원위 요골 골절과 동반된 척골 골절의 치료
Treatment of Ulnar Fractures Combined with Distal Radius Fracture
김재광 • 김종오 • 윤여헌
이화여자대학교 의학전문대학원 정형외과학교실
원위 요골 골절 중 약 5-6%에서 원위 척골 골절이 동반되는 것으로 알려져 있는데, 고령의 골다공증 환자에서 빈번하다. 원위 요골 골절의 고정 후 원위 척골 골절이 안정된다면 석고 고정만으로 치료도 가능하지만, 원위 척골 골절부에 부정 정렬이 있어나 불안정성이 있을 때는 수술적 치료를 시행한다. 원위 척골 골절의 수술적 방법으로는 K-강선, 골수강 내 금속정, 금속판을 이용한 내고정술과 척골두 절제술이나 Sauve-Kapandji 술식과 같은 구제술 등이 있다. 척골 경상돌기 골절은 약 50%의 원위 요골 골절에서 동반된다. 이 골절은 수술적으로 치 료하지 않으면 약 50-70%에서는 유합되지 않지만, 대부분의 경우에 증상을 유발하지 않는다. 최근 원위 요골 골절 치료로 잠김 금속판을 사용한 문헌 보고들은 척골 경상돌기 골절의 존재나 그 크기가 손목의 기능에 영향을 미치지 않는다고 보고하고 있다.
색인단어: 원위 요골 골절, 원위 척골 골절, 척골 경상돌기 골절
접수일 2013년 1월 31일 수정일 2013년 2월 12일 게재확정일 2013년 2월 20일
교신저자 김재광
서울시 양천구 안양천로 1071, 이화여자대학교 의학전문대학원 목동병원 정 형외과
TEL 02-2650-2591, FAX 02-2642-0349 E-mail kimjk@ewha.ac.kr
Copyright © 2013 by The Korean Orthopaedic Association
“This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.”
대한정형외과학회지:제 48권 제 2호 2013
서 론
척골 골절은 해부학적 위치에 따라 척골 간부 골절, 원위 척골 골 절, 척골 경상 돌기 골절로 분류할 수 있다. 원위 척골 골절은 일 반적으로 척골두에서부터 근위 5 cm까지의 골절을 의미하고,1) 척 골 간부 골절은 이보다 더 근위부 골절을 의미한다. 척골 간부 골 절은 주로 요골 간부 골절과 동반되므로 원위 요골 골절과 동반 되는 경우는 드물다. 또한 척골 간부 골절은 원위 요골 골절의 상 태와 상관 없이 전완부 골절의 치료 원칙에 준하여 치료하여야 한다.
대부분의 원위 척골 골절은 원위 요골 골절과 동반하여 발생 하지만,1) 원위 요골 골절 중 약 5-6%에서만 원위 척골 골절이 동 반되는 것으로 알려져 있다.2) 원위 요골 골절에 원위 척골 골절이 동반되는 경우는 특징적인 나이 분포를 가지고 있는데, 5-14세의
아동기와 65-85세의 골다공증이 동반되는 고령기에 높은 발생 빈도를 보인다.3)
원위 척골은 원위 요골과 함께 원위 요척관절을 형성하여 전 완부의 회전 운동에 있어서 중요한 역할을 한다.4) 또한 원위 척골 골절이나 척골 경상돌기 골절의 부적절한 치료는 원위 요척 관절 의 불안정성이나 원위 요척 관절의 부정 유합에 의한 관절염으로 악력의 약화와 지속적인 척측 손목 통증을 유발할 수 있다.2,5,6) 하 지만 원위 요골 골절에 동반된 척골 골절의 치료 방침은 아직까 지 잘 정립되어 있지 않다. 따라서 최근까지 발표된 연구들을 종 합하여 원위 요골 골절에 동반된 원위 척골 골절이나 척골 경상 돌기 골절을 가지고 있는 성인 환자를 대상으로 적절한 치료 방 법을 알아보고자 한다.
본 론
1. 원위 척골 골절
1) 분류
Biyani 등2)은 원위 척골 골절의 형태에 따라 4가지 형태로 분류하 였는데, Type I은 분쇄가 거의 없는 척골 경부의 단순 관절 외 골
원위 요골 골절 및 동반손상의 치료
절, Type II는 거꾸로 된 T나 Y형태의 골절, Type III는 척골 경부 골절과 척골 경상돌기 골절이 동반된 경우, Type IV는 척골 경부 분쇄 골절이다(Fig. 1). 종합적 분류 체계(comprehensive classifica- tion system)에서는 척골 원위 골절은 Q시스템으로 분류하였다.7) Q1은 척골 경상돌기 기저부 골절이고, Q2는 척골 경부의 단순 골 절, Q3는 척골 경부의 분쇄 골절, Q4는 척골두의 관절 내 골절, Q5 는 척골 경부와 척골두의 동반 골절이다(Fig. 2).
2) 원위 척골 골간단 골절
원위 척골 경부 골절과 그보다 근위부의 원위 척골 골절을 포함 한다. 원위 요골 골절과 원위 척골 골간단 골절이 동반하는 경우 는 고령의 골다공증 환자에서 빈번하다.8) 원위 요골 골절과 동반 된 원위 척골 골간단 골절의 치료는 원위 요골 골절에 대한 치료 가 먼저 시행된 다음 고려한다. 원위 척골이 해부학적인 정복 상 태에서 안정되지 못하면, 전완부의 회전 운동의 장해, 척측 손목 의 지속적인 통증, 원위 요골의 불유합을 유발할 수 있기 때문
에,9,10) 원위 요골 골절의 고정 후 원위 척골 골간단부 골절이 안정
된다면 석고 고정에 의해서 치료하지만, 원위 척골 골간단부에 부정 정렬이 있거나 불안정성이 있을 때는 수술적 치료를 시행한 다.1) 원위 척골 골간단부 골절의 부정 정렬은 10도 이상의 각 형
성, 3 mm 이상의 단축, 골절 면의 1/3 이상의 전위로 정의되고,9) 원위 척골 골간단부 골절의 불안정성은 회내-회외 운동 시 골절 면이 50% 이상 움직이는 것으로 정의된다.11)
원위 척골 골간단부 골절에 대한 수술적 치료 방법은 내고정술 과 구제술로 나눌 수 있다. 원위 척골 골간단부 골절의 내고정 방 법으로는 K-강선, 골수강 내 금속정, 금속판(Fig. 3)이 사용되어 왔다.12) 개방성 정복과 내고정을 시행하면 골절편이 안정되게 고 정되어 조기에 관절 운동을 가능하게 하여야 한다. 하지만 원위 척골 골간단부 골절의 경우는 골다공증성 골절이고, 골편이 작으 며, 약 270도가 관절면으로 싸여 있어 내고정으로 안정된 고정을 얻기가 쉽지 않다. 또한 원위 척골 골간단은 건과 근접해 있기 때 문에 크기가 큰 내고정물은 건염을 유발할 수 있어서 작은 크기 의 내고정물이 사용된다. Ring 등12)은 25명의 환자에서 소형 과칼 날 판(mini-condylar blade plate)을 사용하여 치료하였다. 평균 26 개월 추시상 Gartland and Werley 점수가 6명은 매우 우수, 15명은
Figure 1. Classification of distal ulnar fracture proposed. Cited from the article of Biyani et al. (Fig. 1) with permission.2)
Figure 2. In the comprehensive classifi
cation system, the associated fracture of the distal ulna is classified according to a Q system.
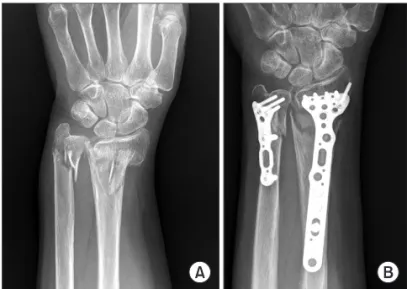
Figure 3. A 74yearold female patient treated with anatomical locking plate fixation for a concomitant distal ulnar metaphyseal fracture. (A) Preoperative radiograph of the wrist. (B) Radiograph taken at three months after surgery.
우수, 4명은 보통이었다. 합병증으로는 2명의 환자에서 원위 요골 골절에 불유합이 있었고, 1명의 환자에서 원위 척골 골절에 불유 합이 있었으며, 7명의 환자는 원위 척골 금속판 때문에 발생한 통 증으로 금속판 제거가 필요하였다. Dennison13)은 5명의 환자에서 2.0 mm의 소형 잠김 금속판(mini-locking plate)을 사용하여 치료 하였다. 평균 12개월 추시에서, 추시상 Gartland and Werley 점수 가 4명은 매우 우수, 1명은 우수였다. 금속판에 의한 불편함 등 추 가적인 수술을 필요로 하는 합병증은 관찰되지 않았다.
원위 척골 골간단부 골절이 골다공증성 분쇄 골절일 경우 해부 학적으로 정복하여 고정하는 것이 매우 힘들고 오히려 합병증을 증가시키기 때문에, 이런 골절을 일차적으로 구제술에 의해 치료 하는 방법들도 사용되었다. Ruchelsman 등9)은 11명의 환자에서 척골 골두 절제술로 치료하였다. 평균 42개월 추시상 Gartland and Werley 점수가 7명은 매우 우수, 4명은 우수였고 추가적인 수술 을 필요로 하는 합병증이 발생하지 않아 만족스러운 치료 방법이 라고 보고하였다. Arora 등14)은 11명의 환자에서 Sauve-Kapandji 방법으로 치료하였다. 평균 46개월 추시상, 전 예에서 원위 요골 과 척골두 간에 불유합은 발생하지 않았고, Green and Obrien 점 수가 8명은 매우 우수, 2명은 우수, 1명은 보통으로 만족스러운 치 료 방법이라고 보고하였다.
고령의 환자에서 원위 척골 골간단 골절은 수술적 치료를 하여 도 해부학적 정복을 얻는 것이 어차피 어렵기 때문에 보존적 방 법을 사용하여도 수술적 치료 방법과 차이가 없다는 연구 결과들 도 있다(Fig. 4).11,15) Namba 등15)은 55세 이상 평균 74세의 원위 요 골 골절과 원위 척골 골간단 골절이 척골두의 관절 내로 침범한 손상을 가진 13명의 환자 14예를 대상으로 한 결과를 보고하였 다. 전례에서 원위 요골 골절은 전방 금속판으로 고정하였고, 원 위 척골 골절은 보존적으로 치료하였다. 평균 18개월 추시 결과 5 예에서 원위 척골 골간단부에 각 변형이 있었지만, 기능 검사상 은 Gartland and Werley 점수가 11예은 매우 우수, 3예는 우수였고 원위 요척관절에 불안정성을 보이는 환자는 없었다고 보고하였
다. Cha 등11)은 65세 이상 고령의 환자에서 원위 요골 골절과 불안 정성 원위 척골 골간단부 골절이 동반된 61명의 환자를 대상으로 연구를 진행하였다. 전례에서 원위 요골 골절은 전방 잠김 금속 판으로 고정하였고, 29명은 원위 척골 골간단부 골절에 대해 금속 판으로 고정하고 32명은 보존적으로 치료하였다. 평균 34개월 추 시상, 악력, visual analogue scale, 손목의 운동 범위, Disabilities of the Arm, Shoulder and Hand 점수와 같은 손목 기능 평가와 방사 선학적 지표에서 양 군 간의 차이는 없었다고 보고하였다.
3) 척골두 골절
척골두 골절 자체가 드물기 때문에 원위 요골 골절과 동반된 척 골두의 관절 내 골절만을 대상으로 해서 연구된 문헌 보고는 아 직까지 없다. 하지만 척골두 단독 골절일 때 전위된 골절들은 개 방성 정복과 머리 없는 유관 압박나사에 치료된 증례 보고들이
있었다.16,17) 따라서 원위 요골 골절과 동반된 척골두 관절 내 골절
이 있더라도 원위 요골 골절의 치료 후 척골두 관절 내 골절이 안 정되고 전위가 없다면, 보존적 방법으로 치료할 수 있고, 척골두 골절이 전위되어 있거나 불안정하다면 개방성 정복과 머리 없는 유관 압박나사로 치료할 수 있을 것으로 생각한다.
대부분의 척골두 골절은 관절면뿐만 아니라 척골 경부나 더 근 위부로 골절이 연장되어 있다. 척골두 골절이 관절 외 골절로 연 장된 경우는 척골두 골절의 관절 내 골편의 전위는 거의 없고 골 절의 불안정성이 대부분 관절 외로 연장된 부분에서 발생하므 로,15) 치료는 원위 척골 골간단 골절의 치료 원칙에 준하여 시행 하면 될 것으로 판단된다.
2. 척골 경상돌기 골절
척골 경상돌기 골절은 약 50%의 원위 요골 골절에서 동반된다.18) 이 골절은 수술적으로 치료하지 않으면 약 50-70%에서는 유합되 지 않지만, 대부분의 경우에 증상을 유발하지 않는다.19) 하지만 몇 몇 예에서 불유합 부위에 통증과 척수근 신근에 건염을 유발시키 Figure 4. A 68yearold female patient who received conservative treatment for a concomitant distal ulnar metaphyseal fracture. (A) Preoperative radiograph of the wrist. (B) Radiograph taken immediately after surgery. (C) Radiograph taken at one year after surgery.
는 증례 보고가 있다.20) 또한 척골 경상돌기 기저부 골절이 있는 경우 원위 요척 관절에 불안정성을 초래할 가능성이 있기 때문에 더 관심을 가져야 한다.
원위 요골 골절에 동반된 척골 경상돌기 골절이 나쁜 영향을 미친다는 문헌 보고는 동반된 척골 경상돌기 골절에 대해 수술적 치료에 대한 주장을 지지하고 있다. Stoffelen 등21)은 척골 경상돌 기 골절이 있는 경우 원위 요척 관절 불안정성을 유발할 수 있기 때문에 Mayo 손목 점수가 더 나쁘다고 보고하였다. Oskarsson 등22) 은 보존적으로 치료한 158명의 원위 요골 골절 환자에서 척골 경 상돌기 골절이 동반된 경우 악력과 손목의 운동 범위가 감소된다 는 것을 발견하였다. May 등23)은 척골 경상돌기 기저부 골절이나 척골 경상돌기 골절이 2 mm 이상 전위된 경우 원위 요척 관절에 불안정성이 유의하게 더 잘 발생한다고 하였다.
하지만 최근 원위 요골 골절 치료로 잠김 금속판을 사용한 문 헌 보고들은 척골 경상돌기 골절의 존재나 그 크기가 손목의 기 능에 영향을 미치지 않는다고 보고하고 있다.18,24,25) 최근 원위 요 골 골절 치료 방법으로 많이 사용되는 개방성 정복 및 금속판 고 정술은 골다공증성 환자에서도 원위 요골을 비교적 해부학적 상 태에서 유합을 얻을 수 있게 한다.26) 이것은 전위된 척골 경상돌 기를 간접적으로 정복시키고, 원위 요척 관절의 불안정성이 원위 요골의 부정 유합에 의해서 발생하는 것을 막는 효과를 가져왔 다.18) 또한 순수하게 척골 경상돌기 골절에 의한 영향만을 반영할 수 있게 한다.
원위 요골 골절이 해부학적으로 정복되고 안정되게 고정된 경 우, 원위 요척 관절에 불안정성이 없으면 척골 경상돌기 골절에 대한 수술을 하지 않는 것에 대해서는 의견의 일치가 있다. 드물 지만 원위 요척 관절에 불안정성이 있으면서 척골 경상돌기 기저 부 골절이 있는 경우에 대해서는 아직까지 이견이 있다. 어떤 저 자들은 척골 경상돌기 골절에 대해 수술적 치료를 하여야 한다고 주장한다.27) 하지만 다른 저자들은 그런 경우도 4주 정도의 고정 으로도 장기적으로 좋은 결과를 보이기 때문에,18) 척골 신경 후방 분지 손상이나 금속 핀에 의한 통증의 위험성을 감수하면서 수술 을 하는 것에 반대하는 의견도 있다.
결 론
원위 요골 골절과 동반된 원위 척골 골절이나 척골 경상돌기 골 절은 원위 요척 관절의 기능이나 불안정성에 영향을 미칠 수 있 다. 원위 요골 골절에 대한 치료가 먼저 시행된 다음 원위 척골 골 절의 부정 정렬과 불안정성 정도를 고려하여 치료 방법을 결정한 다. 원위 요골 골절의 해부학적 정복이 원위 척골이나 척골 경상 돌기 골절의 정복과 안정성을 가져올 수 있기 때문에 보존적 방 법이 우선적 치료 방법으로 고려되어야 할 것으로 생각한다.
참고문헌
1. Logan AJ, Lindau TR. The management of distal ulnar frac- tures in adults: a review of the literature and recommenda- tions for treatment. Strategies Trauma Limb Reconstr. 2008;3:
49-56.
2. Biyani A, Simison AJ, Klenerman L. Fractures of the distal ra- dius and ulna. J Hand Surg Br. 1995;20:357-64.
3. Gschwentner M, Arora R, Wambacher M, Gabl M, Lutz M.
Distal forearm fracture in the adult: is ORIF of the radius and closed reduction of the ulna a treatment option in distal fore- arm fracture? Arch Orthop Trauma Surg. 2008;128:847-55.
4. Kapandji A. Biomechanics of pronation and supination of the forearm. Hand Clin. 2001;17:111-22.
5. Lindau T, Adlercreutz C, Aspenberg P. Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg Am.
2000;25:464-8.
6. Zimmerman RM, Kim JM, Jupiter JB. Arthritis of the distal radioulnar joint: from Darrach to total joint arthroplasty. J Am Acad Orthop Surg. 2012;20:623-32.
7. Müller ME, Nazarian S, Koch P, Schatzker J, Heim U. The comprehensive classification of fractures of long bones. Ber- lin: Springer-Verlag; 1990. 106-15.
8. Jupiter JB, Marent-Huber M; LCP Study Group. Operative management of distal radial fractures with 2.4-millimeter locking plates. A multicenter prospective case series. J Bone Joint Surg Am. 2009;91:55-65.
9. Ruchelsman DE, Raskin KB, Rettig ME. Outcome following acute primary distal ulna resection for comminuted distal ulna fractures at the time of operative fixation of unstable fractures of the distal radius. Hand (N Y). 2009;4:391-6.
10. McKee MD, Waddell JP, Yoo D, Richards RR. Nonunion of distal radial fractures associated with distal ulnar shaft frac- tures: a report of four cases. J Orthop Trauma. 1997;11:49-53.
11. Cha SM, Shin HD, Kim KC, Park E. Treatment of unstable distal ulna fractures associated with distal radius fractures in patients 65 years and older. J Hand Surg Am. 2012;37:2481-7.
12. Ring D, McCarty LP, Campbell D, Jupiter JB. Condylar blade plate fixation of unstable fractures of the distal ulna associated with fracture of the distal radius. J Hand Surg Am. 2004;29:
103-9.
13. Dennison DG. Open reduction and internal locked fixation of unstable distal ulna fractures with concomitant distal radius
fracture. J Hand Surg Am. 2007;32:801-5.
14. Arora R, Gabl M, Pechlaner S, Lutz M. Initial shortening and internal fixation in combination with a Sauvé-Kapandji pro- cedure for severely comminuted fractures of the distal radius in elderly patients. J Bone Joint Surg Br. 2010;92:1558-62.
15. Namba J, Fujiwara T, Murase T, Kyo T, Satoh I, Tsuda T. Intra- articular distal ulnar fractures associated with distal radial fractures in older adults: early experience in fixation of the ra- dius and leaving the ulna unfixed. J Hand Surg Eur Vol. 2009;
34:592-7.
16. Jakab E, Ganos DL, Gagnon S. Isolated intra-articular fracture of the ulnar head. J Orthop Trauma. 1993;7:290-2.
17. Solan MC, Rees R, Molloy S, Proctor MT. Internal fixation af- ter intra-articular fracture of the distal ulna. J Bone Joint Surg Br. 2003;85:279-80.
18. Kim JK, Koh YD, Do NH. Should an ulnar styloid fracture be fixed following volar plate fixation of a distal radial fracture? J Bone Joint Surg Am. 2010;92:1-6.
19. Kim JK, Yun YH, Kim DJ, Yun GU. Comparison of united and nonunited fractures of the ulnar styloid following volar- plate fixation of distal radius fractures. Injury. 2011;42:371-5.
20. Hauck RM, Skahen J 3rd, Palmer AK. Classification and treat- ment of ulnar styloid nonunion. J Hand Surg Am. 1996;21:
418-22.
21. Stoffelen D, De Smet L, Broos P. The importance of the dis-
tal radioulnar joint in distal radial fractures. J Hand Surg Br.
1998;23:507-11.
22. Oskarsson GV, Aaser P, Hjall A. Do we underestimate the pre- dictive value of the ulnar styloid affection in Colles fractures?
Arch Orthop Trauma Surg. 1997;116:341-4.
23. May MM, Lawton JN, Blazar PE. Ulnar styloid fractures as- sociated with distal radius fractures: incidence and implica- tions for distal radioulnar joint instability. J Hand Surg Am.
2002;27:965-71.
24. Souer JS, Ring D, Matschke S, Audige L, Marent-Huber M, Jupiter JB; AOCID Prospective ORIF Distal Radius Study Group. Effect of an unrepaired fracture of the ulnar styloid base on outcome after plate-and-screw fixation of a distal ra- dial fracture. J Bone Joint Surg Am. 2009;91:830-8.
25. Zenke Y, Sakai A, Oshige T, Moritani S, Nakamura T. The ef- fect of an associated ulnar styloid fracture on the outcome af- ter fixation of a fracture of the distal radius. J Bone Joint Surg Br. 2009;91:102-7.
26. Orbay JL, Fernandez DL. Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg Am. 2004;29:96-102.
27. Sammer DM, Chung KC. Management of the distal radioul- nar joint and ulnar styloid fracture. Hand Clin. 2012;28:199- 206.
Treatment of Ulnar Fractures Combined with Distal Radius Fracture
Jae Kwang Kim, M.D., Ph.D., Jong-Oh Kim, M.D., Ph.D., and Yeo-Hon Yun, M.D., Ph.D.
Department of Orthopedic Surgery, Ewha Womans University School of Medicine, Seoul, Korea
Approximately 5-6% of distal radius fractures have a concomitant distal ulnar fracture, this incidence is more frequent in osteoporotic elderly patients. When the distal ulnar fracture is stable after fixation of the distal radius fracture, the distal ulnar fracture can be managed with cast immobilization. However, when the distal ulnar fracture shows malalignment or instability, an operative method should be used. The operative method for distal ulnar fracture includes internal fixation using a K-wire, intramedullary nail, or plates and salvage procedures including ulnar head resection or Sauve-Kapandji procedure. Approximately 50% of distal radius fractures are combined with ulnar styloid process fracture. Although approximately 50-70% of ulnar styloid process fractures result in nonunion if they are not treated by an operative method, they tend to be asymptomatic. Recent studies of distal radius fracture treated using a volar locking plate have generally reported that neither the presence nor the size of concomitant ulnar styloid fracture has an effect on clinical outcome.
Key words: distal radius fracture, distal ulnar fracture, ulnar styloid process fracture
Received January 31, 2013 Revised February 12, 2013 Accepted February 20, 2013 Correspondence to: Jae Kwang Kim, M.D., Ph.D.
Department of Orthopedic Surgery, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, 1071 Anyangcheon-ro, Yangcheon-gu, Seoul 158-710, Korea
TEL: +82-2-2650-2591
FAX: +82-2-2642-0349 E-mail: kimjk@ewha.ac.krCopyright © 2013 by The Korean Orthopaedic Association
“This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.”
The Journal of the Korean Orthopaedic Association Volume 48 Number 2 2013