접수: 2020년 2월 10일, 승인: 2020년 2월 28일 연락처: 정선영, 06974, 서울시 동작구 흑석로 84
중앙대학교 약학대학
Tel: (02) 820-5678, Fax: (02) 816-7338 E-mail: [email protected]
Correspondence to: Sun-Young Jung, PhD
College of Pharmacy, Chung-Ang University, 84 Heukseok-ro, Dongjak-gu, Seoul 06974, Korea
Tel: +82-2-820-5678, Fax: +82-2-816-7338 E-mail: [email protected]
폐렴구균 백신 접종 후 자발적 부작용 보고자료를 이용한 백신 실마리정보 검색 방법론 비교
중앙대학교 약학대학
유승훈ㆍ김묘송ㆍ이민택ㆍ강예진ㆍ정선영
Comparison of Signal Detection Methodologies Using the Korean Spontaneous Adverse Event Reports after Pneumococcal Vaccination
Seung-Hun You, BS, Myo-Song Kim, BPharm, Min-Taek Lee, BS, Ye-Jin Kang, BS and Sun-Young Jung, PhD
College of Pharmacy, Chung-Ang University, Seoul, Korea
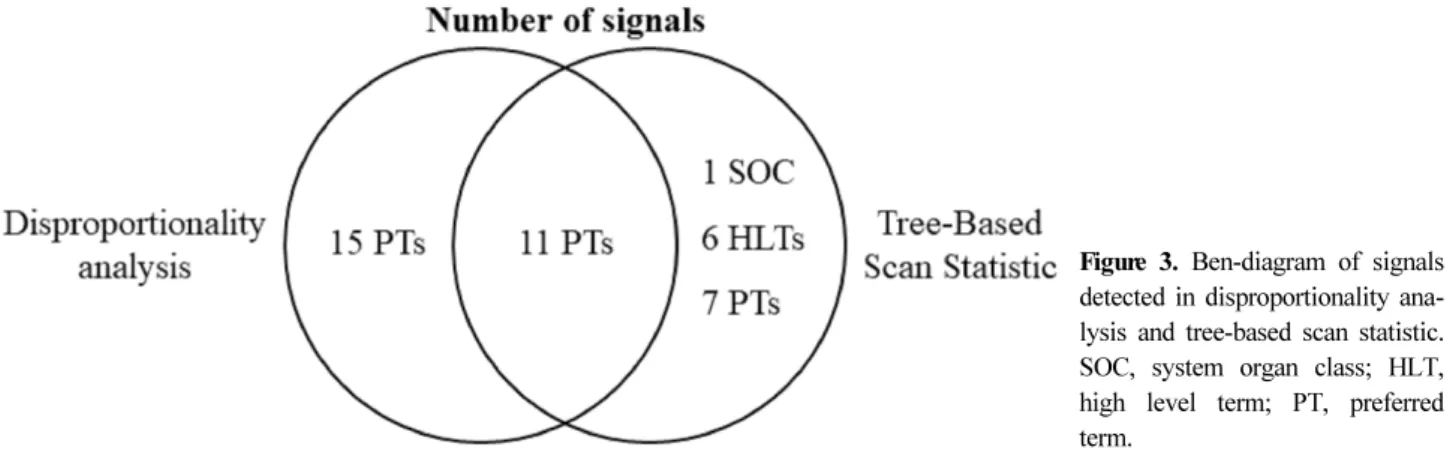
Objective: To compare vaccine signal detection methodologies using the Korea adverse events reporting system (KAERS) database for vaccines. Methods: Among the individual case safety reports (ICSRs) reported to KAERS data- base between 2005 and 2017, the vaccines of interest were pneumococcal conjugate vaccine (WHO-ATC, J07AL01) and pneumococcal polysaccharide vaccine (J07AL02). To derive safety signals, we applied disproportionality analysis and tree-based scan statistic (TBSS). The disproportionality analysis calculated three indices (proportional reporting ratio, re- porting odds ratio, and information component) based on the reported preferred terms (WHO-ART, PT). TBSS calcu- lated the log-likelihood ratio and was validated by Monte Carlo simulation based on the reported all hierarchical level term. Then we examined whether the safety signals were listed in the drug label. Results: Among total of 29,270 vac- cine ICSRs in KAERS database, the number of ICSRs of pneumococcal vaccines was 5,738. The disproportionality analysis yielded 26 PTs as safety signals and detected unlabeled 6 PTs including ‘medicine ineffectiveness’. The TBSS yielded 25 as hierarchy level statistical signals and detected for unlabeled 5 hierarchy level including ‘pneumonia’ and
‘medicine ineffectiveness’. Conclusion: The number of adverse events (AEs) reporting on pneumococcal vaccines in- creased following introduction to the Korean national immunization program. The derived safety signals such as
‘medicine ineffective’ and ‘pneumonia’ may be due to comorbid conditions of vaccine recipients high-risk of infection, which warrants further study. Along with disproportionality analysis, TBSS could be used as a supplementary tool for signal detection with analyzing all-level hierarchical structural term AEs. (JPERM 2020;12:44-52)
Key Words: Vaccines; Signal detection analyses; Data mining; Adverse drug events
서 론
백신은 안전하고 효과적으로 설계되었지만, 시판 전 임상시험
에서 발견되지 않은 이상사례가 시판 후 대규모 인구집단에서
발생할 수 있으므로 백신의 안전성을 확신할 수 없다.
1,2)따라
서 시판 후 백신의 안전성에 대해서 평가 및 감시하여 대중의
신뢰를 얻고 유지해야 한다.
3)우리나라는 감염병을 예방하기 위해 국가예방접종프로그램(National Immunization Program, NIP) 을 시행하고 있으며, 그 중 폐렴구균 백신은 다당백신 (Pneumococcal polysaccharide vaccine, PPSV) 과 단백결합백신 (Pneumococcal conjugate vaccine, PCV) 으로 나누어 접종을 하 고 있다. 다당백신은 2세 이상 고위험군인 소아청소년과 성인 및 65세 이상의 노인을 대상으로 2013년 5월 국가예방접종프 로그램에 도입되었으며, 단백결합백신은 19세 미만 소아청소년 및 면역저하상태 등 기저질환이 있는 19세 이상의 성인을 대상 으로 2014년 5월 국가예방접종프로그램에 도입되었다.
4)비교적 최근 국가예방접종프로그램에 도입된 폐렴구균 백신의 안전성 정보가 부족하다.
약물감시분야에서 백신의 안전성 정보를 평가하기 위한 방법 으로 실마리정보 검색이 있으며, 응용사례로 자발적 보고자료 를 이용하여 인유두종바이러스 백신의 추가 이상사례로 여성의 생식기증 장애 등이 검색되어 허가사항이 변경된 바 있다.
5)이 처럼 실마리정보 검색을 통해 백신의 안전성 정보를 조기에 발 견할 수 있다.
자발적 이상사례 보고로부터 실마리정보를 검색하는 방법 중 가장 널리 사용되는 것은 불균형 분석(Disproportionality analy- sis) 으로, 유럽의약품청(European Medicines Agency, EMA) Eudravigilance (European Union Drug Regulating Authorities Pharmacovigilance) 에서 사용하는 보고분율비(Proportional Re- porting Ratio, PRR)
6)와 네덜란드의 Lareb에서 사용하는 보고오 즈비(Reporting Odds Ratio, ROR)
7)와 세계보건기구(World Health Organization, WHO) 의 WHO-Vigibase에서 사용되는 베 이지안신뢰전달신경망(Bayesian Confidence Propagation Neural Network, BCPNN) 의 정보성분(Information Component, IC)
8)이 대표적인 방법론으로 사용되고있다. 불균형분석을 백신에 적용 한 사례는 2008년부터 2017년까지 SAEFVIC (Surveillance of Adverse Events Following Vaccination In the Community) 의 예방접종 후 이상사례 데이터베이스에서 PRR 지표를 활용하여 인플루엔자 백신의 안전성 조사
9)와 2007년부터 2017년까지 미 국의 VAERS (Vaccine Adverse Event Reporting System) 데이 터베이스에서 ROR 지표를 활용하여 인유두종 바이러스 백신 (Human papilloma virus, HPV) 의 안전성 조사
10)를 하였으며, 2008 년부터 2013년까지 CNAEFIS (Chinese National AEFI Information System) 데이터베이스에서 IC를 포함한 지표를 활 용하여 일본 뇌염 백신의 안전성에 대해서 조사한 바 있다.
11)트리 기반 통계적 검색(Tree-Based Scan Statistic, TBSS)은 계층적 트리 구조를 형성하는 데이터베이스를 감시하기 위해 제안되었으며, 다수의 잠재적 이상사례와 그룹화한 이상사례를 동시에 평가할 수 있다.
12,13)트리 기반 통계적 검색 방법을 백 신에 적용한 사례로 Li 등은 2005년부터 2014년 미국 질병관리 본부(Centers for Disease Control and Prevention, CDC)의 6개
백신안전성데이터링크(Vaccine Safety Datalink, VSD)를 이용 하여 수막구균 결합백신(Meningococcal conjugate vaccine)의 안전성에 대하여 조사한 바 있다.
14)이 방법은 백신등록자료와 의료이용자료 간 연계자료에서 적용된 사례는 다수 있으나, 자 발적 이상사례 보고자료를 이용한 실마리정보 도출 방법론은 적용된 경우가 드물었다.
본 연구는 국내 백신 접종 후 이상사례 보고자료를 이용하여 실마리정보 검색을 위한 불균형 분석과 트리 기반 통계적 검색 방법론의 특장점을 비교하고자 수행되었다.
대상 및 방법 1. 연구자료
한국의약품안전관리원의 의약품부작용보고시스템(Korea Adverse Event Reporting System, KAERS) 에 자발적 보고된 개별이상사 례보고(Individual Case Safety Reports, ICSRs)를 데이터화한 의약품부작용보고원시자료(Korea Institute of Drug Safety KAERS Database, KIDS-KD) 를 사용하였다. KIDS-KD는 보고 자의 기본정보(성별, 연령 등), 의약품정보(투여일, 성분명 등), 부작용정보(부작용코드, 부작용일 등), 중대사례정보(중대한 부 작용 유형), 보고자정보(원보고자자격, 보고기관구분), 평가정보 ( 인과성평가 결과), 병력정보(병력), 그룹정보(최초추적그룹정 보)로 구성되어 있다.
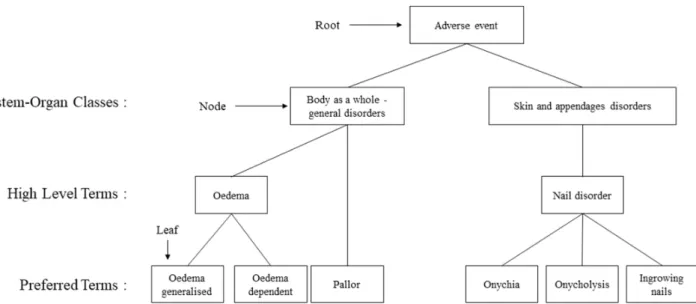
15)KIDS-KD 의 부작용정보는 WHO의 웁 살라모니터링센터에서 개발한 부작용 코드 체계 WHO-ART (World Health Organization Adverse Reaction Terminology) 로 기록되어 있으며, WHO-ART는 신체기관계분류(System-Organ Classes, SOC), 상위용어(High Level Terms, HLT), 우선순위용 어(Preferred Terms, PT), 하위포함용어(Included Terms, IT)의 4 개의 계층(hierarchy) 구조로 구성되어 있다.
16)2. 연구대상백신
2005 년부터 2017년까지 KAERS에 ATC (Anatomical Thera- peutic Chemical) 코드가 J07 (백신류), L03AX03 (BCG vac- cine), L03AX12 (melanoma vaccine) 로 보고된 30,408건의 보고 서를 기반으로 분석하였으며, 관심 백신은 폐렴구균 백신인 단 백결합백신(WHO-ATC, J07AL02)과 다당백신(J07AL01)으로 선정하였다.
본 연구는 중앙대학교 생명윤리위원회 검토 결과 심의면제 승인을 받았다(1041078-201903-HR-071-01).
3. 통계분석 1) 데이터 전처리
KIDS-KD 는 개별 이상사례 보고서의 추가 정보를 기입하는
추적보고 기능을 갖추고 있어, 동일한 백신과 이상사례가 중복
보고될 수 있으며, 본 연구에서는 추적보고의 마지막 보고서를
Figure 1. Example of a small four‐level tree variable, tree-based scan statistic for the current study.
Table 1. Definition and signal detection criteria of implemented data mining indices
Indices Definition Criteria of signal detection DA PRR P(AE
빳drug)/P(AE
빳drug*) PRR ≥2, chi-squared≥4 and number of report≥3
ROR ROR ≥2, chi-squared≥4 and number of report≥3 IC
IC under limit of 95% confidence interval ≥0
TBSS RR
p-value of LLR ≤0.05, LLR =
DA, disproportionality analysis; TBSS, tree-based scan statistic; Drug, suspected drug; drug*, other drug; AE, suspected adverse event; AE*, other suspected adverse event; n, total number of vaccine-AE; PRR, proportional reporting ratio; ROR, reporting odds ratio; IC, information component; RR, relative risk; LLR, log-likelihood ratio.
기준으로 분석하였다. 하나의 보고서 내 여러 백신과 이상사례 가 존재하는 경우 여러 백신과 이상사례의 인과성을 고려하여 백신 투여 후 발생한 이상사례를 조합하였으며, 논리적 오류는 제거하였다. 예를 들어 개별 이상사례 보고서로 A 백신 접종 후 2개의 이상사례가 발생하였고, 이후에 B 백신 접종 후 1개 의 이상사례가 발생하였다고 보고되었다. 하지만 보고 후 추가 로 1개의 이상사례가 발생하여 추적보고한 경우 새로운 개별 이상사례 보고서로 A, B 백신과 이상사례 4개가 보고된다. 최 종 보고서 기준으로 A 백신과 이상사례 2개, B 백신과 이상사 례 2개를 조합하여, 백신-이상사례의 조합을 4건으로 정의하였다.
2) 폐렴구균 백신 접종 후 이상사례 보고의 특성 분석 폐렴구균 백신과 그 외 다른 백신에 대한 개별 이상사례 보 고건의 보고자 연령, 성별과 보고연도, 보고유형 등 보고자와
보고서의 특성을 확인하고 두 그룹간 동질성 여부를 파악하기 위해 카이제곱 검정(chi-squared test)을 하였다.
3) 실마리정보 검색
(1) 불균형 분석(Disproportionality analysis): 불균형 분 석의 대표적인 지표로 PRR, ROR, IC가 사용되고 있다. PRR은 관심 백신에 의한 이상사례 보고건 중 관심 이상사례가 차지하 는 분율을 그 외 백신에 의한 이상사례 보고건 중 관심 이상사 례가 차지하는 분율로 나눈 값이다. ROR은 관심 백신에 의해 발생한 관심 이상사례의 오즈를 그 외 백신에 의해 발생한 관 심 이상사례의 오즈로 나눈 값이다. IC는 관심 백신으로 인한 관심 이상사례가 발생할 확률을 관심 백신의 복용확률과 관심 이상사례의 발생확률의 곱으로 나누어 로그를 취한 값이다.
일반적으로 PRR의 경우 PRR≥2이고 chi-squared≥4이면서
Figure 2. Flow diagram of indivi- dual case safety reports (ICSRs).
PCV, pneumococcal conjugate vac- cine; PPSV, pneumococcal poly- saccharide vaccine; AEs, adverse events.
이상사례 보고건수≥3,
6)ROR 인 경우 ROR≥2이고 chi-squared
≥4이면서 이상사례 보고건수≥3,
7)IC 인 경우 95% 신뢰구간의 하한치가 0이상
8)이면 실마리정보로 간주한다(표 1). 본 연구에 서는 PRR, ROR, IC의 실마리정보 판정기준을 모두 만족하면 백신-이상사례의 실마리정보로 정의하였다.
(2) 트리 기반 통계적 검색(Tree-Based Scan Statistic):
트리 기반 통계적 검색은 계층적 구조를 가진 데이터분석에서 유용하며 각 노드와 잎에서의 초과 위험(excess risk)을 찾는 데 이터마이닝 방법론이다(그림 1).
13)트리 기반 통계적 검색은 포 아송분포, 이항분포 등 사용된 확률분포에 따라 기대값(The number of expected) 과 상대위험비(relative risk)를 도출한다.
17)검정통계량은 로그가능도함수(Log Likelihood Ratio, LLR)로 계산되며, 몬테카를로 시뮬레이션(Monte-Carlo Simulation)을 이용하여 귀무가설 가정하에 무작위 추출된 데이터를 기반으로 검정통계량의 분포를 파악하고 p-value를 도출한다.
12,18)본 연구에서는 표준 이항분포 모델을 적용하였으며, 기대값 은 각 노드와 잎에서의 이상사례 보고건을 관심 백신의 이상사 례가 발생할 확률을 곱한 값이고, 상대위험비는 각 노드와 잎에 서 관심 백신에 의한 이상사례 보고건을 기대값으로 나눈 값이 다(표 1). 실마리정보 판정기준은 검정통계량값이 유의수준 5%
하에서 유의한 경우 백신-이상사례의 실마리정보로 정의하였다.
(3) 검색된 실마리정보 확인: 불균형 분석의 이상사례 분석 단위를 우선순위용어로 정의하여 검색된 실마리정보와 트리 기 반 통계적 검색의 이상사례 분석단위를 신체기관계분류, 상위 용어, 우선순위용어 3단계 계층 구조로 정의하여 검색된 실마 리정보에 대해서 식품의약품안전처의 사용상의 주의사항 포함
여부를 확인하였다. 본 연구에서 통계분석은 SAS 9.4 (SAS Institute Inc., Cary, NC) 와 TreeScan v1.4 (released June 2018) 를 이용하였다.
결 과
2005 년부터 2017년까지 한국의약품안전관리원의 KAERS에 보고된 백신 접종 후 이상사례 보고건은 30,408건이었으며, 추 적보고인 경우 가장 마지막 보고서를 기준으로 유지하고 논리 적 오류를 제외한 결과 30,408건 중 1,138건이 제외되어 29,270 건이 되었다. 그 중 이상사례는 57,589건이고 백신-이상사례의 조합은 85,514건이었다(그림 2).
29,270 건 중 폐렴구균 백신을 포함한 보고는 5,738건(19.6%) 이었으며, 백신-이상사례의 조합은 13,175건이었다. 보고자 성 별의 비율은 남성이 44.2%로 다른 백신에 비해 많았으며, 연령 은 24개월 미만과 64세 이상에서 많았다. 보고연도는 2013- 2017 년이 90.1%를 차지하였으며, 보고유형은 재심사를 포함한 조사연구가 52.2%로 가장 많았고, 이어서 자발적보고로 46.1%
보고되었다. 원보고자는 의료종사자가 77.9%로 가장 많이 차지
하였고, 보고기관은 제약회사에서 77.2%로 가장 많이 보고되었
다. 성별, 연령, 보고연도, 보고유형, 원보고자, 보고기관은 폐렴
구균 백신과 그 외 다른 백신 간 통계적으로 유의한 차이가 있
었다. 중대한 이상사례인 경우는 448건(7.8%)이며, 그 중 입원
또는 입원기간 연장이 299건, 기타 의학적으로 중요한 상황
138 건, 사망 27건, 중대한 불구나 기능저하 7건, 생명의 위협 4
건 보고되었다. 중대한 이상사례는 폐렴구균 백신과 그 외 다른
Table 2. Characteristics of individual case safety reports, pneumococcal vaccine and other vaccine
Characteristics
Total vaccine (N=29,270)
PCV, PPSVvaccine (N=5,738)
Other vaccine
(N=23,532) p-value
N (%) N (%) N (%)
Sex <.0001
Male 10,152 (34.7) 2,537 (44.2) 7,615 (32.4)
Female 17,890 (61.1) 2,923 (50.9) 14,967 (63.6)
Unknown 1,228 (4.2) 278 (4.9) 950 (4)
Age <.0001
<28 days 1,068 (3.6) 439 (7.7) 629 (2.7)
28 days-24 months 3,271 (11.2) 1,037 (18.1) 2,234 (9.5) 24 months-11 years old 2,355 (8.1) 179 (3.1) 2,176 (9.2) 12-18 years old 1,911 (6.5) 19 (0.3) 1,892 (8) 19-64 years old 9,942 (34) 915 (15.9) 9,027 (38.4)
>64 years old 1,738 (5.9) 516 (9) 1,222 (5.2)
Unknown 8,985 (30.7) 2,633 (45.9) 6,352 (27)
Year report was received <.0001
2005-2008 276 (0.9) 89 (1.6) 187 (0.8)
2009-2012 3,437 (11.7) 475 (8.3) 2,962 (12.6)
2013-2017 25,557 (87.4) 5,174 (90.1) 20,383 (86.6)
Report type <.0001
Spontaneous report 13,296 (45.4) 2,645 (46.1) 10,651 (45.3) Research (including PMS) 15,387 (52.6) 2,994 (52.2) 12,393 (52.7)
Literature 204 (0.7) 12 (0.2) 192 (0.8)
Others 383 (1.3) 87 (1.5) 296 (1.2)
Original reporter <.0001
Healthcare professionals 18,969 (64.8) 4,472 (77.9) 14,497 (61.6)
Consumers 2,127 (7.3) 326 (5.7) 1,801 (7.6)
Others 4,339 (14.8) 795 (13.9) 3,544 (15.1)
Unknown 3,835 (13.1) 145 (2.5) 3,690 (15.7)
Reporter <.0001
Regional pharmacovigilance centers 5,693 (19.4) 812 (14.2) 4,881 (20.7) Manufacturer (including importers) 21,082 (72) 4,433 (77.2) 16,649 (70.8) Medical institution 360 (1.3) 26 (0.5) 334 (1.4)
Pharmacy 4 (0) 1 (0) 3 (0)
Community health center 62 (0.2) 46 (0.7) 16 (0.1)
Consumer 422 (1.5) 72 (1.3) 350 (1.5)
Others 1,647 (5.6) 348 (6.1) 1,299 (5.5)
Serious adverse event 0.3335
Yes 2,197 (7.5) 448 (7.8) 1,749 (7.4)
No 27,073 (92.5) 5,290 (92.2) 21,783 (92.6)
Serious adverse event category 0.2757
Significant disability/incapacity 27 (0.1) 7 (0.1) 20 (0.1)
Life threatening 23 (0.1) 4 (0.1) 19 (0.1)
Died 143 (0.5) 27 (0.5) 116 (0.5)
Hospitalization 1,390 (4.7) 299 (5.2) 1,091 (4.6) Important medical event 776 (2.7) 138 (2.4) 638 (2.7)
PCV, pneumococcal conjugate vaccine; PPSV, pneumococcal polysaccharide vaccine; PMS, post marketing surveillance.
백신 간 통계적으로 유의한 차이가 없었다(표 2).
불균형분석의 지표인 PRR, ROR, IC 모두 만족하는 이상사 례로 국소피부반응, 운동이상증, 연조직염 등 26개의 우선순위
용어가 검색되었다. 그 중 식품의약품안전처의 허가사항에 반
영되지 않은 이상사례는 구강건조, SGOT 증가, 심장판막질환,
심정지, 객혈, 효과 없는 약이었다. 트리 기반 통계 검색에서 통
Table 3. Detected signals of pneumococcal vaccine fulfilling the criteria for disproportionality analysis and tree-based scan statistic
Adverse event Pneumococcal/
Other vaccine
Disproportionality analysis Tree-based scan statistic
MFDS PRR ROR IC
025χ
2Expected Relative
risk p-value
#
Skin and appendages disorders
†
Skin reaction localized 12/17 3.88 3.88 1.49 15.02 Labeled
†
Livedo reticularis 8/13 3.38 3.38 1.41 8.30 Labeled
†
Angioedema 16/37 2.37 2.38 1.03 8.89 Labeled
†
Rash 257/1,007 194.74 1.32 0.001 Labeled
*Rash 352/1,423 273.47 1.29 0.001 Labeled
#
Collagen disorders
†
Le syndrome 9/15 3.29 3.30 1.38 8.99 Labeled
#
Central & peripheral nervous system disorders
†
Dyskinesia 32/39 4.51 4.51 1.57 47.98 10.94 2.93 0.001 Labeled
*Dyskinesia 64/90 23.73 2.7 0.001 Labeled
†
Hypokinesia 32/51 3.45 3.45 1.35 34.16 12.79 2.5 0.001 Labeled
#
Gastro-intestinal system disorders
†
Mouth dry 5/8 3.43 3.43 1.48 5.30 Unlabeled
#
Liver and biliary system disorders
†
SGOT increased 8/18 2.44 2.44 1.11 4.71 Unlabeled
#
Myo-, endo-, pericardial & valve disorders
†
Heart valve disorders 5/8 3.43 3.43 1.48 5.30 Unlabeled
#
Heart rate and rhythm disorders
†
Cardiac arrest 4/5 4.39 4.39 1.70 5.82 Unlabeled
#
Respiratory system disorders 3,601/17,224 3208.47 1.12 0.001 Labeled
†
Haemoptysis 4/1 21.96 21.97 2.44 16.01 Unlabeled
†
Respiratory disorder 45/89 2.78 2.78 1.14 34.02 20.65 2.18 0.001 Labeled
†
Pulmonary disorders 4/0 0.62 6.49 0.03 Unlabeled
†
Pneumonia 450/1,649 323.39 1.39 0.001 Unlabeled
*Pneumonia 452/1,662 325.7 1.39 0.001 Unlabeled
†
Upper respiratory tract infection 810/3,229 622.28 1.3 0.001 Labeled
*Upper respiratory tract infection 2,273/11,058 2053.89 1.11 0.001 Labeled
#
White cell and res* disorders
†
Leukocytosis 11/9 6.71 6.72 1.89 24.06 3.08 3.57 0.011 Labeled
#
Urinary system disorders
†
Micturition frequency 3/1 16.47 16.48 2.38 10.90 Labeled
†
Oliguria 4/2 10.98 10.98 2.21 12.10 Labeled
†
Face oedema 14/38 2.02 2.02 0.88 5.30 Labeled
#
Foetal disorders
†
Naevus 3/2 8.24 8.24 2.11 7.63 Labeled
#
Body as a whole-general disorders
†
C-reactive protein increased 6/1 32.94 32.96 2.51 26.55 1.08 5.56 0.009 Labeled
†
Medicine ineffective 26/29 4.92 4.93 1.65 42.88 8.47 3.07 0.001 Unlabeled
*Medicine ineffective 26/29 8.47 3.07 0.001 Unlabeled
†
Temperature changed sensation 26/45 3.17 3.18 1.28 24.53 10.94 2.38 0.004 Labeled
†
Oedema peripheral 40/94 2.34 2.34 0.98 21.48 20.65 1.94 0.007 Labeled
†
Crying abnormal 96/228 2.31 2.32 0.95 50.48 49.92 1.92 0.001 Labeled
†
Fever 1,183/4,551 883.43 1.34 0.001 Labeled
†
Oedema 68/196 40.67 1.67 0.004 Labeled
*Oedema 118/351 72.26 1.63 0.001 Labeled
Table 3. Continued
Adverse event Pneumococcal/
Other vaccine
Disproportionality analysis Tree-based scan statistic
MFDS PRR ROR IC
025χ
2Expected Relative
risk p-value
#
Application site disorders
†
Cellulitis 108/105 5.65 5.69 1.72 204.13 32.82 3.29 0.001 Labeled
†
Injection site reaction 962/1,848 2.86 3.00 1.15 790.28 432.93 2.22 0.001 Labeled
†
Injection site urticaria 15/41 2.01 2.01 0.87 5.57 Labeled
†
Injection site rash 398/1,414 279.17 1.43 0.001 Labeled
#
Resistance mechanism disorders
†
Sepsis 12/28 2.35 2.35 1.04 6.54 Labeled
#



![첨부파일 : [코로나19 백신 이슈] 국외 코로나19 예방접종 후 이상반응 보고 현황](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)