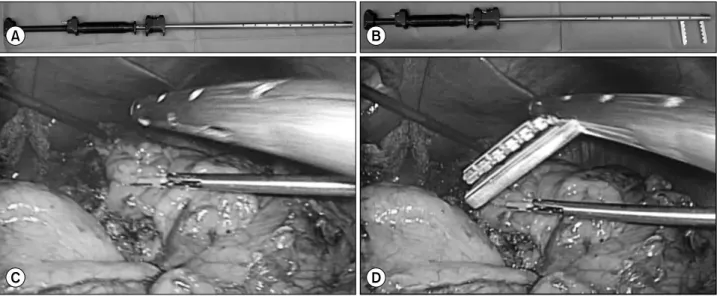
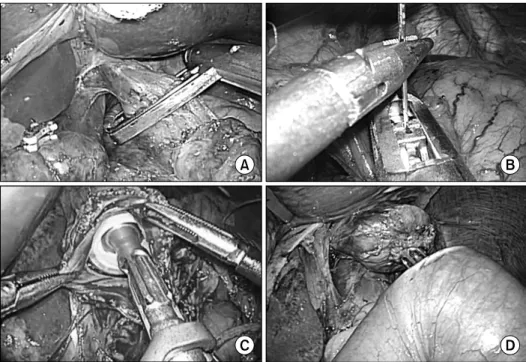
Intracorporeal End-to-Side Esophagojejunostomy Using a Laparoscopic Purse-String Clamp during Laparoscopic Total Gastrectomy
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
Fig.11 Temperature histories of the hot side and cold side heat exchangers according to time with speaker power(10W).. Fig.12 Temperature histories of the hot
And We tried to look out the mathematics-appraisal-guide that was reported in Korea Institute of Curriculum & Evaluation(KICE) to show the education-goal
At the beginning of each section, make clear to the reader in advance what the purpose of that section will be and how that section relates to the preceding material. At
during. When the inductor current is zero, expires, S4 is off, and Sf turns on during to short the two ends of the inductor and suppress possible ringing at Vx until the end
□ The least-upper-bound property (sometimes called completeness or supremum property) is a fundamental property of the real number system. The least-upper-bound
□ The least-upper-bound property (sometimes called completeness or supremum property) is a fundamental property of the real number system. The least-upper-bound
이것은 가 위로 유계가 아니라는 문제의 가정에 모순이다... 유리수의
3,4 Therefore, to date, studies have been conducted to examine the absorbable fixation plate manufactured using polymer and a fixation screw that can
