183
Korean Circulation J 2007;37:183-186
ISSN1738-5520
ⓒ 2007, The Korean Society of Circulation CASE REPORT
A Case of Carney Complex: Diagnosed 11 Years after Resection of Recurrent Cardiac Myxomas
Myung Hwan Bae, MD, Se Yong Jang, MD, Sang Hyuk Lee, MD, Soon Hak Lee, MD, Yongwhi Park, MD, Hun Sik Park, MD, Yongkeun Cho, MD, Shung Chull Chae, MD, Wee Hyun Park, MD, Jae Eun Jun, MD and Dong Heon Yang, MD
Division of Cardiology, Department of Internal Medicine, Kyungpook National University Medical School, Daegu, Korea ABSTRACT
Carney complex (CNC) is a rare disease characterized by myxoma, spotty skin pigmentation, and multiple neuro- endo crine tumors. Here, we present a case of CNC, diagnosed 11 years after resection of recurrent cardiac myxomas.
We had previously reported a 37-year-old woman in 1984 as biatrial myxomas and in 1994 as recurrent left atrial and ventricular myxomas, and at those times, she did not have any other myxomas and skin lesions. On her present admission, she had skin pigmentation and myxomatosis of breast, nostril and forearm. Upon the examination of her relatives, no characteristics of CNC were found on them. She was diagnosed as a sporadic form of CNC. If cardiac myxomas tend to be multiple and recurrent, we should consider the possibility of CNC, even other characteristics of CNC except cardiac myxomas are not present at diagnosis. (Korean Circulation J 2007;37:183-186)
KEY WORDS:Carney complex;Recurrent cardiac myxoma.
Introduction
Carney complex(CNC) is a rare disease characterized mainly by myxomas, spotty skin pigmentations, and multiple neuro-endocrine tumors.1)2) CNC appears to be a familial disease,1) transmitted in an autosomal domi- nant pattern.2) However, sporadic forms of the disease has also been reported.1) Clinical manifestations of CNC may not be fully expressed simultaneously. So CNC may be viewed as a developmental disorder.1) We report a case of CNC, which was in sporadic form, found 11 years after resection of recurrent cardiac myxomas.
Case
A 37-year-old female patient presented with multiple, tender breast masses and intermittent headache. We had previously reported this patient in 1984 as biatrial my- xomas and in 1994 as recurrent left atrial and ventricular myxomas(Fig. 1A, B), and at those times, she did not
have any other extracardiac myxomas and skin lesions.
On her second admission, multiple cerebral aneurysms were noted but aneurysmectomy could not be performed because of patient’s refusal. After the second resection of cardiac myxomas, she did not have medical follow up in our hospital. In 1997, a 5 mm-sized extruding mass was developed on her right forearm and the mass was recurred at the same site shortly after the resection in a local hospital. And then in 2003, a 5 mm-sized extru- ding mass was developed in her right nostril, and from that time, she had suffered from intermittent headache.
On the autumn in 2004, discharges from her left nipple and multiple tender masses in her breasts were developed.
She was referred for further evaluation of these multiple extruding masses and of the current state of previously resected myxomas.
On admission, her vital signs were unremarkable. On physical examination, she had numerous freckles on her lips and perioral skin(Fig. 2). Bean sized soft masses were observed in her right nostril(Fig. 3A) and on her right forearm(Fig. 3B). Various sized tender masses were pal- pated in her breast. Transthoracic and transesophageal echocardiography revealed no residual cardiac myxoma.
Breast MRI showed multiple high signal mass lesions at T2 weighted images.
Pathologic examination of breast lesions showed fib- roadenomas with abundant myxoid components(Fig. 4)
Received:March 12, 2007 Accepted:April 6, 2007
Correspondence:Dong Heon Yang, MD,Departement of Internal Medicine, Kyungpook National University Hospital, #50 Samdeok-2 ga, Jung-gu, Daegu 700-721, Korea
Tel: 82-53-420-5524, Fax: 82-53-426-2046 E-mail: [email protected]
184·Korean Circulation J 2007;37:183-186
but there was no evidence of malignancy. Both MRI and pathologic findings were compatible with myxomas.
Because breast lesions were multiple and numerous, we could not excise them all. Pathologic findings of cuta- neous showed spindle and stellate shaped cells which formed vascular mucinous matrices. These were consis- tent with myxomas. The patient was diagnosed as Carney complex with recurrent cardiac myxomas, cutaneous myxomas, breast myxomatosis and spotty skin pigmen- tations. And then we tried to look for the evidences of neuro-endocrine tumors. IGF-1 and prolactin were sli- ghtly elevated with the values of 573.3 ng/mL(140-400 ng/mL) and 30.21 ng/mL(6-29.9 ng/mL) respectively.
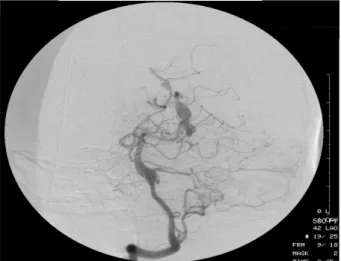
So we performed 75 gm oral glucose tolerance test and pituitary MRI. However, we could not find any evidence of pituitary adenoma. We performed conventional and MR cerebral angiography for the evaluation of previous cerebral aneurysm(Fig. 5). They showed multiple fusi- form dilatations of both middle cerebral arteries, pos- terior cerebral artery and left P2 segment. Aneurysms did not show, however, any impending rupture sign, and the patient strongly refused aneurysmectomy. We decided to make an observation.
Discussion
Carney complex, first described in 1985, is a multiple neoplasia syndrome that is composed of cardiac, endo- crine, cutaneous, and neural tumors, as well as a variety of pigmented lesions of skin and mucosa.1)2) CNC is thought to be a familial disease, inherited in an auto- somal dominant fashion, but some cases have been reported as sporadically occurring or genetically indeter- minate.1) The diagnostic criteria for CNC have been recently reviewed(Table 1).3)4)
Our case was reported in 1984 as biatrial myxomas and in 1994 as recurrent left atrial and ventricular my- xomas, and at those times, she had no other extracar- diac myxomas and skin lesions. However, cutaneous myxomas, breast myxomatosis, and skin pigmentations were developed as time goes by. On the examination of her relatives, any characteristics of CNC could not be found. She was diagnosed as a sporadic form of CNC.
Cardiac myxomas are the most common component of CNC5) and this affect the four chambers of the heart.
Forty one percent of CNC patients have multiple my- xomas while 20% of patients have recurrent myxomas.5) Therefore, for the patients with CNC, if a history of cardiac myxoma is present, screening should be perfor- med every 6 months by echocardiography.6) And if car- diac myxomas tend to be multiple and recurrent, we should consider the possibility of CNC, even other characteristics of CNC were not present at the time of diagnosis.
As is in this case, patients with left atrial myxomas usually present with signs of cardiac failure due to obs- tructed ventricular filling which causes dyspnea, pulmo- nary edema, and right heart failure.7) In at least half of the cases, cerebral arteries are affected, leading to embolic ischemic strokes. In contrast, the formation of intracra- nial aneurysms associated with left atrial myxomas is a less common phenomenon.8)
In the patients with CNC, cutaneous myxomas are presented in 40% of the patients with CNC,5) and com-
A B
Fig. 1. Echocardiographic images of cardiac myxomas. A: Transthoracic echocardiographic image of apical 4 chamber view showed biatrial myxomas in 1984. B: Recurrent Myxomas in LV and LA were noted in transesophageal echocardiography in 1994. LV: left ventricle, LA: left atrium, RA:
right atrium, RV: right ventricle.
Fig. 2. Spotty skin pigmentations were noted on her lips and perioral skin.
Myung Hwan Bae, et al:Clinical Experience of Carney Complex·185
mon sites include eyelids, external ear canals, genital areas and nipples. Breast myxomas, bilateral, are also presented.6)
Clinically evident acromegaly is a relatively infrequent manifestation of CNC. However, asymptomatic elevation
of GH and IGF-I levels, as well as subtle hyperprolacti- nemia, may be present in up to 75% of the patients.9)10) Also, in our patients, although IGF-1 and prolactin levels were slightly elevated, we could not find any evidence of pituitary adenoma on brain MRI.
Only a few cases of CNC have been reported in Ko- rean medical literature.11-15) All of them were compatible with CNC at diagnosis.7)15-17) Our patient was diagnosed as multiple and recurrent cardiac myxomas until her second admission. But 11 years after resection, she was newly diagnosed as CNC by the presentation of cuta- neous myxomas and skin pigmentations at intervals.
Here, we present a rare case of CNC, diagnosed 11 years
Table 1.Diagnostic criteria for Carney complex
01. Spotty skin pigmentation with a typical distribution (lips, conjunctiva and inner or outer canthi, vaginal and penile mucosa)
02. Myxoma (cutaneous and mucosal) 03. Cardiac myxoma
04. Breast myxomatosis or fat suppressed magnetic resonance imaging findings suggestive of this diagnosis
05. PPNAD or paradoxical positive response of urinary glucocorticoids to dexamethasone administration during Liddle’s test
06. Acromegaly due to GH-producing adenoma 07. LCCSCT or characteristic calcification on testicular
ultrasonography
08. Thyroid carcinoma or multiple, hypoechoic nodules on thyroid ultrasonography, in a young patient
09. Psammomatous melanotic schwannoma 10. Blue nevus, epithelioid blue nevus (multiple) 11. Breast ductal adenoma (multiple)
12. Osteochondromyxoma Supplemental criteria:
01. Affected first-degree relative
02. Inactivating mutation of the PRKAR1A gene
To make a diagnosis of Carney complex, a patient must either: 1) ex- hibit two of the manifestations of the disease listed, or 2) exhibit one of these manifestations and meet one of the supplement criteria (an affected first-degree relative or an inactivating mutation of the PR- KAR1A gene). PPNAD: primary pigmented nodular adrenocortical disease, GH: growth hormone, LCCSCT: large cell calcifying sertoli cell tumor
A B
Fig. 3. Bean sized soft masses were observed. A: Right nostril. B: Right forearm.
Fig. 4. Pathologic examination of her breast lesions showed fibroade- nomas with abundant myxoid changes at H & E staining. H & E:
hematoxylin and eosin.
Fig. 5. MR angiogram in 2005 showed multiple fusiform dilatations of middle and posterior cerebral arteries.
186·Korean Circulation J 2007;37:183-186
after resection of recurrent cardiac myxomas.
REFERENCES
1) Stratakis CA, Kirschner LS, Carney JA. Clinical and molecular features of the Carney complex: diagnostic criteria and recom- mendations for patient evaluation. J Clin Endocrinol Metab 2001;
86:4041-6.
2) Carney JA, Hruska LS, Beauchamp GD, Gordon H. Dominant inheritance of the complex of myxomas, spotty pigmentation and endocrine overactivity. Mayo Clin Proc 1986;61:165-72.
3) Stratakis CA, Kirschner LS, Carney JA. Carney complex: diag- nosis and management of the complex of spotty skin pigmentation, myxomas, endocrine overactivity and schwannomas. Am J Med Genet 1998;80:183-5.
4) Stratakis CA, Carney JA, Lin JP, et al. Carney complex, a familial multiple neoplasia and lentiginosis syndrome: analysis of 11 kind- reds and linkage to the short arm of chromosome 2. J Clin Invest 1996;97:699-705.
5) Carney JA. Carney complex: the complex of myxomas, spotty pigmentation, endocrine overactivity, and schwannomas. Semin Dermatol 1995;14:90-8.
6) Bertherat J. Carney complex (CNC). Orphanet J Rare Dis 2006;
1:21.
7) Rhim HY, Youn HJ, Park JW, et al. Clinical experience of cardiac myxoma. Korean Circ J 1999;29:1317-23.
8) Chen HJ, Liou CW, Chen L. Metastatic atrial myxoma presenting
as intracranial aneurysms with hemorrhage: case report. Surg Neurol 1993;40:61-4.
9) Watson JC, Stratakis CA, Bryant-Greenwood PK, et al. Neurosur- gical implications of Carney complex. J Neurosurg 2000;92:
413-8.
10) Pack SD, Kirschner LS, Pak E, Zhuang Z, Carney JA, Stratakis CA. Genetic and histologic studies of somatomammotropic pitui- tary tumors in patients with the “complex of spotty skin pigmen- tation, myxomas, endocrine overactivity and schwannomas” (Car- ney complex). J Clin Endocrinol Metab 2000;85:3860-5.
11) Park HR, Kim EA, Jiang MH, et al. A case of isolated familial somatotropinoma. J Korean Soc Endocrinol 2004;19:398-405.
12) Park JY, Yoo HD, Kim NI. Carney’s complex with familial atrial myxoma. Korean J Dermatol 1998;36:942-5.
13) Kim MC, Lee JY, Park CC, Young YS, Cho KS. Familial atrial myxoma with Carney’s complex: 1 case. Korean J Thorac Car- diovasc Surg 1998;31:816-9.
14) Yoo SJ, Cha BY, Lee KW, et al. A case of Cushing’s syndrome due to primary pimary pigmented nodular adrenal dysplasia (PP- NAD): a case of Carney’s complex. J Korean Soc Endocrinol 1997;12:90-8.
15) Lee RT, Choung BY, Kwon SH, et al. A case of Carney complex in Korea. J Korean Soc Endocrinol 1997;12:633-41.
16) Kim GG, Kang HS, Lee GW. A case of complex cardiac myxoma combined with nipple myxoma. Korean Circ J 1998;28:453-7.
17) Yoon HD, Shon HS. A typical Korean case of Carney complex.
Korean J Intern Med 2003;18:260-5.