대한소화기학회지 2004;43:211-214
INTRODUCTION
1)Brunner's gland hamartoma is a rare tumor of the duodenum that was first described by Salvioli in 1876.1 It is commonly recognized by incidental finding. However, Brunner's gland hamartomas can clinically lead to signifi- cant symptoms including gastrointestinal bleeding, abdominal
접수: 2003년 10월 11일, 승인: 2004년 2월 13일 연락처: 박창환, 501-757, 광주광역시 동구 학동 8
전남대학교 의과대학 내과학교실
TEL: (062) 220-6296, Fax: (062) 228-1330 E-mail: [email protected]
pain, and intestinal obstruction.2 The hamartomas were generally polypoid in configuration and most commonly found within the range of the standard esophagogastroduodenoscope.3 They were rarely seen in the jejunum and proximal ileum.4We report an unusual case of Brunner's gland hamartoma that was located in the fourth portion of the duodenum2)and presented with obscure gastrointestinal bleeding.
Correspondence to: Chang Hwan Park, M.D., Ph.D.
Department of Internal Medicine, Chonnam National University College of Medicine
8 Hak-dong, Dong-gu, Gwangju 501-757, Korea Tel: +82-62-220-6296, Fax: +82-62-228-1330 E-mail: [email protected]
잠복성 위장관 출혈을 일으킨 Brunner선 과오종 1예
전남대학교 의과대학 내과학교실, 외과학교실*, 병리학교실†
박창환·이수정·박정호·박재홍·이완식·주영은·김현수·최성규·유종선·유성협*·이민철
†·김세종
A Case of Brunner's Gland Hamartoma Presenting as Obscure Gastrointestinal Hemorrhage
Chang Hwan Park, M.D., Soo Jung Lee, M.D., Jeong Ho Park, M.D., Jae Hong Park, M.D., Wan Sik Lee, M.D., Young Eun Joo, M.D., Hyun Soo Kim, M.D., Sung Kyu Choi, M.D., Jong Sun Rew, M.D., Seong Yeob Ryu, M.D.*, Min Cheul Lee, M.D.†, and Sei Jong Kim, M.D.
Departments of Internal Medicine, General Surgery*, and Pathology†, Chonnam National University College of Medicine, Gwangju, Korea
Brunner's gland hamartomas are rare tumors of duodenum, they are often discovered incidentally during esophagogastroduodenoscopy or upper gastrointestinal series. These tumors arise mainly in the duodenal bulb and can present with gastrointestinal hemorrhage and intestinal obstruction. Most of Brunner's gland hamartomas are located within the range of the standard esophagogastroduodenoscope. However, they are rarely located below the third portion of duodenum. As well known, the small intestine, including the 4
thportion of duodenum, jejunum, and ileum, is relatively inaccessible with routine endoscopy. Thus, the diagnosis of Brunner's gland hamartoma in these area can be delayed up to several months after onset of symptoms. We report a case of Brunner's gland hamartoma which was located in the fourth portion of the duodenum and presented as obscure gastrointestinal hemorrhage. Radiologic, surgical, and pathologic appearances are presented. (Korean J Gastroenterol 2004;
43:211-214)
Key Words: Brunner's glands; Hamartoma; Intestine, small; Gastrointestinal hemorrhage
대한소화기학회지: 제43권 제3호, 2004
CASE REPORT
A 55-year-old woman had visited the private clinic with a history of several episodes of melena, dizziness, and weakness for 9 months. She was healthy, and there was no history of hematemesis, abdominal pain, nausea, or vomiting. She was found to be severely anemic. After blood transfusion, esophagogastroduodenoscopy, colonoscopy, and small bowel series were carried out. None of abnormal pathological findings was identified. The patient was then transferred to our institution. On admission, laboratory
values were as follows: hemoglobin, 5.3 g/dL; hematocrit, 17.0%; ferritin, 5.83 ng/mL. Other laboratory values were within normal limits.
Esophagogastroduodenoscopy and colonoscopy were performed repeatedly, and there was no significant finding.
Technetium99 red blood cells scintigraphy was negative.
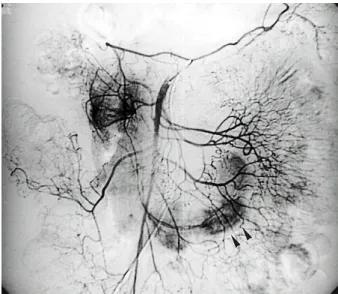
However, superior mesenteric angiogram showed a hyper- vascular-staining lesion in the distal duodenum and the proximal jejunum (Fig. 1). Computed tomographic scan of the abdomen showed a 6×3×3 cm mass lateral to the abdominal aorta, involving the fourth portion of the duodenum and the proximal jejunum (Fig. 2). There was no significant enlargement of lymph nodes, and the surrounding structures were normal.
On diagnostic laparotomy, a 7 cm pedunculated polyp was found arising from the fourth portion of the duodenum and extending to the proximal jejunum. The polyp was
Fig. 1. Superior mesenteric angiogram. It shows a hypervascular- staining lesion (arrowheads) in the distal duodenum and the proximal jejunum.
Fig. 2. Computed tomographic scan. It shows a mass (arrowheads) lateral to the abdominal aorta, involving the fourth portion of the duodenum and the proximal jejunum.
Fig. 4. Histological findings. Lobules of Brunner's glands with intervening bands of fibrous tissue are seen below the duodenal mucosa and villi (H&E, ×40).
Fig. 3. Gross finding. It shows a well-circumscribed, elongated, 6.5
×3×2 cm sized polypoid mass with focal surface ulceration.
212
박창환 외 11인. 잠복성 위장관 출혈을 일으킨 Brunner선 과오종 1예
removed after duodenotomy.
On gross examination, the lesion was a well- circumscribed, elongated, 6.5×3×2 cm sized polypoid mass with focal surface ulceration (Fig. 3). The cut surface was solid, lobulated, and pink-colored. Microscopically, the tumor was located beneath the muscularis mucosa that was composed of Brunner's glands with the intervening fibrous bands (Fig. 4). The glands were lined by cuboidal-to- columnar cells with pale, eosinophilic cytoplasm and basally situated small, flattened nuclei. There was no cellular immaturity or cytologic atypia. The connective tissue stroma contained a mixture of ducts, adipose tissues, smooth muscles, and lymphoid aggregates. In the duodenal epithelium, there was foveolar metaplasia and focal surface ulceration.
One-year follow-up evaluation after the resection of the Brunner's gland hamartoma revealed complete resolution of the iron deficiency anemia, and bleeding did not recur.
DISCUSSION
Patients with obscure gastrointestinal hemorrhage are a diagnostic and therapeutic challenge. Although estimating the current prevalence of obscure bleeding in gastrointestinal hemorrhage is difficult, it is expected less than 5%.5 When routine endoscopy and colonoscopy are not diagnostic and the patient continues to have recurrent bleeding, further evaluations are required.6 Most often the small bowel is suspected as the site of hemorrhage.6
Tumors of the small intestine present a unique challenge to the clinicians across medical specialities. Because the small intestine is relatively inaccessible to routine endoscopy, diagnosis of small intestinal neoplasms is often delayed up to several months after onset of symptoms.7 Brunner's gland hamartomas are rare tumors of the duodenum that are usually small in size. Only a few cases of tumors more than 4 to 5 cm in size have been reported in the literature.8 Brunner's gland hamartomas are mostly located in the duodenal bulb (57%). Additionally, they are found in the second (27%) and third (5%) portions of the duodenum, the pyloric channel (5%), jejunum (2%), and proximal ileum (2%).4 However, there has been no report of the hamartoma in the 4th portion of the duodenum. There are great variations in their size from millimeters to several centimeters. Their usual size is 1 to 2 cm, but the
hamartoma of 12×10×8 cm has ever reported.9
The proper nomenclature for the Brunner's gland proliferation is still controversial, but the features described by Goldman10 most acceptable. They include the lack of encapsulation, a mixture of ducts, acini, smooth muscle, and in some cases adipose tissue, the presence of a continuous sheet of Brunner's glands from the normal submucosa into the stalk and body of the tumor, and the lack of any cellular atypia. In our patient, the tumor was composed mainly of normal tissue including Brunner's glands, ducts, smooth muscle, adipose tissue, and lymphoid tissue. In addition, no cellular immaturity or cytologic atypia was noted. These are in good agreements with the features described above and differentiated from those of adenoma.
Brunner's gland hamartomas usually present in the 4th to 6th decades of life. Most of them are usually found incidentally during the evaluation of symptoms for a peptic ulcer disease or gastroesophageal reflux. Clinically significant presentations include hemorrhage and obstruction.3 Gastrointestinal hemorrhage due to ulceration or erosion of the mucosa stretched over the tumor typically manifest hematemesis or melena, which can occasionally be massive and rarely fatal.3,11,12 Since most of hamartomas were located within the range of the standard esophago- gastroduodenoscope, diagnosis was easily made, and appropriate therapy was instituted without difficulty. Hwang et al13 reported a case of Brunner's gland hamartoma with severe anemia and intussusception. They easily detected the Brunner's gland hamartoma in the duodenal bulb with the standard esophagogastroduodenoscope. However, in our patient, the hamartoma was located unusually in the fourth portion of the duodenum and presented with obscure gastrointestinal hemorrhage. Diagnosis was not made with the standard esophagogastroduodenoscope. Angiography and computed tomography were helpful to detect the hamartoma.
Conservative management is advocated for asymptomatic small lesions of Brunner's glands, since they are not premalignant. The lesions that are causing gastrointestinal hemorrhage, intestinal obstruction, and other atypical manifestations should be excised endoscopically or surgically for both therapeutic purposes and confirmation of the suspected diagnosis.
We report a case of Brunner's gland hamartoma that was located in the fourth portion of the duodenum and presented with obscure gastrointestinal hemorrhage.
213
The Korean Journal of Gastroenterology: Vol. 43, No. 3, 2004
On the basis of this case, we can conclude that in the cases of gastrointestinal hemorrhage of which etiologies are not common or small bowel tumors that require surgery for curing, Brunner's gland hamartoma in an unusual location should be considered as an alternative diagnostic choice.
요 약
Brunner선 과오종은 조직학적으로 도관 및 산재된 간질 성분을 동반한 정상 십이지장의 Brunner선의 과증식을 보 이는 양성 상피성 종양이다. 십이지장 구부에 주로 발생하 여 무증상으로 상부위장관조영술이나 상부위장관내시경검 사에서 우연히 발견되는 경우가 대부분이지만 상부위장관 출혈이나 장폐색 등의 증상을 일으키기도 한다. 증상이 있 는 경우에도 십이지장 구부에 주로 발생하기 때문에 상부 위장관내시경검사 및 상부위장관조영술로 대부분 쉽게 진 단이 되며 십이지장 구부 이하에 위치하여 진단이 어려운 경우는 매우 드물다. 이에 저자들은 십이지장 제4부에 위치 하여 진단이 어려운 잠복성 출혈을 보인 Brunner선 과오종 한 예를 문헌 고찰과 함께 보고한다.
REFERENCES
1. Kaplan EL, Dyson WL, Fitts WT Jr. The relationship of gastric hyperacidity to hyperplasia of Brunner's glands. Arch Surg 1969;98:636-639.
2. Block KP, Frick TJ, Warner TF. Gastrointestinal bleeding from a Brunner's gland hamartoma: characterization by endoscopy, computed tomography, and endoscopic ultrasound. Am J Gastroenterol 2000;95:1581-1583.
3. Levine JA, Burgart LJ, Batts KP, Wang KK. Brunner's gland
hamartomas: clinical presentation and pathological features of 27 cases. Am J Gastroenterol 1995;90:290-294.
4. Walden DT, Marcon NE. Endoscopic injection and polypectomy for bleeding Brunner's gland hamartoma: case report and expanded literature review. Gastrointest Endosc 1998;47:403-407.
5. American Gastroenterological Association. American Gastro- enterological Association medical position statement: evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology 2000;118:197-201.
6. Jensen DM. Current diagnosis and treatment of severe obscure GI hemorrhage. Gastrointest Endosc 2003;58:256-266.
7. Gill SS, Heuman DM, Mihas AA. Small intestinal neoplasms.
J Clin Gastroenterol 2001;33:267-282.
8. Yadav D, Hertan H, Pitchumoni CS. A giant Brunner's gland adenoma presenting as gastrointestinal hemorrhage. J Clin Gastroenterol 2001;32:448-450.
9. de Silva S, Chandrasoma P. Giant duodenal hamartoma consisting mainly of Brunner's glands. Am J Surg 1977;133:
240-243.
10. Goldman RL. Hamartomatous polyps of Brunner's glands.
Gastroenterology 1963;44:57-62.
11. Schluger LK, Rotterdam H, Lebwohl O. Gastrointestinal hemorrhage from a Brunner's gland hamartoma. Am J Gastroenterol 1994;89:2088-2089.
12. Kouraklis G, Kostakis A, Delladetsima J. Hamartoma of Brunner's glands causing massive haematemesis. Scand J Gastroenterol 1994;29:841-843.
13. Hwang JH, Kim J, Moon SH, et al. A case of Brunner's gland hamartoma with severe anemia and intussusception.
Korean J Gastrointest Endosc 1997;17:691-695.
214