ISSN 1225-6552, eISSN 2287-7630 https://doi.org/10.7853/kjvs.2018.41.4.281
< Case Report >
Veterinary Service
Available online at http://kjves.org
*Corresponding author: Inchul Park, Tel. +82-33-250-8675, Fax. +82-33-259-5625, E-mail. icpark@kangwon.ac.kr
Situs inversus totalis in a dog with splenic marginal zone lymphoma
Sooyoung Choi
1, Heesu Kim
1, Kija Lee
2, Inchul Park
1*
1
College of Veterinary Medicine, Kangwon National University, Chuncheon 24341, Korea
2
College of Veterinary Medicine, Kyungpook National University, Daegu 41566, Korea (Received 17 September 2018; revised 14 December 2018; accepted 15 December 2018)
Abstract
An 11-year-old intact male mixed-breed dog was referred for evaluation of a splenic mass. On radio- graphs, the cardiac apex, stomach, and head of the spleen were on the right and the descending colon was on the left of the midline. In addition, the left kidney was located more cranially than the right kidney. Standard two-dimensional echocardiographic images were obtained from each inverted left and right parasternal windows. Furthermore, the spleen was observed on the right side and a splenic mass was found on the splenic tail. Based on the radiographic and ultrasonographic characteristics of the pa- tient, a diagnosis of situs inversus totalis (SIT) and a splenic mass was made, and splenic resection was performed successfully with no unexpected complications. The splenic mass was confirmed histopatho- logically as being marginal zone lymphoma (MZL). This report describes a dog with SIT and splenic MZL.
Key words : Dogs, Marginal zone lymphoma, Radiography, Situs inversus totalis, Ultrasonography
INTRODUCTION
Situs inversus totalis (SIT), which is also termed
"situs inversus with dextrocardia," is a rare congenital malformation with complete reversal of organ placement within the body (Piantedosi et al, 2011), and occurs at a rate of 0.01%∼0.02% in humans (Shiraiwa et al, 1995;
Choi et al, 2001; Jerram et al, 2006). Only a few case reports have been published on this condition in rats, mice, dogs, horses, cattle, pigs, and cats (Handel and Kennedy, 1984; Evans, 1987; Shiraiwa et al, 1995; Choi et al, 2001; Buhl et al, 2004; Jerram et al, 2006). SIT is typically found incidentally during imaging proce- dures such as radiography and ultrasonography, and computed tomography (CT) is applied in humans and dogs with SIT to increase the accuracy of diagnosis (Choi et al, 2001; Oui et al, 2013; Wojcik et al, 2013).
In human medicine, tumors from several organs have occasionally been reported in patients with SIT (Suh,
2017). The tumors may indicate surgical intervention, but SIT can make the surgical procedure difficult. This case report describes a dog that was diagnosed with SIT and a splenic tumor based on radiographic and ultra- sonographic characteristics and treated with surgical intervention.
CASE
An 11-year-old, 9.3-kg, intact male, mixed-breed dog with a splenic mass found in a local hospital was re- ferred to the Veterinary Medical Teaching Hospital at Kangwon National University. Traumatic diaphragmatic hernia caused by a traffic accident had been repaired 2 years previously.
On physical examination and blood analysis, no major
abnormalities were observed. Radiography and ultra-
sonography were performed using VXR (DRGEM, Gwang-
myeong, South Korea) and a Toshiba Aplio 400 device
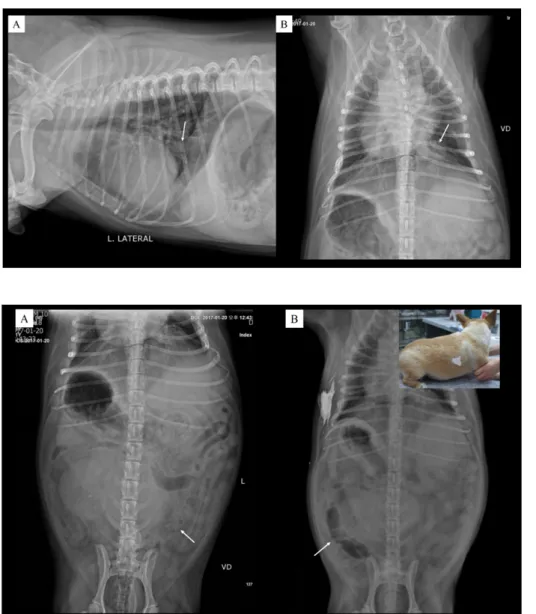
Fig. 2. Ventrodorsal (VD) ab- dominal view showing that the fun- dus of the stomach and the head of the spleen were on the right side of the midline. The right kidney was located more caudally than the left kidney. (A) Radiographs taken at the time of the first visit, showing a left-sided descending colon (arrow). (B) VD radiography was repeated with a radiographic mark- er (barium sulfate) for confir- mation of situs inversus totalis at the second visit for splenectomy.
The descending colon (arrow) was observed on the right-sided abdo- men.
Fig. 1. (A) Ventrodorsalthoracic view revealing dextrocardia and the presence of an oval mass with soft tissue opacity (arrow) on the left diaphragm, which was re- garded to have developed as the result of the diaphragmatic repair.
(B) Left lateral thoracic view re- vealing the caudal vena cava enter- ing the left crus of the diaphragm.
(Toshiba Medical, Otawara, Japan), respectively. Ventro- dorsal (VD) thoracic radiographs revealed a right posi- tion of the cardiac apex and a left position of the car- diac base, suggesting dextrocardia (Fig. 1B). A left lat- eral thoracic image showed the caudal vena cava enter- ing the left crus of the diaphragm (Fig. 1A). In addi- tion, the presence of an oval mass with soft tissue opac- ity was observed on the left diaphragm and was re- garded as an old lesion resulting from the previous trau- matic diaphragmatic hernia. We could not obtain the pa- tient’s medical records from the local hospital at that time. A VD abdominal view showed that the fundus of the stomach and the head of spleen were on the right side of the midline (Fig. 2). The right kidney was lo- cated more caudally than the left kidney. A left-sided
descending colon was observed on radiographs taken at the time of the first visit (Fig. 2A), whereas the de- scending colon was observed on the right side on radio- graphs taken at the second visit for splenectomy (Fig.
2B). VD radiography was repeated with the radiographic marker barium sulfate (Raydix
Ⓡ, Dongindang Pharma- ceutical, Siheung City, South Korea) to confirm a diag- nosis of SIT (Fig. 2B).
Echocardiography was performed for evaluation of
cardiac anomalies. When electrodes were placed in the
routine positions, an inverse electrocardiogram was ob-
tained, and a normal echocardiogram was obtained with
reversal of the electrode placement. Standard 2-dimen-
sional images of 4-chamber long axis and left ventricle
outflow tract views routinely acquired from the right
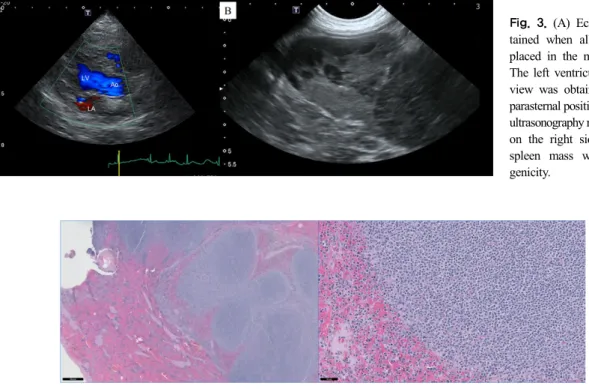
Fig. 3. (A) Echocardiogram ob- tained when all electrodes were placed in the mirrored locations.
The left ventricular outflow track view was obtained from the left parasternal position. (B) Abdominal ultrasonography revealing the spleen on the right side and a solitary spleen mass with mixed echo- genicity.
Fig. 4. Left: White pulp expanding in the spleen and compressing other splenic structures shown as a densely cellular, poorly demarcated, un- encapsulated, expansileround cell neoplasm, composed of lymphoid nodules with an expanded and coalescing marginal zone layer compressing the fading mantle zone layer and germinal centers. Scale bar=500 m. Right: Neoplastic cells with abundant pale cytoplasm and nuclei with peripherali- zation of the chromatin and one prominent nucleolus but without parachromatin clearing. Anisocytosis was mild. Mitotic values were low. Scale bar=50 m.
parasternal window were acquired from the left para- sternal window (Fig. 3A). No cardiac abnormalities were noticed. On abdominal ultrasonographic images, the splenic head was observed on the right-sided ab- dominal cavity, and a solitary splenic mass (maximal di- ameter: 4.7 cm) with mixed echogenicity was observed on the spleen tail (Fig. 3B).
Based on radiographic and ultrasonographic findings, a variant of SIT with the unfixed descending colon and a splenic mass were diagnosed. CT was recommended to obtain more detailed surgical information and de- termine lesional distribution, such as tumoral metastasis related to the splenic mass; however, it could not be performed because of the owner’s refusal.
Splenectomy was performed at the local hospital with the attendance of the authors. The spleen was success- fully found to the right of the abdomen and removed without any unexpected confusion during the operative period. No additional problems were identified in post- operative assessment. The splenic mass was histopatho- logically shown as a densely cellular, poorly demar-
cated, unencapsulated, and expansile round cell neo- plasm composed of lymphoid nodules with an expanded marginal zone layer. Anisocytosis was mild, and mitotic values were low. The splenic mass was confirmed to be marginal zone lymphoma (MZL) (Fig. 4).
DISCUSSION
SIT is a type of situs anomaly (Fulcher and Turner, 2002). The term "situs"refers to the position of the ab- dominal and thoracic organs relative to the midline.
Normal and abnormal positions of organs are termed
"situs solitus" and "situs anomalies," respectively. Situs anomalies has 2 subtypes, one of which is situs in- versus, which can be further divided into situs inversus with dextrocardia or levocardia. The terms "dextrocardia"
and "levocardia" only indicate the direction of the car-
diac apex. Among 11 previously reported canine cases,
9 were SIT and only 2 were situs inversus with levo-
cardia (Carrig et al, 1974; Edwards et al, 1989;
Foodman et al, 1989; Choi et al, 2001; Reichler et al, 2001; Neil et al, 2002; Durant, 2008; Witsberger et al, 2009; Piantedosi et al, 2011; Almeida et al, 2012; Oui et al, 2013). In the present case, reversal of the cardiac apex and gastrointestinal organs was confirmed as being the same as in other dogs with SIT. The midportion of the descending colon has a variety of normal positions in the caudal left abdomen because it is less fixed (Schwart, 2018) and repeated abdominal radiography in the present case showed the descending colon in a vari- ety of positions.
Situs anomalies are sometimes associated withother malformations. SIT is a component of Kartagener’s syn- drome (KS), a disease complex characterized by bron- chiectasis and rhinosinusitis (Kartagener, 1962). Approxi- mately 17% of human beings with SIT and 50% of dogs with SIT are believed to have KS (Mayo and Rice, 1949; Edwards, Kennedy, Patton, et al, 1989). In veterinary medicine, KS has been reported in various breeds of dogs (Carrig et al, 1974; Foodman et al, 1989; Neil et al, 2002; Durant, 2008). In addition, ap- proximately 60% of human patients with situs inversus have other congenital abnormalities of the gastro- intestinal tract (Lee et al, 2006). Based on information obtained from previous canine studies, KS and gastro- intestinal anomalies should be considered as possible complications of SIT. Meanwhile, SIT has been reported as an isolated condition without KS in Doberman pinschers, Cocker spaniels, and mixed-breed dogs (Witsberger et al, 2009; Piantedosi et al, 2011; Almeida et al, 2012). In the present case, KS was not considered because no clinical signs or evidence of bronchiectasis were found on thoracic radiography, and no abnormal- ities of the gastrointestinal tract were observed during abdominal ultrasonographic examination and splenectomy.
The dog in this case was evaluated and considered to have asymptomatic SIT.
In this case, splenic MZL, a lymphoma arising from a particular location within lymphoid follicles, was con- firmed histologically. Splenic MZL is a rare indolent non-Hodgkin lymphoma subtype that originates from B memory lymphocyte, and associated withhepatitis C in human medicine (Santos et al, 2017). MLZ is also rare in veterinary medicine (Stefanello et al, 2011; O'brien et
al, 2013) and no previous report of MZL with SIT exists. In human medicine, previous studies have re- ported SIT with tumors from several organs such as the pancreas, liver, and gastrointestinal track (Suh, 2017).
Although the correlation between tumors and SIT is not well understood, these tumors may play a crucial role in decision making for oncologic surgery. In general, surgi- cal procedures can be difficult because of the widely varying positions of organs in a SIT patient (Blegen, 1949). Thus, recognition of SIT is a valuable step in the preoperative period. Notably, in this case, because a di- agnosis of SIT was made and preparations for unman- ageable problems due to SIT were possible prior to sur- gery, no difficulties were encountered during the splenectomy.
In the present case, although radiography and ultra- sonography enabled the detection of SIT, CT is used to obtain more detailed information (Wojcik et al, 2013) because it provides images of the transverse plane with- out superimposition of structures and can be used to as- sess multiple complex anomalies using reconstructed three-dimensional images (Oui et al, 2013). In several previous canine cases with SIT, CT was used to identify suspicious vessels and hydrocephalus associated with primary ciliary dyskinesia, as well as obtain more ana- tomical details and diagnose bronchiectasis (Neil et al, 2002; Piantedosi et al, 2011; Oui et al, 2013). Hence, CT is highly recommended in dogs with SIT.
In conclusion, the present report documented a dog having asymptomatic SIT with MZL. Although SIT in this dog had no clinical signs, identification of SIT prior to splenectomy with radiography and ultrasonography played a critical role in the success of surgery without unexpected confusion.
ACKNOWLEDGEMENTS
This study was supported by 2017 Research Grant
from Kangwon National University (520170033).
REFERENCES
Almeida G, Almeida M, Freitas L, Santos A, Mattos A. 2012.
Dextrocardia and situs inversus in a dog. Veterinary World 5: 369-372.
Blegen H. 1949. Surgery in situs inversus. Ann Surg 129:
244-259.
Buhl R, Koch J, Agerholm J, Maddox-Hyttel P, Eriksen L. 2004.
Complete situs inversus in a two-year-old standaardbred horse. Vet Rec 154: 600-602.
Carrig C, Suter P, Ewing G, Dungworth D. 1974. Primary dextro- cardia with situs inversus, associated with sinusitis and bronchitis in a dog. J Am Vet Med Assoc 164:
1127-1134.
Choi M, Hwang G, Yoo H, Yoon J, Heo J, Lee K, Chang D.
2001. Radiographic diagnosis—situs inversus of abdomi- nal organs in a dog. Vet Radiol Ultrasound 42: 423-425.
Durant AM. 2008. What is your diagnosis? J Am Vet Med Assoc 232: 197-198.
Edwards D, Kennedy J, Toal R, Maddux J, Barnhill M, Daniel G. 1989. Kartagener's syndrome in a chow chow dog with normal ciliary ultrastructure. Vet Pathol 26:
338-340.
Edwards DF, Kennedy JR, Patton CS, Toal RL, Daniel GB, Lothrop CD. 1989. Familial immotile‐cilia syndrome in English springer spaniel dogs. Am J Med Genet A 33:
290-298.
Evans H. 1987. Cyclopia, situs inversus and widely patent ductus arteriosus in a new-born pig, Sus scrofa. Anat Histol Embryol 16: 221-226.
Foodman M, Giger U, Stebbins K, Knight D. 1989. Kartagener's syndrome in an old miniature poodle. J Small Anim Pract 30: 96-100.
Fulcher AS, Turner MA. 2002. Abdominal manifestations of situs anomalies in adults. Radiographics 22: 1439-1456.
Handel MA, Kennedy JR. 1984. Situs inversus in homozygous mice without immotile cilia. J Hered 75: 498-498.
Jerram RM, Warman CG, Wu CT. 2006. Echocardiographic and radiographic diagnosis: complete situs inversus in a cat.
Vet Radiol Ultrasound 47: 313-315.
Kartagener M. 1962. Bronchiectasis with situs inversus. Arch Pediatr 79: 193-207.
Lee SE, Kim HY, Jung SE, Lee SC, Park KW, Kim WK. 2006.
Situs anomalies and gastrointestinal abnormalities. J Pediatr Surg 41: 1237-1242.
Mayo CW, Rice RG. 1949. Situs inversus totalis: a statistical re- view of data on seventy-six cases with special reference to disease of the biliary tract. Arch Surg 58: 724-730.
Neil JA, Canapp Jr SO, Cook CR, Lattimer JC. 2002.
Kartagener’s syndrome in a Dachshund dog. J Am Anim Hosp Assoc 38: 45-49.
O'brien D, Moore P, Vernau W, Peauroi J, Rebhun R, Rodriguez Jr C, Skorupski K. 2013. Clinical characteristics and out- come in dogs with splenic marginal zone lymphoma. J Vet Intern Med 27: 949-954.
Oui H, Kim J, Bae Y, Oh J, Park S, Lee G, Jeon S, Choi J. 2013.
Computed tomography angiography of situs inversus, portosystemic shunt and multiple vena cava anomalies in a dog. J Vet Med Sci 75: 1525-1528.
Piantedosi D, Cortese L, Meomartino L, Di Loria A, Ciaramella P. 2011. Situs inversus totalis associated with subaortic stenosis, restrictive ventricular septal defect, and tricus- pid dysplasia in an adult dog. Can Vet J 52: 1231-1242.
Reichler I, Hoerauf A, Guscetti F, Gardelle O, Stoffel MH, Jentsch B, Walt H, Arnold S. 2001. Primary ciliary dys- kinesia with situs inversus totalis, hydrocephalus inter- nus and cardiac malformations in a dog. J Small Anim Pract 42: 345-348.
Santos TSd, Tavares RS, Farias DLCd. 2017. Splenic marginal zone lymphoma: a literature review of diagnostic and therapeutic challenges. Rev Bras Hematol Hemoter 39:
146-154.
Schwart T. 2018. Large bowel. pp. 955-969. In: Donal E Thrall(ed.). Textbook of veterinarydiagnostic radiology.
7th. Elsevier. Missouri.
Shiraiwa K, Watanabe A, Sato N, Nito M, Kobayashi Y. 1995.
Case report on situs inversus totalis in two Sprague-Dawley rats. Experimental animals 44: 341-345.
Stefanello D, Valenti P, Zini E, Comazzi S, Gelain M, Roccabianca P, Avallone G, Caniatti M, Marconato L.
2011. Splenic marginal zone lymphoma in 5 dogs (2001- 2008). J Vet Intern Med 25: 90-93.
Suh BJ. 2017. A case of gastric cancer with situs inversus totalis.
Case Rep Oncol 10: 130-135.
Witsberger TH, Dismukes DI, Kelmer EY. 2009. Situs inversus totalis in a dog with a chronic diaphragmatic hernia. J Am Anim Hosp Assoc 45: 245-248.
Wojcik J, Grodzki T, Bielewicz M, Wojtyś M, Kubisa B, Pierog J, Wójcik N. 2013. Lung cancer in situs inversus totalis (SIT)-literature review. Adv Med Sci 58: 1-8.