원 원 저저
서 론
국내 야생 버섯들 중 식용 가능한 버섯은 20-30종 정도 에 불과하며, 160여 종 이상의 독버섯이 존재한다. 국내 버섯 중독 사망 사고의 대부분은 amatoxin을 함유한 독 버섯에 의한 것이다. Amatoxin을 함유한 독버섯으로는 양파광대버섯(Amanita abrupta), 흰오뚜기광대버섯 (Amanita castanopsidis), 개나리광대버섯(Amanita subjunquillea), 흰알광대버섯(Amanita verna), 독우산
Amatoxin 중독 환자에서 Silymarin, Penicillin, N-acetylcysteine의 효과 비교: 체계적 고찰
연세대학교 의과대학 응급의학교실
최민우∙고동률∙공태영∙좌민홍∙유제성∙정성필
Comparison of Silymarin, Penicillin, N-acetylcysteine in Patient with Amatoxin Poisoning: A Systematic Review
Min Woo Choi, M.D., Dong Ryul Ko, M.D., Taeyoung Kong, M.D., Min Hong Choa, M.D., Je Sung You, M.D., Sung Phil Chung, M.D.
Department of Emergency Medicine, Yonsei University College of Medicine, Seoul, Korea
Purpose: This study was conducted to evaluate the clinical efficacy of pharmacologic treatment of amatoxin poison- ing patients.
Methods: Literature was accessed through PubMed, EMBASE, Cochrane library, KoreaMed, KISS and KMBASE.
Studies relevant to human use of pharmacologic therapy including silymarin, penicillin and N-acetylcysteine (NAC) for amanita poisoning were included. Case reports, letters, editorials and papers with insufficient information were excluded. Comparison of clinical outcomes (especially mortality and liver transplantation rate) in each study was analyzed.
Results: The final analysis included 13 retrospective studies. None of these studies showed direct comparisons of individual agents. Among 12 studies comparing silymarin vs penicillin, eight showed clinical superiority of silymarin.
Among eight studies comparing silymarin with NAC, six showed clinical superiority of silymarin. Among seven stud- ies of NAC vs penicillin, five showed clinical superiority of NAC.
Conclusion: This systematic review suggested that clinical superiority of various pharmacological agents used to treat amatoxin poisoning is debatable. Nevertheless, the available evidence suggests it is reasonable to consider combinations of multiple agents for patients with amanita poisoning. Further studies are required to establish a treatment regimen for amanita poisoning.
Key Words: Amatoxin, Poisoning, Silymarin, Silibinin, Penicillin, Acetylcysteine
책임저자: 정 성 필
서울특별시 강남구 언주로 211 연세대학교 의과대학 응급의학교실 Tel: 02) 2019-3030, Fax: 02) 2019-4820 E-mail: [email protected]
투고일: 2018년 5월 6일 1차 심사일: 2018년 5월 6일 게재 승인일: 2018년 6월 11일
* 이 논문은 특정단체의 재정적 지원이나 관련된 이해관계가 없습니다.
광대버섯(Amanita virosa) 등이 있다
1).
Amatoxin 중독의 치료는 보존적 치료와 약물요법, 투 석요법 그리고 간 이식까지 다양한 치료법이 사용되고 있 다. 이중 약물요법의 경우 silymarin, penicillin, N- acetylcysteine (NAC) 등이 대표적이며 이외에도 다양한 치료 약제가 단독 또는 혼합요법으로 사용되고 있다
2). Silymarin은 흰 무늬 엉겅퀴(milk thistle)의 추출물로 1) amatoxin의 간세포막 결합 억제, 2) 막간 수송에서 독소 와 경쟁적으로 작용, 3) 독소의 담즙산 배설과 장내순환 억제, 4) 손상된 간세포에서의 TNF-α분비 억제, 5) 손상 된 간세포의 단백질 합성 자극 기전을 통해 항독소 효과를 보인다고 알려져 있다
3). Penicillin은 Amatoxin 중독에 가장 많이 사용되어온 치료제 중 하나로 막 수송체인 OATP1B3에 경쟁적으로 결합하여 간 내로의 amatoxin 의 이동을 막는 기전을 통해 항독소 효과를 보인다고 보고 있다
4). NAC는 ROS scavenger와 glutathione 전구체로 작용하여 항독소 효과를 나타낸다고 보고 있다
2,5).
저자들은 Amanita species 버섯 중독 환자를 대상으로 대표적인 3가지 약물요법의 치료 효용성을 알아보기 위하 여 체계적 문헌고찰을 시행하였다.
대상과 방법
1. 문헌 검색 및 선정본 연구는 기존 문헌들의 체계적 고찰 연구로 Preferred Reporting Items for Systematic reviews and Meta- Analyses (PRISMA) 그룹이 제시한 체계적 문헌고찰 보 고지침에 따라 수행되었다. 문헌의 선정기준은 amatoxin 중독 환자를 대상으로 치료에 관한 내용이 포함된 경우로 하였다
6). 문헌 검색에 사용된 데이터베이스는 PubMed, Embase, Cochrane library, KoreaMed, Korean Studies
Information Service System (KISS), Korean Medical Database (KMbase) 등이었으며 데이터베이스에 사용한 검색식은 Table 1에 표기하였다.
검색은 두 명의 연구자에 의해 시행되었으며, 제외기준 으로는 1) 약물 투여군과 대조군을 비교한 경우 2) 주제와 관련이 없는 경우, 3) 환자의 임상 양상이 자세히 언급되 지 않은 증례 보고, 4) 학회 초록, 5) 영어나 한국어 이외 의 언어로 출판된 경우(영문 초록이 있는 경우는 포함) 등 은 제외 하였다. 최종 선정된 문헌은 EndNote (X8, Thomson Reuters)에 정리하여 중복된 문헌을 제거하였 다. 또한 문헌에 이용된 참고문헌들을 검토하여 빠진 문헌 이 있으면 추가하였다.
2. 논문의 질 평가
선택된 문헌의 질은 영국 Scottish Intercollegiate Guideline Network (SIGN)의 체크리스트를 이용하여 평가하였다. SIGN의 질 평가도구는 연구 유형에 따라 필 수 항목을 선정하고, level 1은 메타분석, 무작위 대조 실 험의 체계적 문헌고찰, 무작위 대조 실험이 해당하고, level 2는 환자 대조군 연구나 코호트 연구, 또는 이를 이 용한 체계적 문헌고찰이 해당하며, level 3는 증례보고 같 은 비 분석 연구, level 4는 전문가 의견 등이 해당된다.
해당 level의 조건에 모두 잘 또는 적절하게 수행되었을 경우‘++’로, 일부 항목이 불충분할 경우‘+’로, 대부분 충족되지 않았을 경우‘-’로 판정하였다
7).
3. 자료의 요약
필요한 항목과 문헌에 대한 간단한 요약표를 작성하였 다. 최종 선정된 문헌들을 검토하여 각 약제(silymarin, penicillin, NAC) 각 약제간의 치료 효과를 사망 및 간이
Table 1. Search strategy of databases
Database Hits Search strategy
PubMed 118 (“poisoning” [Mesh] OR “intoxication” [Mesh]) AND (amanita [Mesh] OR “mushroom poisoning”
[Mesh]) AND ((“silibinin” [mesh] OR “silibinin” [all fields]) OR (silymarin OR legalon OR milk thistle) OR penicillins [Mesh] OR acetylcysteine [Mesh])
Embase 500 (‘silibinin’/exp OR silibinin OR ‘sylimarin’/exp OR sylimarin OR penicillin OR acetylcysteine) AND (‘amanita’/exp OR amanita OR ‘mushroom’/exp OR mushroom) AND ([english]/lim OR [korean]/lim) Cochrane library 003 amanita OR amanita phalloides OR Amatoxin
KoreaMed 025 (amanita [ALL] or amatoxin [ALL] or mushroom [ALL] ) and (poisoning [ALL] or intoxication [ALL])
KMbase 068 Amanita
KISS 027 Amanita
* KISS: Korean studies information service system, KMbase: Korean medical database
식 비율을 기준으로 정리하였다.
결 과
1. 문헌 검색 결과
문헌검색을 통해 PubMed 118건, Embase 500건, Cochrane library 3건, KoreaMed 25건, KISS 27건,
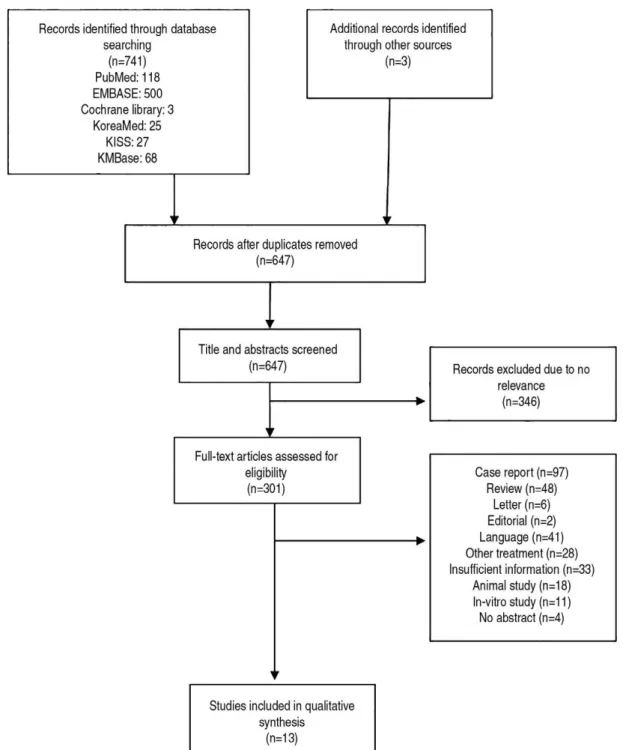
KMbase 68건, 수기 검색으로 추가 3건이 검색되었다. 중 복을 제외하고 제목과 초록을 검토하여 본 연구의 목적과 관련이 없는 문헌을 제외하고 647편을 분석하였다(Fig.
1). 이중 관련 없는 내용을 포함한 301편, 증례보고 97편, 치료 정보가 불충분한 연구 33편, 서신 6편, 사설 2편, 영 문 및 한국어 이외의 언어로 저술된 41편, 다른 치료법을 다룬 28편, 동물 대상 실험 18편, in-vitro study 11편을 제외하고 총 13편을 대상으로 하였다. 논문 형식은 후향
Fig. 1. Flow diagram according to PRISMA format.
적 연구 13편이었다.
2. 논문의 질 평가 결과
SIGN의 질 평가 도구에 의해 후향적 연구에 대하여 질 평가를 시행하였으며, 평가 결과 2++이 2편, 2-가 11편이 었다(Table 2, 3, 4). 문헌의 질 평가 과정은 2명의 연구자 에 의해 수행되었으며, 의견 불일치가 있는 경우는 사전에 검토 원칙을 정하였으나 연구자간 이견은 없었다.
3. 치료 효과의 비교