ORIGINAL ARTICLE
신경근육접합질환의 전기생리학적 진단
을지대학교 의과대학 을지병원 신경과학교실
권 오 현
Electrophysiological Diagnosis of Neuromuscular Junction Disorders
Ohyun Kwon, MD
Department of Neurology, Eulji Hospital, College of Medicine, Eulji University, Seoul, Korea
KEYWORDS Lambert-Eaton
myasthenic syndrome, Myasthenia gravis, Neuromuscular
transmission, Repetitive nerve
stimulation
Neuromuscular junction (NMJ) disorder can be primarily diagnosed by its characteristic clinical features. Electrophysiological study of repetitive nerve stimulation test (RNST) or single fiber electro- myography (SFEMG) should be considered to do ancillary diagnostic role next to the clinical findings from each patient’s own clinical history and examination. RNST has been considered as a principal electrodiagnostic tool for NMJ disorder, even helping discriminate its underlying pathophysiology, that is, whether it is presynaptic or postsynaptic disorder. To get its optimal sensitivity and specificity, RNST should be applied under the well-designed protocol and with correct technical skills not to get erro- neous results subsequently leading misdiagnosis. This article will focus mainly on the principles and the possible fallacies in performing and interpreting RNST and some comment be added about the role of SFEMG in diagnosing NMJ disorders.
Address for correspondence: Ohyun Kwon, MD
Department of Neurology, Eulji Hospital, College of Medicine, Eulji University 14 Hangeulbiseok-gil, Hagye-dong, Nowon-gu, Seoul, 139-872, Korea Tel: +82-2-970-8312, Fax: +82-2-974-7785, E-mail: [email protected]
서 론
운동신경의 활동전위(action potential)가 근육섬유활동전위 (muscle fiber action potential)를 발생시키고 수축(contraction) 을 유발하기 위해서는 운동신경 축돌기 종말(axon terminal) 에서 근육섬유의 종판(end plate)으로 원활한 신호전달이 필 요하다. 이를 위해 운동신경과 근육섬유 사이에는 고도로 특화된 신경근육접합(neuromuscular junction)이 존재한다.
정상 생리적 상황에서는 모든 운동신경의 활동전위는 100%
모두 성공적으로 신경근육접합을 지나 종판전위(end plate)를 문턱값(threshold) 이상으로 탈분극(depolarization)시켜 근육 섬유활동전위를 발생시킨다. 이에 반해 운동신경 축돌기 종말, 신경근육접합, 그리고 근육섬유 종판에 이상이 있어 신경근육전달에 장애를 초래하는 경우 이를 통틀어 신경근
육접합질환(neuromuscular junction disorder)이라 지칭한다.
신경근육접합질환은 침범된 해부학적인 구조물에 따라 일반 적으로 시냅스전질환(presynaptic disorder) 및 시냅스후질환 (postsynaptic disorder)으로 크게 구분되며 중증근무력증(mya- sthenia gravis, MG) 및 램버트-이튼 근육무력증후군(Lambert- Eaton myasthenic syndrome, LEMS)이 각각의 대표적인 질환 이다.
신경근육접합의 기능 즉, 신경근육전달(neuromuscular trans- mission)을 평가하는 대표적인 검사로 반복신경자극검사(repe- titive nerve stimulation test) 및 단일섬유근전도검사(single fiber electromyography)가 있다. 두 검사 모두 운동신경 활동 전위가 신경근육접합을 통해 성공적으로 신경근육전달된 결과 즉, 근육섬유활동전위를 반영하는 검사이다. 반복신경 자극검사는 성공적인 신경근육전달에 의한 결과물인 운동
Table 1. Oh’s method of repetitive nerve stimulation test (From Oh SJ. Principles of clinical electromyography: Case studies.
Baltimore, Williams & Wilkins, 1998)
Electrode placementRecording surface electrodes are placed in the ADQ amd FCU muscles Stimulating surface electrodes are places at the elbow sulcus of the ulnar nerve Testing program
A single stimulation to record the CMAP at rest Exercise of the ADQ muscle for 30 seconds
Immediately after exercise, a single stimulation to record the CMAP to observe postexercise fascilitation 2-Hz stimulation for 3 seconds (six responses)
3-Hz stimulation for 2 seconds (six responses) 5-Hz stimulation for 1 seconds (five responses)
50-Hz stimulation for 1 seconds (titanicstimulation (50 responses)
5-Hz stimulation for 1 seconds (five responses), immediately after tetanic stimulation to observe posttetanic fascilitation 5-Hz stimulation for 1 seconds (five responses), 4 minutes after tetanicstimulation to observe posttetanic exhaustion Measurements
The peak-to-peak amplitude is measured. The amplitude of the initial CMAP is compared with the postexercise CMAP to screen LEMS. At low rates of stimulation (2~5 Hz), the first response is compared with the lowest CMAP among the first five responses. At 50-Hz stimulation, the first response is compared with the lowest or highest CMAP elicited in 1 second.
Skin temperature
>32℃
ADQ, abductor digiti quinti; FCU, flexor carpi ulnaris; CMAP, compound muscle action potential; LEMS, Lambert-Eaton myasthenic syndrome.
섬유활동전위들의 전기생리적인 총합, 즉, 복합근육활동전 위(compound muscle action potential, CMAP)의 크기 - 진폭 (amplitude)이나 면적(area) – 를 통해, 단일섬유근전도검사는 all-or-none 반응이 아닌 점층적인 반응(graded response)을 보이는 종판전위가 all-or-none 반응을 보이는 근육섬유활동 전위의 유발에 필요한 문턱전위(threshold potential)에 도달 하여 근육섬유활동전위가 생성될 때까지 소요되는 시간의 변이, ‘지터’(jitter)를 평균연속차이(mean consecutive diffe- rence)라는 척도를 통해 평가한다. 결국 반복신경자극검사는 운동신경의 활동전위가 근육섬유활동전위로 성공적으로 전달되는지 여부만을 즉, 신경근육전달이 성공이냐 실패냐 만을 평가하나, 단일섬유근전도검사는 이 뿐만 아니라(단일 섬유근전도검사에서 신경근육전달의 실패는 차단(blocking) 으로 나타난다) 신경근육전달이 얼마나 일관적으로, 그리고 효율적으로 빠른 시간에 이루어지는지도 평가하게 된다.
시험에 비유하자면, 반복신경자극검사는 합격인지 불합격 인지만 알려주는데 반해, 단일섬유근전도검사는 점수까지 제시하여 모든 신경근육전달의 성적을 순위로 매겨 보여준 다고 비유할 수 있겠다. 단일섬유근전도검사는 반복신경자 극검사에 비해 월등히 예민하게 신경근육전달의 이상을 확 인할 수 있으나, 일차적인 신경근육접합질환이 아닌, 근육 위축가쪽경화증 등의 신경인성 과정(neurogenic process)이나 근육디스트로피, 근육염 등의 근육인성 과정(myogenic process) 에 의한 이차적 신경근육전달의 이상과의 감별이 사실상 불가능하여 훌륭한 예민도에도 불구하고 실제 임상에서 단일 섬유근전도검사가 적용될 수 있는 영역은 제한적이다. 중증
근무력증이나 램버트-이튼 근육무력증후군 등의 신경근육 접합질환 진단에 일차적으로 사용되는 전기생리적 검사법은 반복신경자극검사라 할 수 있다.1,2 본 글에서는 그 논의를 반복신경자극검사의 경우로 주로 한정하며, 단일섬유근전도 검사의 임상적인 의의에 대해서 간단히 언급하고자 한다.
반복신경자극검사 및 단일섬유근전도검사 전반에 대한 교과 서적인 지식을 얻고자 하는 독자는 관련 책자를 일독하도록 권한다.3-5
반복신경자극검사의 원리 및 구성
반복신경자극검사는 반복적인 연속 자극(trail of stimuli)을 주고, 각 CMAP의 크기를 정량적으로 비교한다는 점을 제외 하고는 일반적인 운동신경전도검사(motor nerve conduction study)의 시행 방법과 그 원리를 함께 한다. 반복신경자극검 사는 근육의 휴지기의 CMAP를 얻은 다음, 우선 일련의 저 빈도자극(lower rate stimulation)으로, 그리고 나서 고빈도자 극(higher rate stimulation)에 따른 일련의 CMAP를 구한다.
또한 고빈도자극 직후 그리고 수분이 지난 후 – 혹은 피험자 스스로 최대 근력으로 10-30초간 지속적인 근육 수축을 하게 한 직후, 그리고 수분이 지난 후 – 다시금 저빈도자극을 가해 CMAP의 정량적 변화를 확인하는 것으로 구성된다(Table 1). 최초의 CMAP의 진폭이나 면적에 대응하여 뒤따라오는 CMAP의 진폭이나 면적의 정량적인 변화를 본다는 면에서 최초 CMAP를 얻을 때 운동신경에 최대상자극(supramaximal stimulation)이 전달됨을 확실히 하는 것이 중요하다.
Figure 1. Repetitive stimulation findings. Under normal conditions the quantal content resulting from depolarization of the nerve terminal at about 2-3 Hz sequentially declines to about 50% of that arising from the initial stimulus. There is an associated decline in the magnitude of the EPP, as one would expect given the Ach reduction; however, all of the EPPs are suprathreshold for the muscle fiber’s action potential. Because the electricalresponse of single fiber action potentials (SFAPs) is an all-or-none phenomenon, as long as the EPP is suprathreshold, each muscle depolarization is essentially identical. The ensuing CMAP is simply the electrical summation of all activated SFAPs and hence is the same with each peripheral nerve trunk depolarization. In a postsynaptic disorder such as myasthenia gravis (MG), the EPPs fall below threshold in response to the normal quantal content reduction secondary to a reduced safety factor. Once this occurs at some NMJs, there is blocking of the SFAP and the CMAP also declines. With a prejunctional disorder of significantly reduced quantal content, EPPs of multiple muscle fibers are reduced upon initiation of stimulation. Only a few SFAPs occur secondary to the markedly reduced number of EPPs. The corresponding CMAP is also significantly reduced and additional NMJs are induced to fail with slow rates of repetitive stimulation. (From Radecki PL. Electrodiagnostic evaluation of neuromuscular junction disorders. In: Dumitru D (ed): Clinical Electrophysiology. Philadelphia, Hanley & Belfus, 1989, pp757-778.)
최대 CMAP를 확인한 다음, 2, 3, 5 Hz의 저빈도자극에 따른 CMAP의 크기 변화를 확인한 다음, 10 Hz 이상의 고빈 도자극을 수십 회 이상 운동신경에 가하고 이에 따른 CMAP 의 변화 양상을 확인한다. 정상적으로 최대상자극은 지배 받는 근육의 모든 근육섬유에서 활동전위를 유발하여 그 근육에서 얻을 수 있는 최대 CMAP를 얻는다. 정상 생리적 환경에서는 반복적인 저빈도자극에 의해 종판전위가 점차 적으로 감소하더라도 종판에서 근육섬유활동전위를 유발 하는데 필요한 문턱값에 여유있게 도달하므로(safety factor), CMAP의 진폭이나 면적 값은 일련의 반복 자극에서도 일정한 최대값을 보이게 된다. 이에 비해 중증근무력증이나 램버트-
이튼 근육무력증후군에서는 최초의 종판전위가 정상보다 작아 연속된 일련의 종판전위가 점진적으로 작아질 때, 이중 일부는 문턱값에 도달하지 못하므로, 근육섬유활동전위를 유발하지 못하게 되고 결과적으로 CMAP의 진폭이나 면적 이 점차 감소하는 감쇠반응(decremental response)을 보이게 된다(Fig. 1). 고빈도자극에서는 축돌기 종말에 칼슘이 축적 되어 분비되는 아세틸콜린의 양이 증가하게 되어, 저빈도 자극에서 분비되는 아세틸콜린의 양이 적었던 램버트-이튼 근육무력증후군은 점차 보상되어 정상 종판전위를 회복하게 되고, 이는 최초의 작았던 CMAP가 점차적으로 정상 진폭 및 면적을 회복하는 증강반응(incremental response)을 보인다.
Figure 2. Posttetanic facilitation and exhaustion in a patient with myasthenia gravis. (A) Results of repetitive stimulation at 3-Hz stimulation. Note 40% decrement. (B) A decrement at the second period of 50-Hz stimulation. (C) About 10-15 seconds following the high-rate stimulation, the decrement is only 9%. (D) Four minutes after the tetanic stimulation, a decrement of 54% is obvious.
(E) Twenty-five minutes after the high-rate stimulation, the decrement is 37% and approaching the resting state. (F) Diagrammatic representation of facilitation and exhaustion as competitive factors generating the net CMAP response. (From Desmedt JE.
Presynaptic mechanisms in myasthenia gravis. Ann N Y Acad Sci 1966;135:209-246)
피험자 의지로 최대 근력으로 수축을 유지하는 즉, 테타니 수축(tetanic contraction)은 이러한 고빈도자극에 대응하는 생리적 활동으로서 고빈도자극에서처럼 램버트-이튼 근육 무력증후군에서 CMAP의 증강반응을 유도할 수 있다. 이러 한 최대 근력의 수축이 전기 자극에 의해 유발되었는지, 피 험자 스스로 수축하였는지에 따라 이러한 증강반응을 테타 니후촉진(posttetanic facilitation) 혹은 운동후촉진(postexer- cise facilitation)이라 한다. 그러나 테타니 수축이나 최대 근력 을 사용한 운동 이후 수분이 경과한 후에는 저빈도자극 시 기존의 감쇠반응이 더 심해지게 된다. 이를 운동후탈진(post- exercise exhaustion) 혹은 테타니후탈진(posttetanic exhaustion) 이라 한다. 원리를 간단히 살펴보자면, 테타니 혹은 운동 후 축돌기 종말에 축적된 칼슘에 의해 아세틸콜린의 분비가 증강되어 신경근육전달의 safety factor가 호전되고, 결과적 으로 ‘촉진’이 나타난다. 이후 1-3분간에 걸쳐 칼슘은 다시 세포외로 방출되어 축돌기 말단의 칼슘 농도는 평상시 수 준으로 회복하는데 반해, 아직 아세틸콜린 소포체의 수는 평상 수준으로 회복하지 못해 신경근육전달은 평상시보다 더 불량해지고 감쇠반응은 더욱 커지는 ‘탈진’이 나타난다.
일반적으로 촉진은 테타니나 운동 직후 가장 뚜렷하며 점 차 그 강도는 줄어 약 20-30초까지 지속되고, 탈진은 2-5분
사이에 뚜렷하다. 운동/테타니후 15-20분이 경과하면 신경 근육전달은 평상 수준을 회복한다(Fig. 2).5 연구에 따르면, 온전히 아세틸콜린의 방출량이나 세포내 칼슘의 농도로만 설명하기는 어렵다고 하며, 아세틸콜린수용체의 탈감작(de- sensitization) 등이 가능한 기전으로 언급된다.6
반복신경자극검사의 기술
일반적인 운동신경전도검사와 동일하게 운동신경에 최대 상자극(supramaximal stimuli)을 가하고 이 운동신경의 지배를 받는 근육의 CMAP는 표면전극으로 측정치를 얻으며, 활동 전극을 힘살에, 기준전극을 건에 부착하는 일반적인 belly- tendon method을 사용한다. 신경 자극은 운동신경전도검사 와 마찬가지로 반드시 최대상자극(supramaximal stimulation) 으로 해야 한다. 단지 차이점은 자극이 연속(train of stimuli) 으로 주어지고 활성화 과정(activation procedure)으로서 일 정한 형태의 운동(conditioning exercise)을 한다는 것 그리고 움직임을 방지하기 위해 고정(immobilization)을 해야 한다는 것 등이다.
운동신경을 연속적으로 자극하고 이 운동신경에 지배를 받는 근육에서 CMAP를 기록한다. 저빈도자극은 2, 3, 5 Hz의
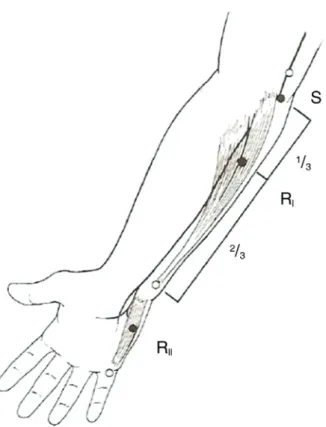
Figure 3. Oh’s method of RNST on the flexor carpi ulnaris (R
I) and abductor digiti quinti (R
II). (From Oh SJ. Principles of clinical electromyography: Case studies. Baltimore, Williams & Wilkins, 1998)
속도로 통상적으로 5회의 연속 자극을 주며, 피지배 근육의 CMAP의 크기를 기록한다. 고빈도자극은 운동신경에 50 Hz 의 자극을 1초간, 즉 50개의 연속된 자극을 주거나(tetanic stimulation), 피험자 스스로 최대 근력으로 근육을 수축토록 하고 직후 다시 하나의 CMAP를 전기 자극으로 얻고 10초 뒤에 저빈도자극을 5번 가하여 CMAP의 크기 변화를 추적 한다. 그리고 피험자는 휴식을 취하면서 일반적으로 4분 후 다시 저빈도자극을 더 가하여 CMAP의 변화를 확인한다 (Table 1).3
일반적으로 팔에서는 새끼두덩근육(hypothenar muscle), 엄지두덩근육(thenar muscle), 어깨세모근(deltoid), 등세모근 (trapezius)을, 다리에서는 앞정강근(tibialis anterior), 네갈래 근(quadriceps)을, 얼굴에서는 눈둘레근(orbicularis oculi), 입 둘레근(orbicularis oris), 코근(nasalis)을 선택한다. 그러나 가 능하다면, 환자가 임상적으로 근위약이나 피로를 호소하는 근육을 빠뜨리지 않고 검사하는 것이 검사의 예민도를 높 이는 데 중요하다. 특히, MuSK항체 양성 중증근무력증 환 자는 특징적으로 얼굴 근육의 위약과 근육위축이 있어 팔 다리의 근육에서는 반복신경자극검사가 정상이더라도, 얼 굴근육에서 특징적으로 이상을 보이는 경우가 많기 때문에
반복신경자극검사에 얼굴 근육을 포함하는 것이 필수적이 다. 일반적으로 먼쪽 근육은 근육의 체적이 작고 운동에 의 한 간섭이 없도록 고정하기 쉬워 상대적으로 검사가 용이 하다. 그러나, 중증근무력증은 일반적으로 팔다리 근육 중 몸쪽 근육이 보다 더 심한 위약을 보이는 경우가 많으므로 먼쪽 근육에서 정상 결과인 경우, 임상적으로 의심한다면 몸쪽 근육에 대한 검사를 반드시 해야 한다. 다만, 몸쪽 근 육을 자극 시 운동신경이 깊이 위치하고 있는 경우가 많아 최대상자극이 되지 않고 그 이하의 강도로 자극이 될 수 있 으며 또한 몸쪽 근육의 수축 시 큰 관절 운동에 의한 움직 임으로 기록전극의 부착이 느슨해지거나, 그리고 근육의 체적이 큰 경우가 많아 일반적인 표면전극으로는 근육섬유 활동전위의 일부만 반영할 수 있기에 CMAP의 크기를 잘못 측정하는 기술적인 오류의 발생 가능성이 커지므로 결과에 대한 세심한 해석이 요구된다. 그래서 등세모근에서 반복 신경자극검사를 할 때는 비교적 검사의 오류 가능성이 적 도록 2 Hz나 3 Hz의 저빈도자극만을 추천하기도 한다.4
한 신경을 자극하여 몸쪽과 먼쪽 근육에서 동시에 기록하 는 방법, 예를 들어 자신경을 자극하여 새끼벌림근(abductor digiti minimi)과 자쪽손목굽힘근(flexor carpi ulnaris)에서 동 시에 기록하는 것도 자극 횟수를 줄여 환자의 불편을 덜어 줄 수 있는 좋은 방법이다(Fig. 3).
반복신경자극검사는 CMAP크기의 일련의 정량적인 변화 를 그 결과로 하기에 검사 과정에 있어 CMAP의 정확한 측 정이 다른 어느 신경생리학적 검사보다 강조된다. 이를 위해 특히 근육의 수축에 의해 유발되는 관절의 움직임과 근육의 온도에 대한 세심한 고려가 필요하다.
반복적인 운동신경의 자극은 필연적으로 근육의 수축 및 그에 따른 관절의 움직임을 유발한다. CMAP의 정량적인 변화를 보는 반복신경자극검사에서는 기록전극의 안정적인 부착이 필수적인 요건이며, 움직임에 의해서 기록전극이 정상적으로 부착되지 않을 경우 틀린 CMAP의 파형을 얻을 수 있으므로 반드시 움직임을 최소화하도록 “Jolly test board”
라든지 벨크로테이프 등으로 피험자의 손이나 팔을 고정해 야 한다. 근육의 신전 및 수축 상태는 또한 표면전극과 근육 섬유와의 거리, 근육섬유활동전위의 전달 속도의 변화를 일 으켜 결과적으로 CMAP의 모양과 크기를 변화시켜 반복 신경자극검사의 민감도 및 신뢰성에 나쁜 영향을 미칠 수 있다.7
무엇보다도 반복신경자극검사를 할 때 가장 중요하게 고 려해야 할 생리적 조건은 온도이다. 근육의 온도가 떨어지 면, 시냅스-전 신경 종말에서 신경전달물질의 유리가 촉진 되고, 34℃ 이하에서는 아세틸콜린에스테라제 활성도가 낮 아져 아세틸콜린의 가수분해 속도가 느려져 아세틸콜린에
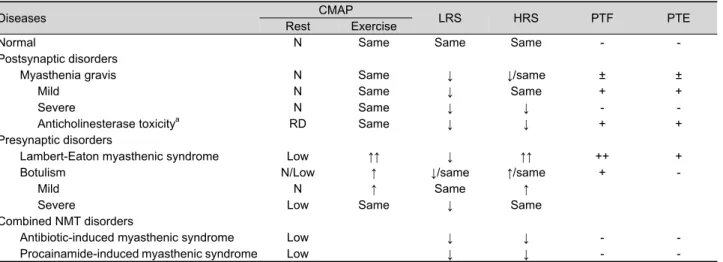
Table 2. Classical findings in the repetitive nerve stimulation test in neuromuscular transmission diseases (From Oh SJ.
Principles of clinical electromyography: Case studies. Baltimore, Williams & Wilkins, 1998)
Diseases CMAP
LRS HRS PTF PTE
Rest Exercise
Normal N Same Same Same - -
Postsynaptic disorders
Myasthenia gravis N Same ↓ ↓/same ± ±
Mild N Same ↓ Same + +
Severe N Same ↓ ↓ - -
Anticholinesterase toxicitya RD Same ↓ ↓ + +
Presynaptic disorders
Lambert-Eaton myasthenic syndrome Low ↑↑ ↓ ↑↑ ++ +
Botulism N/Low ↑ ↓/same ↑/same + -
Mild N ↑ Same ↑
Severe Low Same ↓ Same
Combined NMT disorders
Antibiotic-induced myasthenic syndrome Low ↓ ↓ - -
Procainamide-induced myasthenic syndrome Low ↓ ↓ - -
aThis includes organophosphate poisoning
N, normal; -. absent; +, mildly present; ++, prominently present; ↓ decremental response; ↑ mild incremental response; ↑↑ marked incremental response; CMAP, compound muscle action potential; HRS, high rate stimulation; LRS, low rate stimulation; NMT, neuromuscular transmission; PTE, posttetanic exhaustion; PTF, posttetanic fascilitation; RD, repetitive discharge.
Table 3. Differentiation among neuromuscular transmission disorders, myopathy, and denervation process by SFEMG findings (From Oh SJ. Principles of clinical electromyography: Case studies. Baltimore, Williams & Wilkins, 1998)
Parameters NMT disorders Myopathies Denervation process
Fiber density Normal ++ +++
Abnormal jitter +++ ++ ++
Blocking
Neuromuscular ++ - +
neurogenic - - +
NMT, neuromuscular transmission.
대한 감수성이 증가되는 한편, 자극 후 신경말단에서 칼슘 이온이 소멸되는 속도가 감소하기 때문에 전반적으로 신경 근육전달의 효율은 개선되어 결과의 위음성(false negative result)을 얻을 수 있다.8 그러므로, 검사하는 근육의 온도는 항상 확인되어야 하며, 일반적으로 적어도 32℃ 이상을 유 지하도록 하고 있다. 이러한 생리적 현상을 반대로 이용하 여 40℃ 이상의 고온에서 반복신경자극검사를 함으로써 검 사의 진단적 예민도를 높이고자 하는 시도도 있다.9
반복신경자극검사의 해석
반복신경자극검사는 대부분 임상에서 중증근무력증이나 램버트-이튼 근육무력증후군 등의 신경근육접합질환을 진 단하기 위한 검사법이나, 이들 질환을 진단하는 최적의 기 준(gold standard)은 아니다. 위의 질환들은 일차적으로 임상 적으로 진단이 되는 것이며 반복신경자극검사는 이에 대한 객관적 지표로 사용될 수 있다. 반대로 뚜렷하고 중대한 임상 증상에도 불구하고 음성의 결과가 나왔다면, 임상 진단에 대한 재고찰이 필요함도 물론이다.
저빈도자극에서의 비정상적인 감쇠반응은 10% 이상일 경우로 정하고 있다. 첫 번째 CMAP의 크기 – 면적 혹은 진 폭 – 를 100%로 하고 네 번째나 다섯 번째의 CMAP 크기를 판정의 기준으로 한다. 고빈도자극에서의 비정상적인 증강 반응은 일반적으로 첫 번째 CMAP에 비해 50번째 CMAP가 100% 이상 증가될 경우로 정한다. 일부에서는 증강반응의 기준을 60%로 하면 램버트-이튼 근육무력증후군 진단의 특 이도는 저하시키지 않으며 민감도를 더 향상시킬 수 있다 주장하나 일반적으로 받아들여지고 있지 않다.1
반복신경자극검사의 시냅스-후 신경근육접합질환인 중증 근무력증에 대한 진단적 예민도, 즉 저빈도자극에서의 비 정상 감쇠반응의 빈도는 50-80% 수준이다. 대표적 시냅스-전 신경근육접합질환인 램버트-이튼 근육무력증후군은 3가지 특징적인 전기생리학적 소견, 즉, 휴식 시의 감소된 CMAP 크기, 저빈도자극 시의 감쇠반응, 그리고 고빈도자극이나 운동 직후 증강반응으로 진단할 수 있는데, 90% 이상의 환 자에서 최초 CMAP의 감소 소견, 저빈도자극 시 감쇠반응 이 있으며, 현실적으로 모든 환자에서 운동 직후나 고빈도자 극에서 증강반응이 양성으로 나타난다.
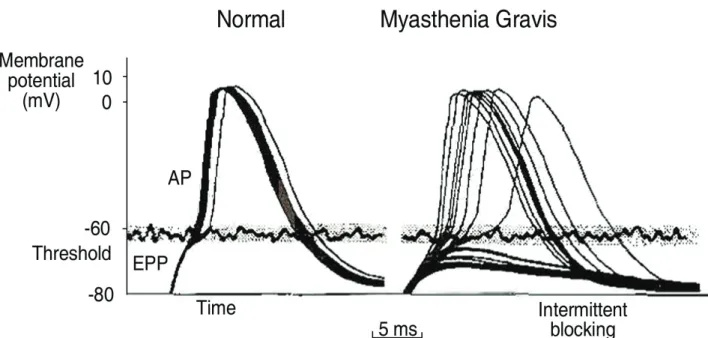
Figure 4. A schematic explanation of jitter in both a normal and myasthenic NMJ. A. A normal NMJ demonstrates a small amount (<50 μs) of variability in achieving threshold from one depolarization to the next. Each EPP is of sufficient magnitude to reach threshold and generate a single muscle fiber action potential. B. End plate potentials recorded from a patient with myasthenia gravis. Note both the increased time and variability from one depolarization to the next. The different numbers of AchRs activated with each depolarization are barely able to reach threshold because of the borderline number of AchRs. As each depolarization has a different rise time because of a variable safety factor, significant variability and even blocking of individual EPPs occur (solid lines below the wavy threshold value approximating -60 mV). (From Stålberg E, Trontelj JV, Schwarz MS. Single fiber recording of the jitter phenomena in patients with MG and in members of their families. Ann N Y Acad Sci 1976;274;189-202)
테타니후촉진이나 테타니후탈진, 그리고 운동후촉진이나 운동후탈진을 보기 위한 테타니 후 혹은 운동 후 반복신경 자극검사의 임상적 의의는 아직 확실히 정립되지 않았다.
중증근무력증 환자 중 운동 후 반복신경자극검사는 운동 전 반복신경자극검사만 시행했을 때에 비해 약 10% 정도 상대 적으로 높은 진단적 예민도를 가진 것으로 알려져 있다.10 실제 임상에서의 운동 후 반복신경자극검사는 이처럼 중증 근무력증 진단의 예민도를 높이기 위해서도 쓰이지만, 보다 중요하게는 운동후촉진이나 운동후탈진을 확인함으로써, 운동전 반복신경자극검사에서 보인 비정상적인 감쇠반응 이 검사의 오류에서 발생한 것이 아니라 환자의 병리적 상 태를 반영한 것이라는 방증이 될 수 있으며, 또한 고빈도자 극 시의 비정상적인 증강반응이 없음을 확인하므로써 운동 전 반복신경자극검사의 감쇠반응이 램버트-이튼 근육무력 증후군과 같은 시냅스 전 장애에 의하지 않았음을 확인하는 의미가 더 크다고 하겠다.
현실적으로 반복신경자극검사에서 가장 흔히 접하게 되는 이상 소견은 저빈도자극에서의 감쇠반응이다. 유의할 점으로 저빈도자극에서의 감쇠반응은 신경근육접합질환에서만 확인 되는 소견이 아니라, 다른 병리적 과정에 의해 이차적으로
신경근육전달이 원활치 않을 경우, 다양한 근육병이나 신경 인성 과정(neurogenic process)에서, 특히 근육위축가쪽경화 증과 같이 빠르게 진행하는 질환일수록, 양성으로 나타날 수 있다. 그러므로, 반복신경자극검사는 신경근육접합질환 을 진단하는데 예민하고 간편한 검사이지만, 임상 양상이 합당하지 않다면 반복신경자극검사에서 감쇠반응을 보였 다는 사실만으로 신경근육접합질환으로 진단하는 오류를 범하지 않도록 주의해야 한다. 그 밖에도 근육긴장질환에 반복신경자극검사가 진단에 도움이 될 수 있다. 근육긴장 질환은 기본적으로 통로병증(channelopathy)로서 근육막 흥 분성(muscle membrane excitability)의 변화가 있어 짧은운동 검사(short exercise test) 및 긴운동검사(long exercise test)에 서 CMAP의 크기가 감소하는 것과 마찬가지로 일부 근육긴 장질환, 특히 열성유전 선천근육긴장증(recessive myotonia congenita)의 일부 유전자형 및 선천이상근육긴장증(paramyo- tonia congenita)에서는 반복신경자극검사에서 감쇠반응을 확 인할 수 있다. 일반적인 반복신경자극검사가 5-10번의 자극 만을 가하지만, 근육긴장질환에서는 5 Hz나 10 Hz의 자극 을 50번 정도 가하여 감쇠반응의 유무를 확인한다.11 반복 신경자극검사의 판독에서 일반적으로 간과하기 쉬운 소견
으로 반복방전(repetitive discharge)이 있다. 한 번의 자극에 반복적인 CMAP가 발생하는 경우를 반복방전이라 하며, 항 아세틸콜린에스테라제나 유기인(organophosphate)의 중독이나, 종판의 아세틸콜린에스테라제 결핍 선천근육무력증후군, 느린통로증후군(slow channel syndrome) 선천근육무력증후 군에서 확인된다.12 반복신경자극검사와는 상관없지만, 반복 방전은 과흥분성말초신경장애(Hyperexcitableperipheral nerve disorder)나 근육긴장질환에서도 보고되었다.
다양한 신경근육전달질환에 따른 반복신경자극검사의 이상 양상은 Table 2에 기술되어 있다.
단일섬유근전도검사의 신경근육접합질환의 진단적 역할
단일섬유근전도검사에서 측정하는 중요한 인자는 지터 (jitter) 및 근섬유밀도(fiber density)이다. 신경근육전달에 영 향을 미치는 모든 병적인 과정, 즉, 신경인성 과정, 신경근육 접합질환, 근육병 모두에서 두 척도는 이상을 보인다(Table 3).
특징적으로 신경근육접합질환에서는 근섬유밀도는 변화가 없는데 반해, 지터는 뚜렷하게 증가하며 질환의 중증도가 심해질수록 신경근육차단(neuromuscular blocking)이 증가하게 된다(Fig. 4). 중증근무력증에서의 단일섬유근전도검사의 진단적 민감도는 평균 95%이며, 이 검사는 워낙 민감하기에 임상적으로 위약이 있는 근육에서 단일섬유근전도검사 소견 이 정상이라면 중증근무력증 진단은 아니라고 볼 수 있다.
REFERENCES