Address reprint requests to Ju Kang Lee, M.D.
Department of Physical & Rehabilitation Medicine, Gachon University School of Medicine, 1198 Guwol-dong, Namdong-gu 405-760, Korea
TEL: 82-10-3235-3197, FAX: 82-32-460-3722, E-mail: [email protected]
투고일: 2014년 5월 12일, 1차 수정일: 2014년 6월 19일, 2차 수정일: 2014년 6월 24일, 게재확정일: 2014년 6월 24일
INTRODUCTION
Dropped Head Syndrome (DHS) is a rare disease and characterized with severe paravertebral extensor muscle
weakness which may cause several clinical entities such as pain, weakness, dysphagia, dyspnea, and so on. The syndrome exhibits chin-on-chest deformity and DHS patient cannot lift one’s head.
1,2The patient’s spinal cord
방사선치료 후 다발성 경추부신경근병변과 동반된 Dropped Head Syndrome
가천대학교 의학전문대학원 재활의학교실
임오경∙심호용∙윤진원∙이진영∙박기덕∙이주강
– Abstract –
Dropped Head Syndrome (DHS) Combined with Cervical Polyradiculopathy Following Radiotherapy
Oh Kyung Lim, M.D., Ph.D., Ho Yong Shim, M.D., Jin Won Yoon, M.D., Jin Young Lee, M.D., Ki Deok Park, M.D., Ph.D., Ju Kang Lee, M.D., Ph.D.
Physical & Rehabilitation Medicine, Gachon University School of Medicine
We report a 55-year-old man with dropped head syndrome who developed neck extensor muscle weak- ness. After he was treated with radiotherapy (66Gy) two years ago because of non-small cell lung cancer, he exhibited progressive inability tolift his head with severe neck pain and dropped head posture.
The electrodiagnostic study revealed left cervical polyradiculopathy and polyneuropathy combined with cervical myelopathy, and localized myopathic change was detected on trapezius muscle biopsy. Cervical magnetic resonance images revealed cervical spine compression fracture and multiple foraminal stenosis, so we concluded that dropped head posture was caused from radiotherapy induced myopathy of neck extensor muscle and left upper extremity pain and weakness was resulted from compression polyradicu- lopathy due to prolonged cervical flexion contracture.
Although neuropathic pain and the neck movement limitation were treated with physical therapy, cervical orthosis, trigger point injection and medication, the improvement was limited. We suggest that the early diagnosis of dropped head syndrome (DHS) and appropriate rehabilitative management should be consid- ered to prevent severe secondary complications such as myopathy and neuropathy.
Key Words: radiculopathy, radiotherapy, dropped head syndrome
could be compressed because of dropped head position.
Here we report a patient who developed DHS with Non Small Cell Lung Cancer (NSCLC) after radiotherapy.
CASE REPORT
A 55-year-old man presented with progressive weak- ness of neck extension for five months. Associated symptoms were the posterior neck pain and weakness of the left upper limb. The patient was diagnosed with NSCLC (Stage IIIA) at 3 years ago. The primary mass was located in the left upper lobe and extended to the apex and the left lower neck area. The combination chemotherapy had administrated to him during 2 years (docetaxel with cisplatin from June to July in 2010 and pemetrexed from August, 2011 to February, 2012) with 9 months scheduled radiotherapy (July, 2010 to May, 2011), simultaneously. The amount of radiation targeting to the left upper lung and the mediastinum was 66Gy and to the spine from C4 to T1 level was 40Gy.
Nine months after radiotherapy, the patient initially complained of posterior neck pain and the oncologist suspected tumor metastasis to the cervical spine. Eight month schedule additional chemotherapy was performed to the patient. Seven month after the completion of addi- tional chemotherapy, the posterior neck pain and exten- sor muscle weakness aggravated and range of neck motion was limited progressively. So the patient visited our clinic with incorrectable neck flexion posture known as dropped head syndrome, he could not sleep on supine position due to severe neck pain and contracture.
The left elbow flexor, elbow extensor and wrist exten- sor muscles were grade IV. The finger flexor, hand intrinsic and finger extensor muscles were grade III.
Moreover, the left hip flexor, knee extensor and ankle dorsiflexor muscles were grade IV. Decreased sensation to light touch, pain, and temperature was noted below the left C2 dermatome. The deep tendon reflex (DTR) was increased on the left biceps brachii and the knee extensor tendon, so the cervical myelopathy was suspect- ed. Cervical magnetic resonance imaging (MRI) showed mild herniation of cervical discs from C4 to C7 and spinal stenosis between C5 and C6 (Fig. 1).
In the resting state, his cervical spine was tilted 5 degrees to the left and flexed 90 degrees. The active range of neck extension was 20 degrees and the passive range of motion was 25 degrees from the 90 degree flexed resting position. Passive rotation of the cervical
spine was 50 degrees to right side and 40 degrees to left side. In the plain radiography of the cervical spine, the maximal range of motion from flexion to extension was only 14.84 degrees (Fig. 2).
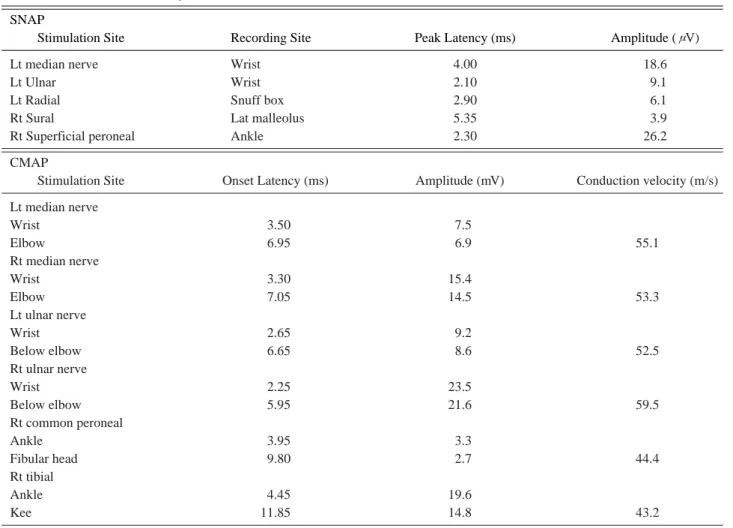
The electrodiagnostic test revealed left cervical polyradiculopathy combined with sensory polyneuropa- thy involving upper and lower extremities (Table. 1,2).
Moreover, the delayed latency in left median and tibial somato-sensory evoke potential (SEP) suggested cervical myelopathy, which we considered resulted from the cer- vical cord compression by longstanding cervical spine flexion contracture.
The muscle biopsy on left cervical paraspinal muscle revealed myopathic changes, such as fibrosis, variation of size and shape without inflammatory cell. The other laboratory tests and tensilon test to rule out neuromuscu- lar and rheumatic diseases were within normal limit.
We concluded that dropped head syndrome with left upper extremity pain and weakness was resulted from sequential pathologic courses. Radiation-induced myo- pathic changes of neck extensor muscles caused dropped head posture, which resulted in compression cervical myelopathy and polyradiculopathies. The medication including opiod analgesic and pregabalin and physiother- apy had limited improvement of pain and range of motion. The cervical orthosis for preventing flexion was not successful because of pain and discomfort. The trig- ger point injections (1% lidocaine) to the upper trapezius muscles, the cervical paraspinal muscles and the rhom-
– 71 –
Fig. 1. Sagittal T2 weighted magnetic resonance imaging scan of the cervical spine showing mild disc herniation from C4-C7, spinal stenosis between C5-C6.
boid muscles were performed in every two days. The range of neck extension was increased following the injection and the Visual Analog Scale (VAS) score improved from 8 points to 3 points, although the effect of injection lasted few hours. On initial visit to our department, he could not lie down or sleep on supine position because of the neck pain but he could sleep on supine position after injection and physiotherapy.
DISCUSSION
DHS was introduced by Suarez and Kelly in 1992 with severe neck extensor weakness in the absence of specific abnormalities on electromyography or muscle biopsy.
Especially if passive range of motion is intact in the absence of any other neuromuscular disorder, it could be referred as Isolated Neck Extensor Myopathy (INEM).
3Although the exact cause of DHS remains controversial, the most favored hypothesis suggests that the injury and fatigue of cervical paraspinal musculature secondarily induce kyphotic posture and age-related loss of tissue
elasticity.
2,4Electromyography, muscle biopsy, magnetic resonance image, and laboratory studies should be performed to diagnose DHS. Electromyography of paraspinal cervical musculature shows either abnormal spontaneous activity including fibrillation and positive sharp wave or myo- pathic pattern. Muscle biopsy is not usually recommend- ed, but it can be discern able for diagnosing neuromuscu- lar diseases presenting inflammation from INEM, which reveals fibrosis, increased fiber size diversity and myofibrillar disarray.
5,6Laboratory studies may help distinguish INEM from other neurologic etiologies, such as polymyositis, inflammatory myositis, myasthenia gravis, chronic inflammatory demyelinating polyneuropathy, hypothy- roidism and hypokalemia.
7MRI should be checked to exclude spinal cord com- pression and if spinal cord compression is detected by MRI, surgical decompressive procedure could be added.
CT is also recommended if MRI is not testable.
2In this case, laboratory findings containing erythrocyte sedi-
Fig. 2. Flexed cervical spine with chin on chest was seen in his initial photograph (A), Plain lateral radiograph of the cervical spine; neutral (B), flexion (C), and extension (D).A B
C D
– 73 –
mentation rate, c-reactive protein, creatine kinase, thy- roid function tests, tensilon tests and antiacetylcholine receptor antibody test ruled out other neuromuscular dis- eases.
2In this case, we suspect the pathological sequence occurred serially after the radiation therapy to neck cer- vical region. First, post-radiation induced myopathy induced weakness of neck extensor muscle. Julie et al reported three cases of late onset DHS in patients who
had received high-dose mantle field irradiation or whole- body irradiation for Hodgkin’s disease.
3Second, the lim- ited range of motion and contracture in flexion position of the patient exacervated stenosis of spinal canal and neural foramen which resulted in cervical polyneuropa- thy and myelopathy.
The pathophysiology of the late effects of radiation- induced neuromuscular disease is on debate. Some researchers claim that selective injury to the lower motor
Table 2. Needle ElectromyographyMuscle IA Spontaneous activity MUAPs Recruitment pattern
L. APB, ADM, FDI, FCU, FCR Inc Fibs & PSWs (+) Polyphasic Reduced
L. Biceps, triceps, deltoid Normal - Normal Reduced
CER PSP (C5-T1) Inc Fibs & PSWs (+) NC NC
MUAP: Motor Unit Action Potential, Recr: Recruitment, IA: Insertion activity, Fib: Fibrillation, PSW: Positive Sharp Wave, R:
Right, L: Left, APB: Abductor Pollicis Brevis Muscle, ADM: Abductor Digiti Minimi Muscle, FDI: First Dorsal interossei Muscle, FCU: Flexor Carpi Ulnaris Muscle, FCR: Flexor Carpi Radialis Muscle, CER PSP: Cervical Paraspinal Muscle, NC: Not Checkable, Inc: Increased
Table 1. Nerve Conduction Study SNAP
Stimulation Site Recording Site Peak Latency (ms) Amplitude (μV)
Lt median nerve Wrist 4.00 18.6
Lt Ulnar Wrist 2.10 9.1
Lt Radial Snuff box 2.90 6.1
Rt Sural Lat malleolus 5.35 3.9
Rt Superficial peroneal Ankle 2.30 26.2
CMAP
Stimulation Site Onset Latency (ms) Amplitude (mV) Conduction velocity (m/s) Lt median nerve
Wrist 3.50 7.5
Elbow 6.95 6.9 55.1
Rt median nerve
Wrist 3.30 15.4
Elbow 7.05 14.5 53.3
Lt ulnar nerve
Wrist 2.65 9.2
Below elbow 6.65 8.6 52.5
Rt ulnar nerve
Wrist 2.25 23.5
Below elbow 5.95 21.6 59.5
Rt common peroneal
Ankle 3.95 3.3
Fibular head 9.80 2.7 44.4
Rt tibial
Ankle 4.45 19.6
Kee 11.85 14.8 43.2
SNAP, sensory nerve action potential; CMAP, compound motor action potential; Rt, Right; Lt, Left
neurons in the spinal cord is the leading cause of it. Oth- ers insist that the main site of insult is spinal roots or peripheral nerves. Others believe that ischemic nerve insult gives rise to conduction block of motor axons, in cases of delayed post-radiation plexopathy which responds to treatment with anti-coagulation.
3Son et al. suggested that excessive mechanical stress to the region of transition from cervical lordosis to thoracic kyphosis due to weakness of neck muscles led to hyper- trophies of the ligamentum flavum and the posterior lon- gitudinal ligament, finally causing upper thoracic myelopathy.
8In this case, the patient was treated with radiotherapy which included mantle field (i.e., of the lymph nodes of the neck, axilla, and mediastinum) and, especially, the left C4 area. The total amount of radiation was 40 Gy which was similar dose reported by Sumita et al.
9We first reported this case in Korea. DHS associated lung cancer is also extremely sparse.
Because the patient was in advanced stage in DHS, we could not get the significant improvement for his pain and limitation of neck motion. If clinicians recognized DHS in the early stage, severe complication such as con- tracture and compression neuropathy could be prevented.
So, the diagnosis and aggressive treatment should be considered in early stage. Moreover, if the patient's life expectancy is long, the surgical treatment would be taken into account.
10REFERENCES
1. Liao JP, Waclawik AJ, Lotz BP, Salamat SM, Beinlich
BR, Brooks BR: Myopathic Dropped Head Syndrome An Expanding Clinicopathological Spectrum, Am J Phys Med Rehabil 2007;86:970-6
2. Sharan AD, Kaye D, Malveaux W, Riew KD: Dropped Head Syndrome: Etiology and Management, J Am Acad Orthop Surg 2012;20:766-74
3. Rowin J, Cheng G, Lewis SL, Meriggioli MN: Late Appearance of Dropped Head Syndrome after Radiothera- py for Hodgkin’s Disease, Muscle Nerve 2006;34:666-9 4. Katz JS, Wolfe GI, Burns DK, BryanWW, Fleckenstein
JL, Barohn RJ.: Isolated Neck Extensor Myopathy: A Common Cause of Dropped Head Syndrome, Neurology 1996;46:917-21
5. Ahmed A, Specht CS, Scott K: A Case of Dropped Head plus Syndrome, J Clin Med Res 2009;1:230-2
6. Zenmyo M, Abematsu M, Yamamoto T, Ishidou Y, Komiya S, Ijiri K: Dropped Head Syndrome due to Myo- genic Atrophy: A Case Report of Surgical Treatment, Diagn Pathol 2011;6:9
7. Nakanishi K, Taneda M, Sumii T, Yabuuchi T, Iwakura N.:
Cervical Myelopathy Caused by Dropped Head Syn- drome, J Neurosurg Spine 2007;6:165-8
8. Son HK, Cha YS, Suh H, Ki CS, Shin YB: Upper Thoracic Myelopathy Caused by Delayed Neck Extensor Weakness in Myotonic Dystrophy, Ann Rehabil Med 2012;36:569- 72
9. Bhatia S, Miller RC, Lachance DL: Neck extensor muscle weakness (Dropped head syndrome) following radiothera- py, Radiol Oncol 2006;40:29-33
10. Petheram TG, Hourigan PG, Emran IM, Weatherley CR:
Dropped Head Syndrome A Case Series and Literature Review, Spine 2008;33:47-51