슬관절 전 치환술시의 출혈 양 및 수혈 양 감소를 위한 Ap ro t i n i n 의 효과
울산대학교 의과대학 강릉아산병원 정형외과학교실, 성균관대학교 의과대학 강북삼성병원 정형외과학교실*
최영준・황재광・안형선・배의정・김정환・김유진*
= 국문초록=
목 적: 슬관절 전 치환술 시 Aprotinin 투여에 따른 수술 후 출혈 양과 수혈 양 감소에의 효과를 연구하 였다.
대상 및 방법: 양측 슬관절 전 치환술을 동시에 시행 받은 환자 1 0 0명을 대상으로 하였다. 투여군 5 0명은 지혈대 사용 직전 A p r o t i n i n을 저용량 용법에 따라 주사하였고, 비투여군 5 0명은 A p r o t i n i n을 투여하지 않은 대조군이었다. 술 후 출혈 양, 술 중 및 술 후 수혈 양을 측정하였다. 술 전 및 술 후 시간 경과별 혈 색소 및 적혈구 용적을 측정하였고, Aprotinin 투여 후 합병증에 대해서도 조사하였다.
결 과: 투여군과 비투여군에서 수술 후 총 출혈 양은 각각 평균 1197 ml, 2215 ml로 유의한 차이를 보였 다. 평균 총 수혈양은 두 군에서 각각 농축 적혈구가 2 . 0단위 및 4 . 0단위, 신선 냉동 혈장이 0 . 1단위 및 1 . 2단위로 유의한 차이를 보였다. 혈색소 및 적혈구 용적치는 술 후 1일, 2일, 4일에 유의한 차이가 있었 고, 모든 환자에서 과민성 쇼크, 심부 정맥 혈전증, 혈색전증, 협심증, 급성 신부전등의 합병증을 보인 예는 없었다.
결 론: 슬관절 전 치환술 시 A p r o t i n i n의 투여는 수술 후 총 혈액 손실과 수혈 양을 감소시키는데 효과가 있으며, 합병증 면에서 안전한 것으로 사료되었다.
색인 단어: 슬관절 전 치환술, Aprotinin, 출혈 양, 수혈 양
Volume 17, Number 2, December 2005
서 론
대부분의 슬관절 전 치환술에 있어서 어느 정도의 출혈과 그에 따른 수혈이 요구되고 있으나, 수혈의 안전성 문제가 제기되면서 출혈 및 수혈을 줄일 수 있는 방법에 대한 관심도가 높아지고 있다. 출혈을 보충하기 위하여 술 전 자가수혈2 , 5 , 1 2 )
, 정상 혈량 혈
액희석2 0 )과 같은 혈액 보존 요법과, 저혈압 마취20) 등
이 수혈의 부작용을 줄이기 위해 시도되고 있으나, 수혈 양 감소에의 효용성은 아직 미지수이며, cell
saver 등의 보존 요법은 비용과 시설 등에 대한 제 한점이 있다2 ). 최근 흉부외과 수술과 간 수술 등에서 A p r o t i n i n의 사용에 따른 출혈 양 및 수혈 양 감소 에 대해서 연구가 이루어져 왔으며4 , 1 6 , 1 9 ), 현재까지 정형외과 영역에서는 고관절 전 치환술, 슬관절 전 치환술 및 척추 수술등에서 A p r o t i n i n의 효용성에 대해 보고된 바 있다3 , 7 - 9 , 1 0 , 1 7 , 1 8 ). 본 연구에서는 양측 슬관절 전 치환술을 동시에 시행 받은 환자에서 A p r o t i n i n을 투여 한 후 그 결과를 투여하지 않은 대조군과 비교하여 수술 후 출혈 양 및 수혈 양의 감 소 여부와 현재까지 보고된 Aprotinin 투여 후의 부
Corresponding Author: Jae Kwang Hwang, M.D.
Department of Orthopedic Surgery, Gangneung Asan Hospital,
415, Bangdong-Ri, Sacheon-Myon, Gangneung, Gangwon-Do 210-711, Korea
작용 발현 여부3 , 7 , 8 , 1 5 )를 조사하여 그 효과와 안전성에 대해 고찰해 보고자 한다.
대상 및 방법
2 0 0 2년 9월부터 2 0 0 4년 7월까지 한 명의 술 자에 의하여 양측 슬관절 전 치환술을 시행 받은 퇴행성 골 관절염 환자1 0 0명을 대상으로 하였으며, Apro- t i n i n의 투약 여부에 따라 환자를 두 군으로 나누었 다. 투여군( N = 5 0 )의 환자들은 지혈대 사용직전 초기 용량 Aprotinin 1.000.000 kalikrein inhibiting u n i t s ( K I U )단위를 2 0 ~ 3 0분간 주사 후 2 4시간 동 안 시간당 2 0 0 . 0 0 0 K I U의 유지 용량 주사를 시행하 였으며 비투여군( N = 5 0 )의 환자들은 Aprotinin 투 여 없이 수술을 진행하였다. 대상 환자 중 수술 전에 시행한 혈액 응고 검사에서 이상을 보인 예는 없었으 며 두 군간에 성별, 연령, 수술 시간 및 재원 일수 등에서는 통계적으로 유의한 차이는 없었다.
모든 환자에서 NexGen, LPS-FlexⓇ p r o s t h e s i s (Zimmer, Warsaw, IN)를 사용하였으며, 동일한 방법으로 시행되었다. 수술 중 수혈은 모든 예에서 동일한 마취과 의사의 판단에 따라 시행하였고, 수술 후에는 농축 적혈구( P R B C )를 혈색소 수치( H e m o- g l o b i n )가 8 . 0 g / d l미만, 또는 적혈구 용적 측정치 ( H e m a t o c r i t )가 2 4 %미만인 경우에 수혈하였다. 수
술 직 후 모든 환자에서 슬관절 운동을 허용하였으 며, 수술 전 후에 혈액 응고 능력을 변화 시킬 수 있 는 약은 투여하지 않았다. 술 후 출혈 양은 두 개의 흡입 배액관을 이용하여 측정하였으며, 24시간 동안 누적 배액이 200 ml 이하인 경우에는 술 후 2일째 에 배액관을 제거하였으나 그 이상의 배액이 있는 경 우(투여군 1 0례, 대조군 9례)에는 술 후 3일에 배액 관을 제거하였다. 술 전 혈색소 및 적혈구 용적을 측 정하였으며, 술 후 혈액 검사는 수술 2시간 후와 술 후 1일, 2일, 4일, 7일에 측정하여 비교하였다. 입 원 기간 중에 현재까지 보고된Aprotinin 투여에 의 한 약물성 과민성 쇼크, 심부 정맥 혈전증, 혈색전 증, 협심증, 급성 신부전증 등의 합병증의 발현에 대 해서도 조사하였다3 , 7 , 8 , 1 4 , 1 5 ). 결과 분석은 SPSS for Windows 11.5Ⓡ를 이용하여 S t u d e n t’s t-test를 통해 시행하였으며, 유의수준 0 . 0 5이하를 통계학적 의의가 있다고 설정하였다.
결 과
평균 출혈 양은 투여군에서 수술 후 당일과 총 평 균 출혈 양에서 통계적으로 유의한 차이를 보였고 (p=0.000), 술 후 2일에는 투여군에서 출혈양이 증 가한 결과를 보였으나 통계적 유의성은 없었으며 (p=0.051) 술 후 3일째의 출혈양은 두 군간에 유의
Table 1. Post-operative blood loss (ml)
Aprotinin group Control group p-value
POD* 1 0544±237.7† 1766±532.00‡ 0.000
POD* 2 0459±200.9† 0381±175.00‡ 0.051
POD* 3 0350±143.9† 0374±107.0‡0 0.064
Total blood loss 1195±840.9† 2215±671.36‡ 0.000
Results are expressed as mean±standard deviation (SD) unless noted otherwise.
* Post-operative day
†Number of patients=10
‡Number of patients =9
Table 2. Mean amount of blood cell transfusion (units)
Aprotinin group Control group p-value
P-RBC* FFP† P-RBC* FFP† P-RBC*/FFP†
Intra-operative 2.0±0.59 00.1±0.05 2.9±1.20 1.2±1.4 0.000/0.000
Post-operative 0.2±0.55 0.02±0.14 1.1±1.20 0.00 0.000/0.310
Total 2.2±0.87 00.1±0.47 4.0±1.12 1.2±1.4 0.000/0.000
Results are expressed as mean±SD unless otherwise noted.
* Packed red blood cell
†Fresh frozen plasma
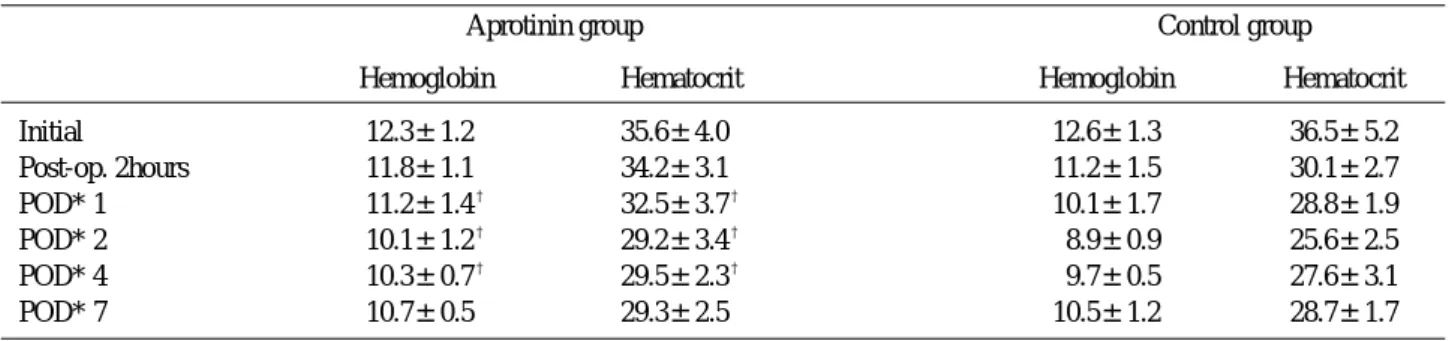
한 차이가 없었다(p=0.064)(Table 1). 수술 중 평 균 수혈 양과 총 평균 수혈 양은 투여군에서 농축 적 혈구와 신선 냉동 혈장 모두 통계적으로 유의한 차이 의 감소를 보였으며(Table 2), 술 후 농축 적혈구 수혈을 시행 받은 환자는 투여군에서 7예(14%), 비 투여군에서 2 5예( 5 0 % )였으며, 수혈 양에서도 통계 적으로 유의한 차이를 보였고, 투여군 중 2예( 4 % )에 서는 수혈 없이 수술을 진행하였다. 술 전 혈색소와 적혈구 용적 측정치는 두 군간에 유의한 차이가 없었 으며, 술 후 1일, 2일 및 4일의 결과에서는 통계적 으로 유의한 차이를 보였다(Table 3).
A p r o t i n i n을 투여한 모든 환자에서 입원 기간 중 약물성 과민성 쇼크, 심부 정맥 혈전증, 혈색전증, 협심증, 급성 신부전증 등과 같은 합병증의 임상적 증상을 보인 예는 없었다.
고 찰
A p r o t i n i n은 소의 폐에서 분리된 5 8개의 아미노 산으로 구성된 serine protease inhibitor로서 Kunitz 등1 3 )에 의해 처음으로 보고된 트립신, 키모 트립신, 플라스민, 칼리크레인 등의 억제제이며, 그 작용기전은 칼리크레인과 플라스민의 작용을 직접 방 해하여 섬유소 용해를 억제 하고, 플라스민의 작용을 억제함으로써 혈소판의 Glycoprotein (GP) Ib 수 용기의 분해를 방지하고, GPIIb-IIIa 수용기 기능을 보존함으로써, 혈소판 유착성을 유지시켜 혈소판 응 집과 그 기능을 보호하는 것으로 알려져 있다1 , 6 , 1 1 ). Murkin 등1 8 )은 인공 고관절 전 치환술 시 A p r o- t i n i n을 투여함으로써, 출혈 양 및 수혈 양을 현저히 줄일 수 있었고, 초기 용량 2,000,000 KIU의 고용 량 용법과 1,000,000 KIU의 저용량 용법에서 모두 비슷한 결과를 보고하였다. Capdevila 등3 )은 외상, 종양, 척추 수술 등의 정형외과 영역에서 A p r o t i n i n
을 투여하여, 출혈 양을 4 0 %이상, 수혈 양을 5 0 % 이상 줄일 수 있었다. 최근에는 Jeserschek 등9 )이 슬관절 및 고관절 재치환술에서 Aprotinin 투여가 부작용의 발현 없이 수술 중 및 술 후 출혈 양과 수 혈 양의 감소에 효용성이 있음을 보고한 바 있다. 본 연구에서는 슬관절 전 치환 술에서 Aprotinin 투여 시 술 후 출혈 및 수혈 양이 현저히 감소하는 결과를 보였다. 특히 술 후 총 평균 출혈양은 비투여 군과 비교하여 4 5 %이상 감소하였으며, 술 중 농축 적혈 구 수혈 양과 총 평균 농축 적혈구 수혈 양도 1 . 5단 위 이상 줄일 수 있었다. 술 후 혈색소와 적혈구 용 적의 변화는 술 후 1일, 2일, 4일에 통계적으로 유 의한 차이를 보여 이 시기의 수혈을 줄일 수 있었던 것으로 사료되었으며, 수술 종료 2시간 후의 측정치 는 수술 중의 출혈과 연관된 수혈 양의 차이로 인해 두 군에서 거의 비슷한 결과를 보인 것으로 생각되었 다.
현재까지 A p r o t i n i n투여 후의 합병증에 대해서는 많은 조사가 이루어졌다. 여러 연구에서 A p r o t i n i n 투여 후의 심부 정맥 혈전증과 혈색전증의 발현 여부 에 대해 보고되었고3 , 8 ), Lemmer 등1 5 )은 A p r o t i n i n 투여 후 혈청 크레아티닌(creatinine) 수치가 증가 되는 결과를 보고하였으며, Laupacis와 F u r g u s- s o n1 4 )의 연구에서는 협심증 발현의 증가가 보고되기 도 하였다. 그러나 최근의 연구에서는 A p r o t i n i n의 투여 후 심부 정맥 혈전증 등의 합병증의 발현이 대 조 군과 비교하여 차이가 없는 것으로 나타나고 있으 며3,18), 이러한 결과는 Hayes 등7 )의 연구에서도 확인 된 바 있다. Janssens 등8 )과 Murkin 등1 8 )은 심부 정맥 혈전증의 발현 빈도가 비투여 군에서 오히 려 높은 것으로 보고하였다. 본 연구에서는 술 후 정 맥 조영술이나 도플러 초음파 등을 통한 심부 정맥 혈전증에 대한 검사는 시행하지 않아 정확한 발생 빈 도를 알 수 없었으나, 그 외 약물성 과민 반응, 혈색
Table 3. Initial & postoperative mean hemoglobin (g/dl) & hematocrit (%)
Aprotinin group Control group
Hemoglobin Hematocrit Hemoglobin Hematocrit
Initial 12.3±1.2† 35.6±4.0† 12.6±1.3 36.5±5.2
Post-op. 2hours 11.8±1.1† 34.2±3.1† 11.2±1.5 30.1±2.7
POD* 1 11.2±1.4† 32.5±3.7† 10.1±1.7 28.8±1.9
POD* 2 10.1±1.2† 29.2±3.4† 08.9±0.9 25.6±2.5
POD* 4 10.3±0.7† 29.5±2.3† 09.7±0.5 27.6±3.1
POD* 7 10.7±0.5† 29.3±2.5† 10.5±1.2 28.7±1.7
전증, 협심증, 급성 신부전등의 합병증이 발생한 예 는 없었다.
저자들은 슬관절 전 치환 술 시 A p r o t i n i n을 투여 하여 술 후 출혈 양 및 수혈 양 감소에 있어 만족할 만한 결과를 얻을 수 있었다. 그러나 현재 국내의 경 우 A p r o t i n i n의 투여 비용이 술 후 출혈 및 수혈 양 감소에 의한 의료비용 절감에 비해 과다하다는 점이 약물투여의 제한점으로 생각되어, 이러한 점이 보완 된다면 슬관절 전치환술 시에 A p r o t i n i n을 투여함 으로써 출혈과 수혈의 문제점을 효과적으로 줄일 수 있을 것으로 사료되었다.
결 론
슬관절 전 치환술 시의 A p r o t i n i n의 투여는 수술 후 총 혈액 손실과 수혈 양을 감소시키는데 효과가 있으며, 합병증 면에서 안전한 것으로 사료되었다.
REFERENCES
01) Allison PM and Whitten CW: What is mechanism of action of aprotinin? Anesthesiology, 73B:377-379, 1991.
02) Bottner F, Pavone V, Johnson T, Heitkemper S and Sculco TP: Blood management after bilateral total knee arthroplasty. Clin Orthop, 410:254-261, 2003.
03) Capdevila X, Calvet Y, Biboulet P, Biron C, Rubenovitch J and d’Athis F: Aprotinin decreases blood loss and homologous transfusion in patients undergoing major orthopedic surgery. Anesthesiolo - gy, 88:50-57, 1998.
04) Cicek S, Demirkilic U, Ozal E, et al: Postoperative use of aprotinin in cardiac operations. An alternative to its prophylactic use. J Thorac Cardiovasc Surg, 112:1462-1467, 1996.
05) Couvret C, Laffon M, Baud A, Payen V, Burdin P and Fusciardi J: A restrictive use of both autolo- gous donation and recombinant human erythropoi- etin is an efficient policy for primary total hip or knee arthroplasty. Anesth Analg, 99:262-271, 2004.
06) Davis R and Whittinton R: Aprotinin. A review of its pharmacology and therapeutic efficacy in reduc- ing blood loss associated cardiac surgery. D r u g s, 49:984-1006, 1995.
07) Hayes A, Murphy DB and McCarroll M: The effi-
cacy of single dose aprotinin 2 million KIU in reduc- ing blood loss and its impact on incidence of deep venous thrombosis, in patients undergoing total hip replacement surgery. J Clin Anesth, 8:357-360, 1996.
08) Janssens M, Joris J, David JL, Lemaire R and Lamy M: High dose aprotinin reduces blood loss in patients undergoing total hip replacement surgery.
Anesthesiology, 80:23-29, 1994.
09) Jeserschek R, Clar H, Aigner C, Rehak P, Primus B and Windhager R: Reduction of blood loss using high-dose aprotinin in major orthopaedic surgery. A prospective, double blind, randomized and placebo controlled study. J Bone Joint Surg, 85-B:174-177, 2003.
10) Kasper SM, Elsner F, Hilgers D, Grond S and R u ¨ tt J : A retrospective study of the effects of small- dose aprotinin on blood loss and transfusion needs during total hip arthroplasty. Eur J Anesthesiology, 15:669-675, 1998.
11) Kozek-Langenenecker SA, Mohammad SF, Masaki T, Green W, Kamerath C and Cheung A K: The effects of aprotinin on platelet in vitro using whole blood cytometry. Anesth Analg, 90:12- 16, 2000.
12) Kourtzis N, Pafilas D and Kasimatis G: Blood saving protocol in elective total knee arthroplasty.
Am J Surg, 187:261-267, 2004.
13) Kunitz M and Northrop JH: Isolation from beef pancreas of crystalline trypsinogen, a trypsin inhibitor and intibulartrypsin compound. J Gen Physiol, 19:911-1007, 1936.
14) Laupacis A and Fugersson D: Drugs to minimize perioperative blood loss in cardiac surgery. Meta- analysis using perioperative blood transfusion as the outcome. The International Study of Peri-operative Transfusion (ISPOT) Investigators. Anesth Analg, 85:1258-1267, 1997.
15) Lemmer JH, Stanford W, Bonney SL, et al: Apro- tinin for coronary artery bypass grafting. Effect on postoperative renal function. Ann Thorac Surg, 59(1):132-136, 1995.
16) Lentschener C, Benhamou D, Mercier JF, et al:
Aprotinin reduces blood loss in patients undergoing elective liver resection. Anesth Analg, 84:875-881, 1997.
17) Lentschener C, Cottin P, Bouaziz H, et al: Reduc- tion of blood loss and transfusion requirement by aprotinin in posterior lumbar spine fusion. A n e s t h Analg, 89:590-597, 1999.
18) Murkin JM, Haig GM, Beer KJ, et al: Aprotinin decreases exposure to allogenic blood during prima- ry unilateral total hip replacement. J Bone Joint
Surg, 82-A:675-684, 2000.
19) Royston D : High dose aprotinin therapy. A review of the first five years’experience. J Cardiothoracic Vasc Anesth, 6(1):76-100, 1992.
20) Tenholder M and Cushner FD : Intraoperative blood management in joint replacement surgery.
Orthopedics, 27(6 Suppl):663-668, 2004.
─ Abstract ─
The Effect of Aprotinin for Reducing Blood Loss and Amount of Transfusion in Total Knee Arthroplasty
Young Joon Choi, M.D., Jae Kwang Hwang, M.D., Hyung Sun Ahn, M.D., Eui Jung Bae, M.D., Chung Hwan Kim, M.D., Eugene Kim, M.D.*
Department of Orthopedic Surgery, Gangneung Asan Hospital, Gangneung, Gangwon-Do, Korea, Department of Orthopaedic Surgery, Kangbuk Samsung Hospital,
Sungkyunkwan University School of Medicine,Seoul, Republic of Korea*
Purpose: To evaluate the effect of Aprotinin in reducing postoperative blood loss and amount of trans- fusion in total knee arthroplasty.
Materials and Methods: In a prospective study, 100 patients undergoing bilateral total knee arthro- plasty were investigated. A low dose Aprotinin was administred in randomly selected fifty patients and the other fifty patients were selected as control group. Postoperative blood loss, the amount of intraopera- tive and postoperative transfusion, preoperative and postoperative value of hemoglobin and hematocrit were evaluated and statiscally compared. Postoperative complications were assessed.
Results: Significant reduction in postoperative total blood loss was observed (Aprotinin group:1195 ml, control group:2216 ml). The amount of packed red blood cells transfusion was also reduced in Aprotinin group (Aprotinin group: 2.0 units, control group: 4.0 units), and fresh frozen plasma (Aprotinin group:
0.1units, control group: 1.2 units) as well. Aprotinin also reduced the decline in hemoglobin and hemat- ocrit levels at the first, second and fourth postoperative days. There were no clinical evidence of compli- cations such as anaphylactic shock, deep vein thrombosis, thromboembolism, myocardiac infarction and acute renal failure.
Conclusion: Aprotinin is safe and effective in reducing postoperative blood loss and amount of blood transfusion in total knee arthroplasty.
Key Words: Total knee arthroplasty, Aprotinin, Postoperative blood loss and transfusion