서 론
급성신우신염(acute pyelonephritis)은 흔한 세균성 감염 중의 하나 로 배뇨통, 긴급뇨, 빈뇨, 측부통, 발열, 오한, 오심 및 구토 등의 증상 과 함께 늑척추간 압통을 보이는 신실질과 신 집뇨계의 감염이다. 급 성신우신염은 미국 통계에 의하면 매년 600만 명 이상의 새로운 환 자가 발생하고 있으며,1) 1970년대 말까지 증가 추세를 보이다가 1980 년대 중반 이후부터는 발생률이 감소하는 추세를 보이고 있으나 아 직까지도 가장 빈번한 전염성 질환 중에 하나이다.2) 국내 보고로는 1
년에 인구 10,000명당 35.7명의 높은 발병률을 보이고 이 중 5.5명이 입원치료를 받는 흔한 질환이다. 급성신우신염은 인체 내의 감염 중 에서 그 빈도가 호흡기 감염 다음으로 많은 것으로 보고되고 있고, 근래에 항생제의 오남용으로 각종 항생제에 내성균 빈도의 증가와 인체 저항력의 감소 및 병원감염의 증가로 이에 대한 적극적 예방 및 치료가 요구되고 있다.3) 이러한 항생제 감수성의 변화는 지역과 시간 에 따라 다르게 나타나므로, 경험적 초기 항생제의 선택은 그 지역사 회의 항생제 감수성을 고려하여 결정해야 할 것이다. 급성신우신염 의 가장 흔한 원인균인 Escherichia coli인 경우 trimethoprim-sulfa-
Original Article
급성신우신염에 있어서 Ciprofloxacin 내성균주가 배양된 환자들의 위험인자
최민규, 이성현, 강인영, 어윤호, 안남주, 정윤희*, 고성백
김포우리병원 가정의학과
Risk Factors of Ciprofloxacin Resistance in Acute Pyelonephritis
Min Kyu Choi, Sung Hyun Lee, In Young Kang, Yoon Ho Eo, Nam Joo Ahn, Yoon Hee Chung*, Sung Baik Ko
Department of Family Medicine, Kimpo Woori Hospital, Kimpo, KoreaBackground: Increasing ciprofloxacin resistance among Escherichia coli has been reported in worldwide, including in Korea. We aimed to identify the risk factors associated with ciprofloxacin resistance in urinary E. coli isolates.
Methods: Patients with positive urine culture result for E. coli and resistance to ciprofloxacin between April 1, 2013 and April 31, 2014 at the Kimpo Woori Hospital were prospectively identified as cases, and the isolates obtained from the cases (n= 322) were compared with ciprofloxacin susceptible E. coli isolates (controls; n= 631).
Results: Multivariate analysis revealed that urinary tract catheterization (odds ratio [OR], 2.631; 95% confidence interval [CI], 1.058-6.544; P= 0.037) and prior exposure to quinolones (OR, 13.072; 95% CI, 3.367-50.75; P< 0.001) were independent risk factors for ciprofloxacin resistance in urinary E. coli isolates. Compared with ciprofloxacin-susceptible E. coli isolates, ciprofloxacin-resistant E. coli isolates from urine specimens showed significantly higher rate of resistance to all other tested antimicrobial agents, except amikacin and imipenem.
Conclusion: In patients with urinary tract infection, urinary catheterization and prior quinolone exposure are associated with high risk of ciprofloxacin- resistance in E. coli which may lead to treatment failure.
Keywords: Ciprofloxacin; Drug Resistance, Bacterial; Escherichia coli; Risk Factors; Urinary Tract
http://www.kafm.or.kr/kjfp.2015.5.3.224pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3):224-228
KJFP
Korean Journal of Family PracticeReceived August 29, 2014 Accepted August 28, 2015 Corresponding author Yoon Hee Chung
Tel: +82-31-999-1724, Fax: +82-31-999-1899 E-mail: imkchoe@naver.com
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
최민규 외. 급성신우신염의 Ciprofloxacin 내성 위험인자 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice methoxazole (TMP-SMX)이 사용되어 왔으나, 최근 미국의 Infectious Disease Society of America’s Guideline (IDSA)에 의하면,4) 지역사회 내 의 TMP-SMX 저항성이 10-20%에 도달할 시 초기치료로 ciprofloxa- cin 및 3세대 세팔로스폴린을 권유하고 있다. 급성신우신염 국내 표 준 가이드라인에서도 ciprofloxacin은 초기치료로 권장되고 있다.5) 하 지만 국내 ciprofloxacin의 E. coli에 대한 내성률은 20% 전후로 계속 증가되고 있음이 보고되고 있다. 이는 IDSA 권장의 영향으로 보인다.6) 우리는 ciprofloxacin에 대해 저항성을 갖고 있는 E. coli가 동정된 급 성신우신염에 대한 위험인자를 조사하고, 이를 통해 급성신우신염 의 항생제 선택에 고찰이 필요함을 말하고자 한다.
방 법
1. 연구방법
연구는 김포우리병원에 내원한 환자들의 의무기록 열람을 통해 후향적으로 이루어졌다. 2013년 4월 30일부터 1년 동안 급성신우신염 으로 진단코드가 붙여진 환자들 중 E. coli가 동정된 모든 환자를 검 색하여 데이터화하였다. E. coli가 동정된 환자들 중 발열이 없거나, 빈 뇨, 급박뇨, 하복부 압통 등 급성신우신염증상이 없는 환자들은 차 트기록 및 경과기록지 리뷰를 통해 배제시켰다. 이 절차를 포함한 이 유는 초기 진단코드와 이후 경과가 다르게 보여 결과적으로 급성신 우신염에 합당하지 않은 환자들이 상당수 포함되어 있었기 때문에 보다 정확한 연구결과를 위함이었다. 배제된 환자의 수는 134명이었 다. 항생제 감수성 검사는 ampicillin-sulbactam, ampicillin, ticarcillin- clavulanate, cefmetazole, ceftazidime, ceftria, aztreonam, imipenem, gentamicin, netilmicin, amikacin, TMP-SMX, minocycline, ciprofloxa- cin을 disk diffusion method에 의해 구하였다.
2. 연구대상
급성신우신염으로 진단된 환자 중에서 소변에서 ciprofloxacin에 저항성을 갖고 있는 E. coli가 배양된 환자 그룹(ciproxacin-resistance, CR)을 실험군으로 설정하였으며, 급성신우신염으로 진단되었고, cip- rofloxacin에 감수성을 갖고 있는 균이 배양된 환자(ciproxacin-suscep- tible, CS)를 뽑아 이를 대조군으로 설정하였다. 총 대상환자 수는 953 명이며, 실험군은 322명, 대조군은 631명이었다. 의무기록 열람 및 환 자 인터뷰를 통해 ciprofloxacin 저항성 위험인자에 대한 예측인자인 나이, 성별, 외래-입원 여부, 병원감염 여부, 검체수집 90일 이내 입원 기간이 48시간 이상하였는지 여부, 기저질환의 여부, 요로계 관련 시 술 및 술기가 검체수집 2주 이내에 이루어졌는지 여부, 항생제 투여 가 검체수집 2주 이내 48시간 이상 투여되었는지 여부를 조사하였다.
기저질환의 유무는 환자 차트열람을 통해 조사되었다. 결체조직질 환은 systemic lupus erythematosus, 류마티스관절염, 베체트병이 포함 되었다. 악성종양은 고형암 및 혈액암 모두를 포함하였다. 심혈관질 환은 부정맥, 심부전, 허혈성심질환이 포함되었다. 소화기계 질환은 궤양, 위장관 출혈, 장폐쇄가 포함되었다. 신장질환은 만성심부전, 단 백뇨, 혈뇨가 포함되었다. 단백뇨는 dipstick에서 1+ (30 mg/dL)로 정 의하였다. 신경계질환은 뇌혈관질환, 치매, 파킨슨병이 포함되었다.
3. 통계분석
통계분석은 SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA)를 이용하였 으며, 유의성 판정기준은 P-value 0.05 미만으로 정의하였다. 단변량 분석은 chi-square test를 이용하였으며, 이를 이용하여 각 위험인자 에 대한 위험 정도를 계산하였다. 연속량분석은 Student t-test를 이용 하였다. 단변량분석에서 P-value 0.05 이하인 변수들은 다변량분석 (로지스틱회귀분석)을 통해 분석하여 CR의 독립적인 위험인자가 무 엇인지 분석하였다. 모든 유의수준은 P<0.05로 정의하였다.
결 과
총 953명의 환자가 진단기준을 만족시켜 연구대상에 포함되었다.
이 중 남자가 319명, 여자는 634명이었다. 실험군의 환자는 총 322명이 었으며, 이 중 남자가 134, 여자가 188명이었다. 대조군의 환자는 총 631명이었으며, 이 중 남자가 185명, 여자가 446명이었다. 평균연령은 53.6세(range, 1-98세)였다.
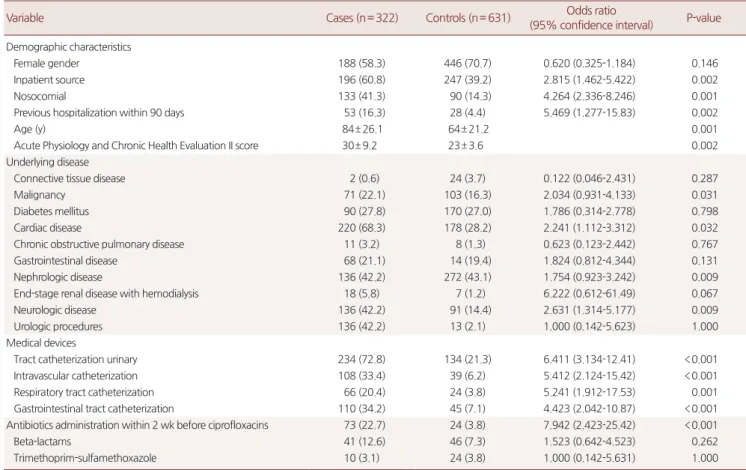
실험군과 대조군의 환자특성 및 임상적 데이터의 분석은 Table 1 에 정리하였다. 단변량분석에서 실험군이 대조군에 비해 통계적 유 의성을 갖는 변수로는 병원획득 환자, 입원기간이 90일 이내에 48시 간 이상 있었던 경우, 심혈관질환이 있었던 경우, 신경계질환이 있었 던 경우, 요로관 삽입되어 있었던 경우, ciprofloxacin 제제가 검체수 집 2주 이내 사용한 적이 있었던 경우였다. 다른 항생제 사용 여부는 통계적인 유의한 차이가 발견되지 않았다. 단변량분석에서 유의성 이 있었던 변수 중 다변량분석(로지스틱회귀분석)으로 CR의 위험인 자 분석은 Table 2에 정리하였다.
분석된 위험 독립인자로서는 도뇨관 삽입이 되어있는 환자(adjust- ed odds ratio [OR], 2.631; 95% confidence interval [CI], 1.058-6.544;
P= 0.037), ciprofloxacin 사용력이 2주 이내 있었던 환자(adjusted OR, 13.072; 95% CI, 3.367-50.75; P<0.001)였다. 실험군, 대조군에 대한 항생 제 감수성 검사는 Table 3에 수록하였다.
급성신우신염에서 항생제의 내성률은 ampicillin (89.3%), ampicil- lin/sulbactam (61.4%), TMP-SMX (83.7%)의 경우에는 내성률이 높아
Min Kyu Choi, et al. Risk Factors of Ciprofloxacin Resistance – APN
Korean Journal of Family Practice
KJFP
일차적인 항생제로 사용하는 것은 적합하지 않을 것으로 생각되며, cephalosporin 계열 항생제인 ceftriaxone (9.1%), ceftazidime (3.8%) 및 aztreonam (5.4%), imipenem (4.1%), amikacin (3.3%)은 내성률이 낮았 다. 이는 ampicillin의 내성률이 TMP-SMX보다 높았고 ceftriaxone,
imipenem, amikacin의 경우 항생제 감수성이 90% 이상으로 나타난 이전 연구들과도 일치하는 결과이다. 이러한 항생제 내성률의 차이 로 인하여 3세대 cephalosporin인 ceftriaxon의 치료성공률이 91%인데 반해 ciprofloxacin의 치료성공률은 61%로 나타난 것으로 보인다. CR Table 1. Univariate analysis of risk factors for the detection of ciprofloxacin-resistant Escherichia coli in clinical specimens
Variable Cases (n= 322) Controls (n= 631) Odds ratio
(95% confidence interval) P-value Demographic characteristics
Female gender 188 (58.3) 446 (70.7) 0.620 (0.325-1.184) 0.146
Inpatient source 196 (60.8) 247 (39.2) 2.815 (1.462-5.422) 0.002
Nosocomial 133 (41.3) 90 (14.3) 4.264 (2.336-8.246) 0.001
Previous hospitalization within 90 days 53 (16.3) 28 (4.4) 5.469 (1.277-15.83) 0.002
Age (y) 84± 26.1 64± 21.2 0.001
Acute Physiology and Chronic Health Evaluation II score 30± 9.2 23± 3.6 0.002
Underlying disease
Connective tissue disease 2 (0.6) 24 (3.7) 0.122 (0.046-2.431) 0.287
Malignancy 71 (22.1) 103 (16.3) 2.034 (0.931-4.133) 0.031
Diabetes mellitus 90 (27.8) 170 (27.0) 1.786 (0.314-2.778) 0.798
Cardiac disease 220 (68.3) 178 (28.2) 2.241 (1.112-3.312) 0.032
Chronic obstructive pulmonary disease 11 (3.2) 8 (1.3) 0.623 (0.123-2.442) 0.767
Gastrointestinal disease 68 (21.1) 14 (19.4) 1.824 (0.812-4.344) 0.131
Nephrologic disease 136 (42.2) 272 (43.1) 1.754 (0.923-3.242) 0.009
End-stage renal disease with hemodialysis 18 (5.8) 7 (1.2) 6.222 (0.612-61.49) 0.067
Neurologic disease 136 (42.2) 91 (14.4) 2.631 (1.314-5.177) 0.009
Urologic procedures 136 (42.2) 13 (2.1) 1.000 (0.142-5.623) 1.000
Medical devices
Tract catheterization urinary 234 (72.8) 134 (21.3) 6.411 (3.134-12.41) <0.001
Intravascular catheterization 108 (33.4) 39 (6.2) 5.412 (2.124-15.42) <0.001
Respiratory tract catheterization 66 (20.4) 24 (3.8) 5.241 (1.912-17.53) 0.001
Gastrointestinal tract catheterization 110 (34.2) 45 (7.1) 4.423 (2.042-10.87) <0.001
Antibiotics administration within 2 wk before ciprofloxacins 73 (22.7) 24 (3.8) 7.942 (2.423-25.42) <0.001
Beta-lactams 41 (12.6) 46 (7.3) 1.523 (0.642-4.523) 0.262
Trimethoprim-sulfamethoxazole 10 (3.1) 24 (3.8) 1.000 (0.142-5.631) 1.000
Values are presented as number (%) or mean± standard deviation. Two-tailed chi-square test or Student t-test, as appropriate. Within 2 weeks before urine specimen collection.
Table 2. Multivariate analysis (logistic regression) of risk factors for the emergence of ciprofloxacin-resistant Escherichia coli in clinical specimens
Variable Adjusted odds ratio (95% confidence interval) P-value
Demographic characteristics
Inpatient 1.832 (0.696-4.819) 0.220
Nosocomial 1.011 (0.346-2.957) 0.983
Previous hospitalization within 90 days 3.783 (0.954-14.99) 0.058
Underlying disease
Cardiac disease 1.022 (0.452-2.309) 0.959
Neurological disease 1.531 (0.616-3.806) 0.360
Medical devices
Urinary tract catheterization 2.631 (1.058-6.544) 0.037
Intravascular catheterization 2.805 (0.601-13.08) 0.189
Respiratory tract catheterization 0.763 (0.118-4.914) 0.776
Gastrointestinal tract catheterization 1.358 (0.331-5.562) 0.671
Antibiotics administration within 2 wk before E. coli isolation
Quinolones 13.072 (3.367-50.75) <0.001
최민규 외. 급성신우신염의 Ciprofloxacin 내성 위험인자 Korean Journal of Family Practice
KJFP
에 대해서 다른 항생제에 대한 내성률은 ampicillin (96.1% of isolates), ampicillin-sulbactam (67.3%), amoxicillin-clavulanate (53.2%), TMP/
SMX (93.2%), minocycline (71.2%), chloramphenicol (90.3%), ceftriaxone (31.2%)였다.
CR의 147명은 ciprofloxacin 이외의 하나 이상의 항생제 내성을 갖 고 있었다. 2명은 이들 중 한 개의 항생제 내성을 갖고 있었으며, 6명 은 2개의 추가 항생제 내성, 10명은 3개의 항생제 내성을, 29명은 4개 의 항생제 내성을, 나머지는 5개 이상의 항생제 내성이 있었다. CR 중 10명은 imipenem류에 내성을 가지고 있었다.
고 찰
항생제 내성균주에 의한 감염률의 증가는 계속되어 왔으며, 이는 치료율의 하락으로 이어졌다. 이러한 내성균주에 대한 위험요소를 적절히 판단할 수 있다면 항생제 선택에 있어서 도움이 될 수 있다.
최근 이루어진 외국의 연구들에 의하면 반복적인 급성신우신염에 있어서 4주 이내의 ciprofloxacin 사용의 기왕력이 독립적인 CR의 위 험인자로 보고된 바 있고7) 다른 연구에 의하면 복합적 신우신염이 CR의 위험인자로 결론을 내린 바 있다.8) 또한 Arslan 등8,9)의 연구에 서 보고한 바와 같이 ciprofloxacin 이외의 항생제 사용력은 CR과의 상관관계가 적음을 우리 연구에서도 확인할 수 있었다. Ciprofloxa- cin은 국내에서 TMP/SMX 내성률이 50% 이상으로 보고된 지역사회
내의 급성신우신염에서 추천되는 항생제이다. 하지만 우리 연구에서 는 임상의는 반드시 환자의 약물사용력을 확인 후 항생제를 사용해 야 함을 말해주고 있다. Killgore10)이 보고한 바와 마찬가지로 CR은 다제내성인 가능성이 높음을 우리 연구에서도 결론 내렸다. 이러한 이유로 인해서 ‘ciprofloxacin 사용력이 있는 급성신우신염 환자에 있 어서 3세대 세팔로스포린이 보다 더 추천된다.’라고 보고한 바 있는 Pena 등11)의 연구는 재고될 필요가 있다. 임상의들은 각 지역에 대해 서 급성신우신염의 항생제 내성률을 파악하고 있을 필요가 있으며, 이를 치료에 적극 반영해야 한다.
또한 과도한 항생제 사용은 내성률 상승에 영향을 준다.11,12) 항생 제 종류의 선택 또한 cirofloxacin 내성균주의 출현에 영향을 주는 것 으로 보고되어 있다.13) 같은 맥락에서 무증상 세균뇨가 배양된 도뇨 관 삽입 환자에 있어서 항생제 사용을 자제해야 하는 연구도 있다.14)
결론적으로, 심혈관질환, 신경계질환, 퀴놀론계 항생제 기왕력, 도 뇨관 삽입 등 카테터 유치 환자에 대해서는 ciprofloxacin 내성률 가 능성이 높으며, ciprofloxacin 내성균주인 경우 다른 계열 항생제에 대 한 교차내성을 갖고 있을 가능성이 높으므로 항생제 감수성 결과에 따른 항생제 전환이 반드시 필요하다.
요 약
연구배경:
급성신우신염은 근래에 항생제의 오남용으로 각종 항생 Table 3. Resistance to other antimicrobial agents among ciprofloxacin-resistant and ciprofloxacin-sensitive Escherichia coliAntimicrobial agent No. of resistant isolates (%) Odds ratio
(95% confidence interval) P-value Cases (n= 322) Controls (n= 631)
Penicillins
Ampicillinb 309 (96.1) 529 (83.8) 4.043 (1.123-14.42) 0.020
Ampicillin-sulbactamb 216 (67.3) 166 (26.2) 6.253 (3.234-13.42) <0.001
Amoxicillin-clavulanate 171 (53.2) 140 (22.3) 4.231 (2.342-8.234) <0.001
Piperacillin 136 (42.1) 153 (24.3) 2.532 (1.232-5.534) 0.003
Ticarcillin-clavulanate 109 (33.8) 215 (34.1) 4.532 (2.232-10.23) <0.001
Cephalosporins
Cefmetazole 74 (23.1) 47 (7.4) 4.532 (1.234-10.53) 0.001
Ceftazidime 41 (12.7) 19 (3.1) 3.534 (1.253-13.56) 0.034
Ceftriaxone 100 (31.2) 36 (5.8) 6.657 (2.547-17.67) <0.001
Aztreonam 30 (9.3) 16 (2.3) 5.456 (1.434-28.36) 0.031
Imipenem 10 (3.1) 0 (0.0)
Aminoglycosides
Gentamicin 219 (68.2) 153 (24.2) 5.753 (2.234-11.21) <0.001
Netilmicin 55 (17.2) 33 (5.3) 3.324 (1.534-8.897) 0.013
Amikacin 14 (4.3) 8.9 (1.4) 3.523 (0.534-19.23) 0.213
Trimethoprim-sulfamethoxazole 300 (93.2) 426 (67.3) 5.534 (1.234-14.53) <0.001
Minocycline 229 (71.2) 292 (46.2) 2.435 (1.232-4.434) 0.014
Chloramphenicol 290 (90.3) 339 (53.8) 5.534 (2.234-12.53) <0.001
Two-tailed chi-squared test. Oral form was available in Republic Korea.
Min Kyu Choi, et al. Risk Factors of Ciprofloxacin Resistance – APN
Korean Journal of Family Practice
KJFP
제에 내성균 빈도의 증가와 인체 저항력의 감소 및 병원감염의 증가 로 이에 대한 적극적 예방 및 치료가 요구되고 있다. 본 연구는 Infec- tious Disease Society of America’s Guideline에서 우선적으로 추천되고 있는 ciprofloxacin의 내성균주의 위험인자를 파악함으로써 항생제 선택에 도움을 주고자 하였다.
방법:
2013년 4월 30일부터 1년 동안 김포우리병원 환자들 중 급성신 우신염 중 Escherichia coli가 동정된 모든 환자를 검색하여 데이터화 하였다. E. coli가 동정된 환자들 중 발열이 없거나, 빈뇨, 급박뇨, 하복 부 압통 등 급성신우신염 증상이 없는 환자들은 차트기록 및 경과기 록지 리뷰를 통해 배제시켰다.결과:
최종 연구대상 953명 중 322명이 ciproxacin-resistance (CR)로 확인되어 실험군으로, 631명은 대조군으로 설정되었다. 단변량분석 에서 실험군이 대조군에 비해 통계적 독립인자로 유의성을 갖는 변 수로는 요로관 삽입이 되어있었던 경우(odds ratio [OR], 2.631; 95%confidence interval [CI], 1.058-6.544; P= 0.037), ciprofloxacin 제제가 검 체수집 2주 이내 사용한 적이 있었던 경우(OR, 13.072; 95% CI, 3.367- 50.75; P<0.001)였다. CR 환자군은 imipenem, amikacin을 제외한 다 른 항생제에 있어서 교차내성이 높게 나타났다.
결론:
Ciprofloxacin 사용력, 도뇨관 삽입 등 카테터 유치 환자에 대해 서는 ciprofloxacin 내성률 가능성이 높으며, ciprofloxacin 내성균주인 경우, 다른 계열 항생제에 대한 교차내성을 갖고 있을 가능성이 높으 므로 항생제 감수성 결과에 따른 항생제 전환이 반드시 필요하다.중심단어:
내성균주; 위험인자; 급성신우신염 REFERENCES1. Brenner BM. Brenner & Rector’s the kidney. 8th ed. Philadelphia: WB Saun- ders; 2008.
2. Raz R, Chazan B, Kennes Y, Colodner R, Rottensterich E, Dan M, et al. Em- piric use of trimethoprim-sulfamethoxazole (TMP-SMX) in the treatment of women with uncomplicated urinary tract infections, in a geographical area with a high prevalence of TMP-SMX-resistant uropathogens. Clin Infect Dis
2002;34:1165-9.
3. Ki M, Park T, Choi B, Foxman B. The epidemiology of acute pyelonephritis in South Korea, 1997-1999. Am J Epidemiol 2004;160:985-93.
4. Warren JW, Abrutyn E, Hebel JR, Johnson JR, Schaeffer AJ, Stamm WE.
Guidelines for antimicrobial treatment of uncomplicated acute bacterial cys- titis and acute pyelonephritis in women. Infectious Diseases Society of America (IDSA). Clin Infect Dis 1999;29:745-58.
5. Kim SW, Lee JY, Park WJ, Cho YH, Yoon MS. Antibiotic sensitivity to the causative organism of acute simple urinary tract infection for recent 3 years.
Korean J Infect Dis 2000;32:380-7.
6. Kim JH, Lee CS, Choi NW, Park SK, Lee CH, Kim G, et al. Quinolone resis- tance in community-acquired acute pyelonephritis. Korean J Nephrol 2006;
25:571-8.
7. National Committee for Clinical Laboratory Standards. Performance stan- dards for antimicrobial susceptibility testing: 9th informational supplement.
NCCLS document M100-S9. Wayne (PA): National Committee for Clinical Laboratory Standards; 1999.
8. Arslan H, Azap OK, Ergonul O, Timurkaynak F; Urinary Tract Infection Study Group. Risk factors for ciprofloxacin resistance among Escherichia coli strains isolated from community-acquired urinary tract infections in Turkey.
J Antimicrob Chemother 2005;56:914-8.
9. Ena J, Amador C, Martinez C, Ortiz de la Tabla V. Risk factors for acquisition of urinary tract infections caused by ciprofloxacin resistant Escherichia coli. J Urol 1995;153:117-20.
10. Killgore KM, March KL, Guglielmo BJ. Risk factors for community-acquired ciprofloxacin-resistant Escherichia coli urinary tract infection. Ann Pharma- cother 2004;38:1148-52.
11. Pena C, Albareda JM, Pallares R, Pujol M, Tubau F, Ariza J. Relationship be- tween quinolone use and emergence of ciprofloxacin-resistant Escherichia coli in bloodstream infections. Antimicrob Agents Chemother 1995;39:520- 4.
12. Richard P, Delangle MH, Raffi F, Espaze E, Richet H. Impact of fluoroquino- lone administration on the emergence of fluoroquinolone-resistant gram- negative bacilli from gastrointestinal flora. Clin Infect Dis 2001;32:162-6.
13. Karlowsky JA, Hoban DJ, Decorby MR, Laing NM, Zhanel GG. Fluoroqui- nolone-resistant urinary isolates of Escherichia coli from outpatients are fre- quently multidrug resistant: results from the North American Urinary Tract Infection Collaborative Alliance-Quinolone Resistance study. Antimicrob Agents Chemother 2006;50:2251-4.
14. Hong T, Moland ES, Abdalhamid B, Hanson ND, Wang J, Sloan C, et al.
Escherichia coli: development of carbapenem resistance during therapy. Clin Infect Dis 2005;40:e84-6.