대한소화기학회지 2004;44:193~198
INTRODUCTION
1)Although several studies have claimed the relationship between Helicobacter pylori (H. pylori) infection and cardio-
접수: 2004년 5월 3일, 승인: 2004년 7월 16일 연락처: 손희정, 135-710, 서울시 강남구 일원동 50
삼성서울병원 소화기내과
Tel: (02) 3410-3409, Fax: (02) 3410-3849 E-mail: [email protected]
vascular disease, it is still unclear whether an active H. pylori (H. pylori) infection is clinically involved in the initiation or development of coronary heart disease (CHD).1-92) Further- more, association of H. pylori infection with the acute
Correspondence to: Hee Jung Son, M.D.
Department of Medicine, Samsung Medical Center 50 Irwon-dong, Gangnam-gu, Seoul 135-710, Korea Tel: +82-2-3410-3409, Fax: +82-2-3410-3849 E-mail: [email protected]
한국인에서 헬리코박터 감염이 심혈관 질환에 미치는 영향
성균관대학교 의과대학 내과학교실
이선영․김덕경․손희정․이준행․김영호․김재준․백승운․이종철
The Impact of Helicobacter pylori Infection on Coronary Heart Disease in a Korean Population
Sun-Young Lee, M.D., Duk-Kyung Kim, M.D., Hee Jung Son, M.D., Jun Haeng Lee, M.D., Young-Ho Kim, M.D., Jae J. Kim, M.D., Seung Woon Paik, M.D., and Jong Chul Rhee, M.D.
Department of Internal Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea
Background/Aims: Although several studies have claimed that Helicobacter pylori (H. pylori) infection is related to cardiovascular disease, it is still uncertain whether it is related to the acute process or the chronic inflammatory atherosclerotic changes. The aim of our study was to confirm the impact of active H. pylori infection on coronary heart disease, acute inflammatory factors, and the coagulation factors. Methods: A total of 94 patients completed questionnaires about occupation, smoking, past medical history, and socio-economic status. The serum of the subjects was drawn for a low density lipoprotein test, white blood cell count, C reactive protein, fibrinogen, homocysteine, prothrombin time, activated partial thrombin time, plasminogen activator inhibitor type-1, and tissue-type plasminogen test. All of the subjects underwent a coronary angiography and an upper gastrointestinal endoscopy for the diagnosis of coronary heart disease and H. pylori infection, respectively. Results: There was no significant difference in acute inflammatory factors, coagulation factors, atheromatous burden score, and Jeopardy score between the H. pylori-infected group and non-infected group. Odds ratio of H. pylori infection on coronary heart disease was 2.59 (95% CI, 0.80-6.17), but it diminished below 1.0 (95% CI, 0.14-1.36) after adjusting for conventional risk factors such as age, gender, diabetes, hypertension, smoking, body mass index and socio-economic status. Conclusions: H. pylori infection is not an independent risk factor for coronary heart disease, and it does not alter the coagulation system or evoke the systemic inflammatory response. (Korean J Gastroenterol 2004;44:193-198)
Key Words: Helicobacter pylori; Coronary heart disease; Risk factors
대한소화기학회지: 제44권 제4호, 2004 194
process of CHD or the chronic inflammatory atherosclerotic changes also needs to be clarified. Such ambiguities come from the evaluation method to determine H. pylori infection status by measuring merely the titer of the serum antibody.
Additionally, H. pylori seropositivity can not discriminate a current infection from a previous one. Anti-H. pylori IgG is not a reliable marker for an active H. pylori infection, because the antibody titer can not distinguish active infection from past infection. Moreover, it is relatively inferior to the diagnostic biopsy in accuracy, sensitivity, and specificity.10
Recently, some studies reported that H. pylori infection is not implicated as early etiologic triggers in the genesis of CHD.11,12 They suggested that H. pylori is not associated with acceleration of existing atherosclerosis and acute plaque rupture. Previous studies have accessed CHD with variable criteria such as abnormality of electrocardiogram (EKG), World Health Organization (WHO) criteria, clinical diagnosis of angina or acute myocardial infarction, and death due to cardiovascular disease.1-9 In our study, we tried to confirm the impact of an active H. pylori infection on CHD by stomach biopsy and coronary angiography. We also evaluated the conventional factors related to cardiovascular risk factors, acute inflammation, and coagulation factors.
MATERIALS and METHODS
1. Patients
We selected 94 patients who underwent coronary angiography due to chest pain from April 2001 to June 2002 in Samsung Medical Center, Seoul, Korea, retrospectively.
All of the patients received an upper gastrointestinal endoscopy for the diagnosis of H. pylori within two months of the interval from their coronary angiography. None of them received antibiotic therapy during this period. The patients were provided informed consent before the exami- nation.
The subjects completed a questionnaire about occupation, cigarette smoking, and past medical history including diabetes and hypertension. We assessed body mass index (BMI) and socio-economic status (SES) by the index of Hollingshead.13 The serum of the subjects was analyzed for low density lipoprotein (LDL), white blood cell count (WBC), C reactive protein (CRP), fibrinogen, homocysteine,
prothrombin time (PT), activated partial thrombin time (aPTT), plasminogen activator inhibitor type-1 (PAI-1), and tissue-type plasminogen (tPA).
2. Cardiovascular assessment
All of the patients were examined by coronary angio- graphy for the firm diagnosis of CHD. They were diagnosed as significant coronary artery stenosis when more than 30%
of luminal narrowing was observed. Based on coronary angiography, the patients were classified into the CHD and the control group.
The Jeopardy score was calculated by dividing the coronary tree into 6 segments: the left anterior descending artery (LAD), diagonal branches of LAD, septal perforating branches, left circumflex coronary artery (LCx), obtuse marginal branches, and the posterior descending coronary artery.14 This score encompassed the total region of jeopardized myocardium supplied by a target vessel and the supplying collaterals to other heart regions. The score also contained the degree of baseline left ventricular dysfunction.
The Jeopardy scoring system is composed of three items.
One point is given for each myocardial region supplied by a target region, 1 point for each myocardial region supplied by a vessel with diameter stenosis more than 70%, and 0.5 point is given for each myocardial region that is hypokinetic at the baseline and it is not supplied by a vessel with significant stenosis.
The atheromatous burden score was calculated for the accurate measurement of atherosclerotic changes in the 3 major coronary arteries. We define the score 0 as no luminal abnormality, which means completely normal artery.
The score 1 means a stenosis less than 30%. Luminal irregularities and hypoplastic arteries were measured as 1 in this scoring system because these conditions might represent the minimal atherosclerotic changes. Stenosis between 30%
and 50% to total occlusion was defined as score 2, that between 50% and 70% as score 3, and that exceeding 70%
as score 4. The left main coronary artery was assigned as a double score, more than the major 3 coronary arteries, because it represents the sum of the LAD and LCx. For example, if the left main coronary artery was totally occluded, it was scored as 8. Each major coronary artery (LAD, LCx, RCA) was scored from 0 to 4, and thus, the maximal possible number of points was 12.
이선영 외 7인. 헬리코박터 감염과 심혈관 질환 195
3. Histological assessment
All of the subjects underwent upper gastrointestinal endoscopy to confirm H.
pylori infection. Each gastric biopsy was obtained from the antrum and body separately. The specimens were fixed in 10% formalin and then embedded with paraffin. The sections were stained by hematoxylin & eosin and Giemsa for the laboratory assessment. To prevent inter- personal variation, one experienced pathol- ogist examined all the biopsied specimens.
The specimens were examined for H. pylori colonization, neutrophil activity, mononu- clear cells, atrophy, and intestinal meta- plasia. The results were finally reported using the criteria of the updated Sydney system.
4. Statistical analyses
A p value less than 0.05 was considered significant. Differences between the H.
pylori-infected group and the non-infected
group were assessed by chi-square test and t-test. A logistic regression analysis was made to adjust the other cardiovascular risk factors such as age, gender, diabetes, hypertension, smoking, BMI, and SES. The association between H. pylori infection and CHD was estimated by odds ratio.
RESULTS
1. The basal characteristics of the patients with or without H. pylori infection
Between the H. pylori-infected group and non-infected group, there was no significant difference in age, gender, BMI, SES, proportion of patients with diabetes and hypertension, and the proportion of smokers (Table 1). The mean values of LDL, WBC, CRP, fibrinogen, homocysteine, PT, aPTT, PAI-1, and tPA showed no significant difference between the two groups (Table 1).
2. The result of coronary angiography
Among 94 patients, 54 patients had a significant coronary artery stenosis showing more than 30% of luminal narrowing. A total of 25 patients were diagnosed as one vessel disease, 10 patients as two vessels disease, and 19 patients as three vessels disease. CHD was observed in 41 patients (65.6%) among 61 of H. pylori-infected group and 15 (42.4%) among 33 of non-infected group (p=0.03).
Jeopardy score was 1.06±1.36 in H. pylori-infected group and 1.08±1.76 in non-infected group (p=0.96). The atheromatous burden score revealed that a normal coronary finding is more frequently observed in the non-infected patients than in the H. pylori-infected ones (Fig. 1).
Comparing the number of the narrowed major coronary arteries between the H. pylori-infected group and non- infected group, the proportion of the patients seemed to be higher in infected group than in non-infected group though it was not statistically significant (Fig. 2).
3. The relationship between CHD and risk factors including H. pylori infection
We selected several different patient groups inside our Table 1. Clinical Characteristics of Patients
Helicobacter pylori
p value Positive
(n=61)
Negative (n=33) Mean age
Gender (M/F) Diabetes (%) Hypertension (%) Smoking (%) SES (level) LDL (mg/dL) WBC (/mm3) CRP (mg/dL) Fibrinogen (mg/dL) Homocysteine (mg/dL) PT (sec)
aPTT (sec) PAI-1 (ng/mL) tPA (ng/mL)
59.9±8.9 43/18
27.9 41.0 37.7 2.5±1.4 126.9±49.3 6,657.9±1,857.8
1.6±3.2 392.2±126.5
13.2±3.2 13.1±0.9 37.6±7.4 35.3±23.1
9.4±4.9
58.2±9.6 24/9 21.2 33.3 42.4 3.0±1.4 114.8±34.7 7,219.7±2,694.9
1.3±2.2 402.0±140.4
14.0±6.2 13.5±1.4 39.2±8.2 39.6±24.4
9.3±4.5
NS NS NS NS NS NS NS NS NS NS NS NS NS NS NS Mean±SD; NS, not significant; SES, socioeconomic status; LDL, low density lipoprotein; WBC, white blood cell; CRP, C reactive protein; PT, prothrombin time; aPTT, activated partial thrombin time; PAI-1, platelet plasminogen activator inhibitor type-1; tPA, tissue-type plasminogen.
SES13: 1 indicates the highest; 5 indicates the lowest.
The Korean Journal of Gastroenterology: Vol. 44, No. 4, 2004 196
Fig. 1. Atheromatous burden score in the H. pylori-infected group and non-infected group. Normal coronary finding was more frequently observed in the non-infected group than the H. pylori- infected group, but it was not statistically significant.
Fig. 2. Number of the narrowed major coronary arteries (0-3) in the H. pylori-infected group and non-infected group assessed by the proportion of the patient (%). The mean number for the coronary artery stenosis more than 30% in the H. pylori-infected group and non-infected group was 1.21±1.14 and 0.85±1.18, respectively (p
=0.15).
study population which is described in Table 2. Among 54 CHD patients, 40 (74.1%) patients had a H. pylori infection.
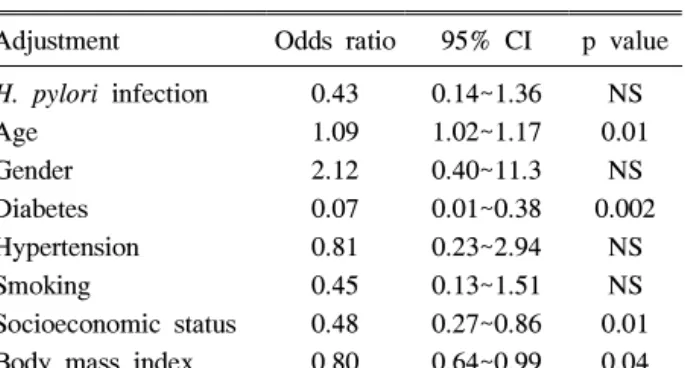
In contrast, among the 40 non-CHD patients, 21 (52.5%) patients had a H. pylori infection. Odds ratio was 2.59 with a confidence interval of 0.80~6.17 (p=0.03). However, it diminished below 1.0 after adjusting the conventional risk factors in a logistic regression analysis (Table 3).
DISCUSSION
H. pylori is known to evoke an inflammatory response in tissue by pro-inflammatory cytokines, altering the coagu- lation activity by damaging the gastric mucosa. This involves
Table 2. Relationship between H. pylori Infection and Coronary Heart Disease in Different Patient Groups
Patient groups Chi-
square p value Whole study population (N=94)
Patient without diabetes (N=70) Patient without diabetes and hypertension (N=46)
Patient without diabetes, hypertension, and smoking (N=21)
4.70 3.23 1.17 2.52
0.03 NS NS NS
NS, not significant.
Table 3. Relationship between Coronary Heart Disease and Risk Factors
Adjustment Odds ratio 95% CI p value H. pylori infection
Age Gender Diabetes Hypertension Smoking
Socioeconomic status Body mass index
0.43 1.09 2.12 0.07 0.81 0.45 0.48 0.80
0.14~1.36 1.02~1.17 0.40~11.3 0.01~0.38 0.23~2.94 0.13~1.51 0.27~0.86 0.64~0.99
NS 0.01
NS 0.002
NS NS 0.01 0.04 CI, confidence interval; NS, not significant.
various bacterial and host dependent toxic substances that are associated with an increased risk of CHD.1,15,16 In Korea, several reports have suggested that H. pylori may be associated with CHD, ischemic cerebrovascular disease and cardiovascular risk factors.17-20 H. pylori is known to affect the level of CRP, fibrinogen, cholesterol, homocysteine, and triglyceride, and all of these are important factors in CHD.4,21 However, in our study, the mean level of LDL, WBC, CRP, fibrinogen, homocysteine, PT, aPTT, PAI-1, and tPA showed no significant difference between the H.
pylori-infected group and non-infected group. Even though our study subjects do not represent the whole H.
pylori-infected population, our result indicates that an active H. pylori infection does not always evoke systemic inflammation. This is consistent with previous study that H.
pylori infection was not associated with serum CRP levels in Korean population.22
The data from our study demonstrates that H. pylori infection is related to CHD by its dependence on other cardiovascular risk factors. There was a significant relevance
Lee SY, et al. H. pylori and Coronary Heart Disease 197
between CHD and SES (p=0.02), but not according to the status of H. pylori infection. The acquisition of H. pylori is known to be associated with poverty which explains the part of the link between childhood poverty and adult CHD.23 The logistic regression analysis revealed that H. pylori infection is not related to CHD when the other risk factors are adjusted. This suggests that an active H. pylori infection might be confused as an independent risk factor in CHD, but in fact, it is so only when the other cardiovascular factors have not been adjusted.
According to our result, CHD is not a simple disease that can be provoked merely by an active H. pylori infection because the relationship between H. pylori infection and CHD with cardiovascular risk factors seemed to be irrelevant. The Jeopardy score, which encompasses coronary stenotic regions with more than 70% of luminal narrowing, also seemed irrelevant to active H. pylori infection.
However, there is still a possibility of chronic persistent inflammatory changes due to H. pylori infection that could be shown as the coronary arterial luminal narrowing in our study. We suspect that some cardiovascular risk factors, such as old age, SES, BMI, and diabetes, affect CHD along with H. pylori infection because these are shared risk factors in both CHD and H. pylori infection.
In conclusion, active H. pylori infection was not an independent risk factor in CHD and it does not alter the coagulation system or evoke a systemic inflammatory response. However, it can be easily confused as a risk factor of CHD due to other conventional major cardiovascular risk factors related with H. pylori infection. The association of H. pylori infection and atheromatous change of coronary artery needs better confirmation, especially concerning the major cardiovascular risk factors.
요 약
목적: 여러 연구를 통해 헬리코박터 감염과 심혈관 질환 의 연관성이 밝혀졌으나, 급성 염증반응 혹은 만성 동맥경 화성 변화와 관련이 있는지에 대해서는 정립된 바가 없다.
본 연구에서는 헬리코박터 감염이 심혈관, 급성염증인자, 응고인자에 영향을 미치는지 알아보았다. 대상 및 방법: 흉 통을 주소로 내원한 94명의 환자에서 혈액검사를 통해서 low density lipoprotein, white blood cell count, C reactive protein, fibrinogen, homocysteine, prothrombin time, activated partial thrombin time, plasminogen activator
inhibitor type-1, tissue-type plasminogen 수치를 측정하였 다. 심혈관 조영술 검사를 통해 30% 이상 좁아진 혈관을 양성 소견으로 판단하였고, 상부위장관 내시경검사시 조직 을 채취하여 헬리코박터 감염여부를 판단하였다. 결과: 총 54명의 환자에서 심혈관 내경이 30% 이상 좁아진 이상소 견이 발견되었으며, 헬리코박터 감염에 양성인 군과 음성 인 군으로 나누어 비교한 결과, 급성염증인자, 응고인자, atheromatous burden score, Jeopardy score에는 차이가 없었 다. 또한, 심혈관 질환에 대한 헬리코박터 감염의 교차비는 2.59였으나 나이, 성별, 당뇨, 고혈압, 흡연, 체질량지수, 사 회경제상태 등의 위험인자를 보정한 보정 교차비는 1.0이 하로 감소하였다. 결론: 헬리코박터 감염은 심혈관 질환의 독립적인 위험인자가 아니며, 응고인자나 급성염증인자에 영향을 미치지 않는다.
색인단어: 헬리코박터, 심혈관 질환, 위험인자
REFERENCES
1. Mendall MA, Goggin PM, Molineaux N, et al. Relation of Helicobacter pylori infection and coronary heart disease. Br Heart J 1994;71:437-439.
2. Gunn M, Stephens JC, Thompson JR, Rathborne BJ, Samani NJ. Significant association of cagA positive Helicobacter pylori strains with risk of premature myocardial infarction.
Heart 2000;84:267-271.
3. Whincup PH, Mendall MA, Perry IJ, Strachan DP, Walker M. Prospective relations between Helicobacter pylori infection, coronary heart disease, and stroke in middle aged men. Heart 1996;75:568-572.
4. Tsai WC, Li YH, Sheu BS, et al. Association of elevation of anti-Helicobacter pylori antibody with myocardial ischemic events in coronary artery disease. Am J Cardiol 2001;87:1005-1007.
5. Danesh J, Youngman L, Clark S, Parish S, Peto R, Collins R. Helicobacter pylori infection and early onset myocardial infarction: case-control and sibling pairs study. BMJ 1999;
319:1157-1162.
6. McDonagh TA, Woodward M, Morrison CE, et al.
Helicobacter pylori infection and coronary heart disease in the North Glasgow MONICA population. Eur Heart J 1997;18:1257-1260.
7. Pasceri V, Cammarota G, Patti G, et al. Association of virulent Helicobacter pylori strains with ischemic heart disease. Circulation 1998;97:1675-1679.
8. Osawa H, Kawakami M, Fujii M, et al. Helicobacter pylori
대한소화기학회지: 제44권 제4호, 2004 198
infection and coronary heart disease in Japanese patients.
Cardiology 2001;95:14-19.
9. Rupprecht HJ, Blankenberg S, Bickel C, et al. Impact of viral and bacterial infectious burden on long-term prognosis in patients with coronary artery disease. Circulation 2001;
104:25-31.
10. Graham KS, Graham DY. Contemporary diagnosis and management of H. pylori associated gastrointestinal diseases.
2nd ed. Newtown, Pennsylvania: Handbooks in Health Care Co., 2002:70-95.
11. Khairy P, Rinfret S, Tardif JC, et al. Absence of association between infectious agents and endothelial function in healthy young men. Circulation 2003;107:1966-1971.
12. Fraser AG, Scragg RK, Cox B, Jackson RT. Helicobacter pylori, Chlamydia pneumoniae and myocardial infarction.
Intern Med J 2003;33:267-272.
13. Hollingshead AB. Two factor index of social position. New Haven: Yale University, 1965:119-121.
14. Califf RM, Phillips HR 3rd, Hindman MC, et al. Prognostic value of a coronary artery jeopardy score. J Am Coll Cardiol 1985;5:1055-1063.
15. Crabtree JE, Shallcross TM, Heatley RV, Wyatt JI.
Mucosal tumor necrosis factor alpha and interleukin-6 in patients with Helicobacter pylori associated gastritis. Gut 1991;32:1473-1477.
16. Kowalski M. Helicobacter pylori (H. pylori) infection in coronary artery disease: influence of H. pylori eradication on coronary artery lumen after percutaneous transluminal
coronary angioplasty. The detection of H. pylori specific DNA in human coronary atherosclerotic plaque. J Physiol Pharmacol 2001;52:3-31.
17. Rhee EJ, Sung KC, Kim BS, et al. Prevalence of Helico- bacter pylori infection and its association with cardiovas- cular risk factors in Korean adults. Korean J Med 2002;
63:469-476.
18. Park MH, Lee SH, Kim BJ, Park KW, Lee DH, Park MK.
Helicobacter pylori infection and monocyte CD14 receptor gene polymorphism in stroke patients. J Korean Neurol Assoc 2001;19:337-341.
19. Kim KH, Jeong MH, Shin JH, et al. The role of chronic infection and inflammation in Korean patients with coronary artery disease. Korean Circ J 2000;30:1107-1116.
20. Han JY, Park JS, Yu KH, et al. The effects of Helicobacter pylori & cytomegalovirus infection on the risk of restenosis after percutaneous transluminal coronary angioplasty. Korean Circ J 2000;30:39-48.
21. Martin-de-Argila C, Boixeda D, Canton R, Gisbert JP, Fuertes A. High seroprevalence of Helicobacter pylori infection in coronary heart disease. Lancet 1995;346:310.
22. Sung KC, Kang JH. Serum C-reactive protein level and its association with H. pylori infection and other risk factors in apparently healthy Korean. Korean Circ J 2002;32:573-580.
23. Mendall MA, Goggin PM, Molineaux N, et al. Childhood living conditions and Helicobacter pylori seropositivity in adult life. Lancet 1992;339:896-897.