥식·장기현·한문희·한만청 - Abstract-
Spinal Tuberculosis: Gadolinium-enhanced MRI*
Sung Moon Kim, M.D., Heung Sik Kang, M.D., Kee Hyun Chang, M.D., Moon Hee Han, M.D., Man Chung Han, M.D.
Department o[ Radiology. Seoul National University College o[ Medicine
To evaluate the value of gadolinium (Gd)-enhancement in the examination of spinal tuberculosis using magnetic resonance (MR) imaging in 25 surgically-confirmed cases of spinal tuberculosis. we studied (1) the ability of MR to show the extent of the lesions among Gd-enhanced Tl weighted images and non-contrast Tl, proton density.
and T2 weighted images, and (2) the specific contrast enhancing pattems of the lesions. The Gd-enhanced T l-weighted images were better in evaluating the extent of the disease than the noncontrast T 1. T2. and proton density images in 68%, 52%, and 68%. respectively. After Gd-DTPA enhancement, the inflammatory tissues showed 2 types of rim enhancement‘ (1) irregular thick enhancing wall with centrallow intensity and (2) uniformly thin rim enhance- ment in large mass suggesting cold abscess.
We concluded that Gd enhancement was valuable in MR examination of spinal tuberculosis in evaluating the disease extent as well as specific diagnosis by characteristic rim enhancement
Index Words: Spine. infection 30.23 Spine. MR studies 30.1214 Tuberculosis, skeletal 30.23
서 론
우리나라에서 척추 감염의 대부분을 차지하는 척추 결 핵은 아직도 흔하게 발견되며 이의 방사선학적 진단 방 볍으로 단순 X 선 촬영과 CT 가 이용되어 왔는데 (1-9) , 연부 조직간의 대조도가 우수하며 다평연상을 얻을 수 있는 장점을 지난 자기공명영상 (MRI) 의 개발은 진단 및 병변의 범위 파악에 도움을 주고 있다. 그러나 저자들이 아는 한 척추 결핵의 자기공명영상소견에 대한 보고는 많지 않으며(1 0-13) , 더우기 Gadolinium(Gd) 조영증강 소견의 보고는 아주 드물어(1 0 , 13) 척추 결핵의 MRI 진 단시 Gd 조영증강의 의의를 알아보고자 후향적으로 이 연구를 시행하였다.
대상 및 방법
서울대학병원에서 1988 년 12 월부터 1990 년 9 월까지 MRI 를 시행하여 척추 결핵으로 진단받고 수술로 확진 된 51 예 중 Gd 조영증강을 시행한 25 예를 대상으로 하 였다. 연령은 3 세에서 52 세까지로 평균 33세이었으며, 남녀의 비는 12 : 13 이었다. 5 예에서 0.5T 스캐너 (Goldstar, Supertec 5000) 를, 나머 지 20 예 에 서 2.0T 스캐너 (Goldstar, Spectro 20000) 를 이용하였다. 스핀 에코 기법으로 Tl 강조영상 (TR/TE=500- 800 msec/30 msec)‘ 양자 농도영상 (1300-2500/30 40), T2 강조영상 (1300-2500/65-85) 과 Gd-DTPA (gadolinium diethylenetriaminepentaacetic acid) 를 체 중
*본 논문은 1991 년도 서울대학교병원 특진 연구비 보조로 이루어졌음.
이 논문은 1991 년 4 월 12 일 접수하여 1991 년 5 월 31 일에 채 택되었음
대한방사선의학회지 1991; 27(4) : 567~57i
1 kg 당 0.1 mMol 로 정맥 주입한 후 Tl 강조영상 (Gd 하였다. 양자 농도영상과의 비교에서 17 예 (68 %)에서 Tl wr,500-900/30) 을 얻었으며 2 예에서 Gradient Gd- Tl WI 가 우수하였으며 (Fig. 2) 8 예 (32%) 에서 같 ech 。 기법으로 T2* 강조영상 (200/12) 을 얻었으며, 촬 았다. T2 강조영상보다 우수한 Gd- T1 WI 는 13 예 영면은 시 상면, 횡단면, 및 관상변을 모두 혹은 이중 2 (52 %)이었으며 (Fig. 3) 11 예 (44%) 에서 같았으며 1 예에 개의 촬영연만을 얻었다. 결핵 병변의 중심부로 생각되 서 T2 강조영상이 우수하였다.
는 부위로부터 연속적인 척추체에서 중심부와 같은 신호 염증조직은 Tl 강조영상에서 저신호강도로 나타나며 강도를 보이는 부분과 척추체의 병변주위로 정상과 다른 T2 강조영상에서 고신호강도로 보였으며, Gd 조영증강 신호강도의 척추체 측부 종괴를 병변의 범위에 포항시켰 후의 Tl 강조영상에서 테두리 조영증강 (rim enhance.
으며, 서로 같은 촬영변에서 Gd-Tl WI 와 Tl, T2 양자 ment) 을 전예에서 보였는데 비교적 고르고 앓은 테두리 농도영상 간의 병변의 범위를 비교하였으며, Gd 조영증 (evenly thin wall) 와 불규칙적인 두께의 테두리 (irregu.
강 후 영변의 특정적인 소견을 찾고자 하였다 lar thick wall) 의 두 형태를 모두 보였다. 척추체내 또는
7~ E븐 과
24 예에서 추간판 (intervertebral disc) 의 침범이 있었 으며 전예에서 농양으로 인한 척추주위인대 (paraspinal ligament) 의 융기가 있었고, 5 예에서 척추주위인대의 파 열을 볼 수 있었으며 인대의 파열이 동반된 경우 그 주
그 근접부의 염증 조직은 불규칙적인 두께의 테두리 조 영증강을 보였으며 한냉농양 (cold abscess) 으로 생각되 는 척추에서 멀리 떨어진 부위의 병변은 앓고 고른 테두 리 조영증강을 보였t:j- (Fig -t)
고 찰
위에 커다란 한냉능양을 형성하였다. 단순 X 션 촬영 또 척추 결핵은 척추체의 전측부에서 시작하여 서서히 진 는 CT 로 9 예에서 병변 내의 석회화를 볼 수 있었으며, 행하여 척추체 주위 인대의 밑을 통하여 척추체 주위에 통일한 위치에서 자기공명영상으로는 6 예에서 발견할 농양을 형성하며 척추강으로도 침범하는데 결핵균은 단 수 있었으며 Tl, T2. 및 양자농도영상에서 모두 저신호 백질 분해효소를 생산하지 않아서 비교적 진행된 경우에 강도를 보였다 추간판을 침범한다 (3). 단순 X 선 촬영에서는 척추체의 자기공명영상에서 Gd 조영증강 전과 후에 보이는 결 파괴, 척추체 주위의 종괴 형성, 추간판 간격의 소실,
핵 병 변의 범위 비교는 Gd- Tl WI 가 17 예 (1 7/25= 척추후굴증과 석회화 등을 볼 수 있으나, 정확한 침습 68 %)에서 Tl 강조영상보다 우수하였고 (Fig. 1), 7 예 범위를 알 수 없으며 활동성을 나타내어 주지 못한다 (28 %)에서 같았으며, 1 예 (4%)에서 Tl 강조영상이 우수 (12). 또한 CT 를 이용하면, 작은 골파괴와 소량의 농양
a b
- 568 --
Fig, 1, Tl weighted image vs. Gd- enhanced Tl weighted image a. Non-contrast Tl weighted image (TR/TE 500/30) shows a large mass involving the odontoid process and C2 body (arrows) with a small abscess anterior to the anterior arch of C 1 (arrowheads).
b. Tl weighted image (800/30) after . . Gd-DTPA administration shows dif-
fuse enhancement of C 1, C2, C3, and the sUITounding inflammatory mass (arrows). Note the thin-walled peripheral rim enhancement with central area of low signal intensity representing the abscess (ar- rowheads)
a b
a b
김성문 외 , 척 추 걸 핵
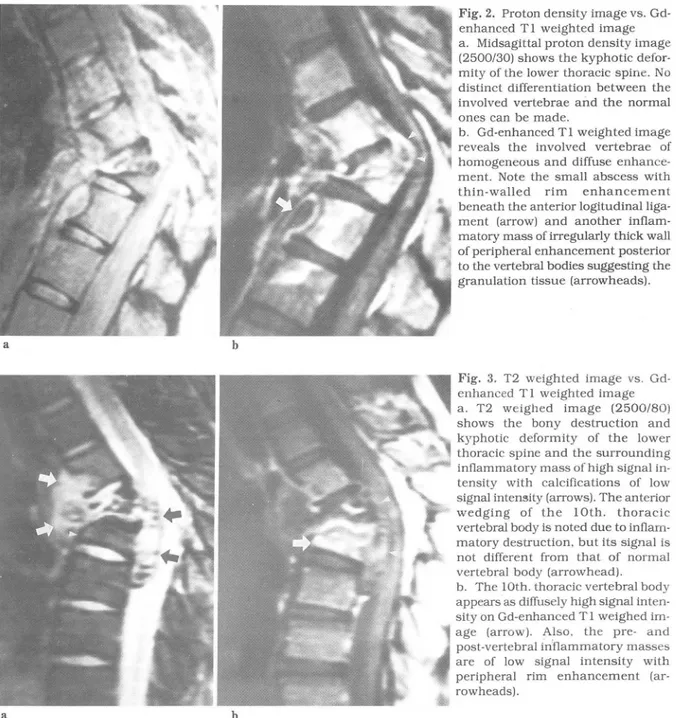
Fig. 2. Proton density image vs. Gd- enhanced Tl weighted image a. Midsagittal proton density image (2500/30) shows the kyphotic defor- mity of the lower thoracic spine. No distinct differentiation between the involved vertebrae and the normal ones can be made
b. Gd-enhanced Tl weighted image reveals the involved vertebrae of homogeneous and diffuse enhance- ment. Note the small abscess with thin-walled rim enhancement beneath the anterior logitudinalliga- 훨 ment (arrow) and another inflam- matory mass of irregularly thick wall of peripheral enhancement posterior to the vertebral bodies suggesting the granulation tissue (arrowheads)
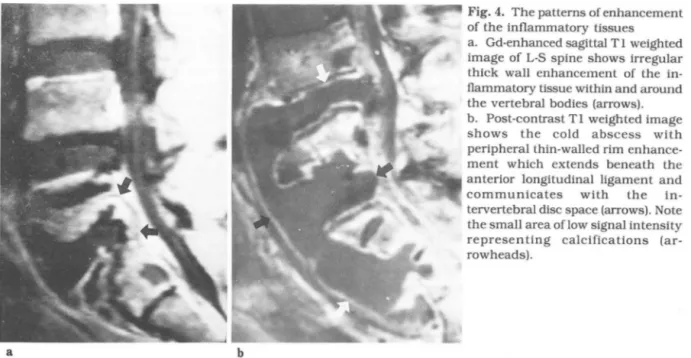
Fig. 3. T2 weighted image vs. Gd- enhanced Tl weighted image a. T2 weighed image (2500/8이
shows the bony destruction and kyphotic deformity of the lower thoracic spine and the surrounding inflammatory mass of high signal in- tensity with calcifications of low signal intensity (arrows). The anterior wedging of the 10th. thoracic vertebral body is noted due to inflam matory destruction. but its signal is not different from that of normal vertebral body (arrowhead)
b. The 10th. thoracic vertebral body appears as diffusely high signal inten- sity on Gd-enhanced Tl weighed im- age (arrow). Also. the pre- and post-vertebral inflammatory masses are of low signal intensity with peripheral rim enhancement (ar rowheads).
및 척수강으로의 침범 여부를 알 수 있으나 횡단면 만을 도의 차이가 거의 없어 발견이 쉽지 않으며, 특히 척수 얻을 수 있기에, 전체적인 모양을 파악하기 어려우며 추 강으로 파급된 경우에는 정상적인 저신호강도의 척수액 간판의 침범을 정확하게 알 수 없다(2 , 8 , 12). 이에 반 과 구분이 어려우며 척수강으로의 파급이 심해 척수의 해, 다평면상을 얻을 수 있으며 조직간의 대조도가 우수 압빅으로인한 변형이 있어야 발견이 용이하다. Proton 한 자기공명영상은 척추 결핵의 진단은 물론 병변의 범 및 T2 강조영상에서 염증조직과 농양은 고신호강도를 위를 정확하게 파악하는데 유용한 것으로 알려져 왔다 보이므로 성인의 경우에 척추체가 지방골수(fat marrow)
(9-13). 로서 저신호강도를 보여 구분이 가능하나, 촬영 시간
Tl 강조영상에서 염증조직과 한냉농양은 저선호강도 (acquisition time) 이 길어서 환자의 웅직임과 척수액의 로 나타나므로 정상적으로 저신호강도를 보이는 적색골 박동으로 인한 진정상 (artifact) 이 생기므로 상이 션명하 수 (red marrow) 내의 병변은 주위의 정상 부분과 신호강 지 않으며 병변이 척수강으로 파급된 경우에 정상적으로
대한방사선의학회지 1991 ; 27(4) : 567~571
a b
고신호강도를 보이는 척수액과 구별이 어렵다. 그러나 Gd 조영증강 후의 Tl 강조영상은 촬영 시간이 짧아 환 자의 움직임과 척수액의 박동으로 인한 진정상이 적어 선명한 상을 나타내며, 염증조직과 농양벽이 강한 조영 증강을 보이므로 저신호강도의 척수액, 정상 추간판 및 적색골수와 구분이 잘 되며 척수막의 조영증강을 보이는 지 망막염 (arachnoiditis) 의 발견 이 용이 하다(13 , 14).
척추체의 파괴를 통반하며 척추체 측부의 종괴를 형성 하는 질환으로서 화농성 척추염 (pyogenic spondylitis), 브루셀라 척추염 (brucellar spondylitis) 과 척추 종양이 있는데, 화농성 척추염의 경우 추간판 중심으로 병변이 파급되며 골파괴가 심하고 척추체 측부의 종괴형성이 결 핵의 경우보다 약하며 석회화의 동반이 없다(1 5). 브루 셀라균에 감염된 동물조직이나 우유를 통해서 전염되는 브루셀라 척추염은 우리나라에서 드물며 성년의 남자에 게 많으며 척추체 측부의 총괴형성이 경미하며 Gd 조영 증강시 테두리 조영증강보다 종괴 전체에 균일한 조영증 강을 보이므로 결핵의 경우와 감별이 가능하다 (9 , 13).
척추에 생긴 종양의 경우에 척추체 측부의 종괴 형성이 없거나 경미하며 병변이 척추의 후부 (posterior element) 까지 파급되며 하나의 척추체에 국한되며 추간판으로의 침범이 드문 점이 결핵의 경우와 다르다 (15).
결론적으로 Gd 조영증강 후의 Tl 강조영상은 척추결 핵 병변의 범위 파악에 가장 좋았음은 물론, 염증조직의 테두리 조영중강을 보이는 특징적인 소견을 보여 진단에 도 도움이 되었다.
Fig. 4. The patterns of enhancement of the inflammatory tissues a. Gd.enhanced sagittal Tl weighted image of L-S spine shows irregular thick wall enhancement of the in.
flammatory tissue within and around the vertebral bodies (arrows).
b. Post-contrast Tl weighted image shows the cold abscess with peripheral thin-walled rim enhance- ment which extends beneath the anterior longitudinal ligament and communicates with the in- tervertebral disc space (arrows). Note the small area oflow signal intensity representing calcifications (ar- rowheads).
참 고 문 헌
1. 임승수, 김충현, 이병철, 조준식. 척추 결핵의 전산화 단층촬영술에 대한 고찰. 대한방사선의학회지 1986 ; 22 : 848-857
2. Whelan MA. Naidich DP. Post JD. Chase NE. Com- puted tomography of spinal tuberculosis. JCAT 1983: 7:25-30
3. Weaver P. Lifeso RM. The radiological diagnosis of tuberculosis of the adult spine. Skeletal Radiol 1984;
12:178-186
4. Maritz NGJ. De Viìliers JFK. Van Castricum OQS Computed tomograph in tuberculosis of the spine Comput Radiol 1982; 6:1-5
5. Price AC. Allen JH. Eggers FM. Shaff MI. Everette JA. Intervertebral disk-space infection: CT changes.
Radiology 1983; 149:725-729
6. 8ell D. Cockshott WP. Tuberculosis ofthe vertebral pedicles. Radiology 1971; 99:43-48
7. Chapman M. Murray RO. Stoker DJ. Tuberculosis of the bones and joints. Semin Roentenol 1979;
14(4):266-282
8. LaBerge JM. 8rant-Zawadzki M. Evaluation ofPott’S
disease with computed tomography.Neuroradiology 1984; 26:429-434
9. Sharif HS. Aideyan OA. Clark DC. et al. 8rucellar and tuberculous spondylitis‘ comparative imaging features. Radiology 1989; 171 :419.425
- 570 -
김성문 외 : 척 추 걸 핵
10. DeRoos A. van Persijn van Meerten EL. Bloem JL. Granulomatous spinal infections: MR imaging Bluemm RG. MRI oftuberculous spondylitis. AJR Radiology 1990; 177:101-107
1986; 146:79-82 14. Chang KH. Han MH. Choi YW. Kim 10. Han MC. Kim 11. Smith AS. Weinstein MA. Mizushima A et al. MR im- CW. Tuberculous arachnoiditis of the spine: findings aging characteristics of tuberculous spondylitis vs on myelography. CT. and MR imaging. AJNR 1989;
vertebral osteomyelitis. AJNR 1989; 10:619-625 10: 1255-1262
12 강흥식, 석세일, 장기현, 한만청. 척추 결핵의 자기공 15. Van Lom KJ. Kellerhouse LE. Pathria MN. et al. In- 명 영 상. 대 한방사사산 의 학회 지 1988 ; 24(3) : 421- fection versus tumor in the spine: criteria for distinc-
427 tion with CT. Radiology 1988: 166:851-855
13. Sharif HS. Clark DC. Aabed MY. et al