pISSN 2288-9272 eISSN 2383-8493 J Oral Med Pain 2014;39(4):156-162 http://dx.doi.org/10.14476/jomp.2014.39.4.156
A Novel Treatment of Recurrent Temporomandibular Joint Dislocation with Intermaxillary Fixation Using Microimplant: A Case Report
In-Kyung Kee*, Jin-Seok Byun*, Jae-Kap Choi
Department of Oral Medicine, School of Dentistry, Kyungpook National University, Daegu, Korea
Received October 8, 2014 Revised October 16, 2014 Accepted October 31, 2014
Dislocation of temporomandibular joint (TMJ) is troublesome condition which was most com- monly shown far anteriorly displaced mandibular condyle to the articular eminence, thereby make it impossible to close one’s mouth. It is often referred to as ‘open lock’ in clinically.
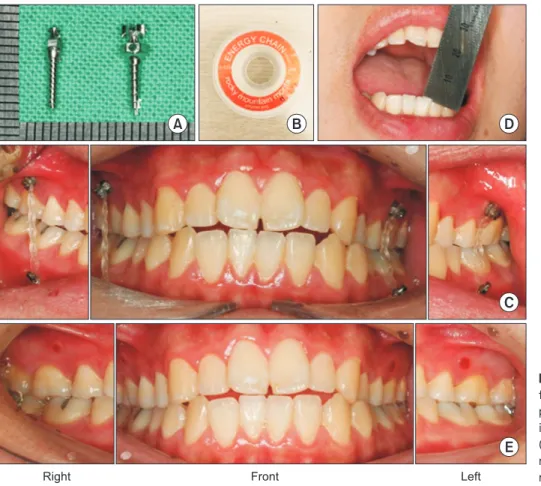
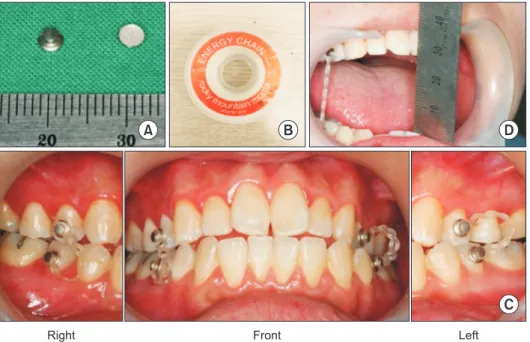
Although anatomical modification of the articular eminence through eminectomy has been considered most satisfactory and efffective treatment for managing the recurrent dislocation, it seldom performs clinically due to its invasiveness and patient’s reluctance. We thought a short- term intermaxillary fixation could be of benefit to the patient suffering from recurrent dislo- cation. A 21-year-old male patient with recurrent TMJ dislocation which had developed after excessive mouth opening, was successfully treated with intermaxillay fixation using microim- plant for 2 months. It is more conservative and less complicated method than eminectomy in treating recurrent TMJ dislocation. Transient intermaxillary fixation using microimplant and elastics could be one of treatment options for recurrent TMJ dislocation.
Key Words: Dental implants; Dislocations; Temporomandibular disorders; Temporomandibular joint
*These authors equally contributed to this study.
Correspondence to:
Jae-Kap Choi
Department of Oral Medicine, School of Dentistry, Kyungpook National University, 2177, Dalgubeol-daero, Jung-gu, Daegu 700-412, Korea Tel: +82-53-600-7321 Fax: +82-53-426-2195 E-mail: [email protected]
injured joint lose its function as passive restrictors and the masticatory muscles lose coordination during mouth open- ing and closing. In addition, specific anatomic characteris- tics of TMJ such as steepness of the articular eminence and joint laxity may predispose a patient to TMJ dislocation. A TMJ articular eminence which showed “short steep posterior slope” and “long flat anterior slope” was generally regarded vulnerable to dislocation.
2)In treating recurrent TMJ dislocation, behavioral modifi- cation is the primary treatment option. However, if the pa- tient’s hazardous habit could not be managed, additional methods should be considered to restrict mouth opening precisely. Although many treatment modalities have been suggested in the literature,
3,4)only surgical alteration of TMJ called eminectomy or eminoplasty has been regarded as definitive in treating TMJ dislocation.
5)No satisfactory
INTRODUCTION
Temporomandibular joint (TMJ) dislocation is character- ized when the mandibular condyle moves far anteriorly during opening and passes the articular eminence eas- ily. Subsequently the ligaments around the joint are of- ten stretched by an intra-articular effusion, which induces various physical and social problems such as pain, closing limitation, difficulty in speech and chewing. According to Diagnostic Criteria for Temporomandibular Disorders 2014 guideline,
1)if dislocated condyle was voluntarily reduced, it is called “subluxation,” and if not, the term “luxation” was used. In general, dislocation of TMJ clinically designated
“luxation” of TMJ.
Macrotraumatic event by extensive mouth opening is re- garded main cause of TMJ dislocation. The ligaments of
JOMP
Journal of Oral Medicine and PainCopyright Ⓒ 2014 Korean Academy of Orofacial Pain and Oral Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.