https://doi.org/10.35827/cp.2021.20.1.43
접수일 : 2020 년 10 월 20 일 , 게재승인일 : 2020 년 11 월 24 일 책임저자 : 박지혜 , 서울시 은평구 통일로 1021
뿸 03312, 가톨릭대학교 의과대학 은평성모병원 재활 의학교실
Tel: 02-2030-4619, Fax: 02-2030-4620 E-mail: [email protected]
신경과 먼 부위 근육 내 주사 후 발생한 좌골신경병증
가톨릭대학교 의과대학 은평성모병원 재활의학교실
윤수인ㆍ박지수ㆍ고윤담ㆍ송대헌ㆍ박지혜
Sciatic Neuropathy after Intramuscular Injection at a Site Remote from the Nerve
Soo In Yun, M.D., Jisoo Park, M.D., Yun Dam Ko, M.D., Dae-Heon Song, M.D., Ph.D. and Jihye Park, M.D.
Department of Rehabilitation Medicine, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Sciatic nerve can be injured by various mechanism such as compression, traction during surgery, and direct trauma. This case reports a sciatic neuropathy caused by compression due to hematoma occurring after intramuscular injection in the gluteus medius muscle far from the nerve. In order to avoid occurrence of sciatic neuropathy after buttock injection, the injection was made in the upper outer quadrant of the buttock, but sciatic neuropathy occurred. Sciatic neuropathy can be confused with lumbar radiculopathy, so differential diagnosis is important. (Clinical Pain 2021;20:43-48)
Key Words: Sciatic neuropathy, Intramuscular injection, Gluteus medius
INTRODUCTION
The sciatic nerve originates from the L4-S3 nerve roots, the anterior division becomes the tibial nerve and the poste- rior division becomes the common peroneal nerve. The sci- atic nerve exits the pelvis through the greater sciatic fora- men and passes beneath the piriformis muscle. The sciatic nerve, covered by the gluteus maximus, then runs medial and posterior to the hip joint. It supplies sensation to the distal leg except for the medial area and foot, and in- nervates the muscles of the anterior/lateral and posterior compartments of the legs. These muscles function as knee flexion, ankle dorsiflexion, and ankle plantar flexion.
Nerve injury after injection is relatively common and the sciatic nerve is one of the most commonly involved nerves.
The causes of sciatic neuropathy include direct trauma, per- ineural nerve injection injury, infarction, or compression [1].
In this case report, we present a case of sciatic neuro-
pathy caused by hematoma after intramuscular injection of the gluteus medius muscle, a remote site from the sciatic nerve.
CASE REPORT
A 68-year-old man visited to neurosurgery outpatient
clinic with severe pain in the left gluteal area which radi-
ated down the calf for a week. He had chronic lower leg
pain, but recently complained that the pain has worsened
and cannot walk. There was no specific history of trauma
to the area. There was no underlying disease other than dia-
betes mellitus, and he was taking diabetes and pain
medication. Lumbar X-ray showed degenerative spondy-
losis, and lumbar spine computed tomography (CT) and
magnetic resonance imaging (MRI) were performed with
suspicion of lumbosacral radiculopathy, but there were no
abnormalities. Thus he was prescribed pain medications
and planned a follow-up visit. The patient returned 2 weeks
later with aggravated pain and was hospitalized for further
evaluation and treatment. In the last two weeks, he was
given several blocks at his lower back and an intramuscular
injection in the left buttock, especially in the upper outer
quadrant of gluteus medius at the local pain clinic. On
physical examination, manual muscle tests revealed weak-
ness of left toe and ankle dorsiflexion, which was grade
Table 1. Sensory Nerve Conduction Study
Sensory nerve Stimulation Peak latency (ms) Amplitude (μV) Distance (cm) CV (m/s)
Rt. Sural Calf 3.8 10.4 14.0 44
Lt. Sural Calf 3.9 10.0 14.0 44
Rt. Superficial peroneal Lower leg 2.8 12.4 9.0 41
Lt. Superficial peroneal Lower leg 3.1 7.0* 9.0 39
Rt.: Right, Lt.: Left, ms: millisecond, μV: microvolt, CV: conduction velocity, m/s: meter/second.
*Decreased amplitude of SNAP.
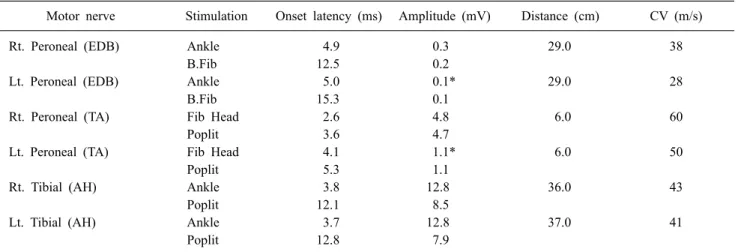
Table 2. Motor Nerve Conduction Study
Motor nerve Stimulation Onset latency (ms) Amplitude (mV) Distance (cm) CV (m/s)
Rt. Peroneal (EDB) Ankle 4.9 0.3 29.0 38
B.Fib 12.5 0.2
Lt. Peroneal (EDB) Ankle 5.0 0.1* 29.0 28
B.Fib 15.3 0.1
Rt. Peroneal (TA) Fib Head 2.6 4.8 6.0 60
Poplit 3.6 4.7
Lt. Peroneal (TA) Fib Head 4.1 1.1* 6.0 50
Poplit 5.3 1.1
Rt. Tibial (AH) Ankle 3.8 12.8 36.0 43
Poplit 12.1 8.5
Lt. Tibial (AH) Ankle 3.7 12.8 37.0 41
Poplit 12.8 7.9
Rt.: Right, Lt.: Left, EDB: Extensor digitorum brevis, TA: Tibialis anterior, AH: Abductor hallucis, B.Fib: Below fibular head, Fib Head: Fibular head, Poplit: Popliteal fossa, ms: millisecond, mV: millivolt, CV: conduction velocity, m/s: meter/second.
*Decreased amplitude of CMAP.
2 according to the Medical Research Council (MRC) scale for muscle strength. The paresthesia and hypesthesia was localized in left lateral calf and foot dorsum. Pathologic re- flexes were negative and deep tendon reflexes of knee and ankle were normoactive. There was tenderness in the left lateral mid-buttock area. In blood test, C-Reactive Protein showed a mild elevation of 1.30 mg/dl (normal range: 0.01∼
0.5 mg/dl), and other abnormalities were not observed.
Because lumbar spine imaging studies did not show specif- ic findings to demonstrate the symptoms, electrodiagnostic study was requested. Nerve conduction study of lower ex- tremity showed reduced amplitude of sensory nerve action potential (SNAP) in left superficial peroneal nerve and re- duced amplitude of compound muscle action potential (CMAP) in left common peroneal nerve recording at ex- tensor digitorum brevis muscle. The conduction velocity of
CMAP around fibular neck was normal (Table 1, 2). On
needle electromyography (EMG), left L4-L5 paraspinalis,
gluteus medius, tibialis anterior, and peroneus longus
showed positive sharp waves (Table 3). Base on the results,
we suggested a left peroneal neuropathy combined with left
superior gluteal neuropathy, but it is uncommon for the two
distant nerves to be involved. Therefore, we recommended
the pelvis MRI to demonstrate the lesion that causes
neuropathies. In the pelvis MRI, 6 × 6 × 2.4 cm sized het-
erogenous mass-like lesion was found within the left glu-
teal medius muscle, which was probably intramuscular
hematoma (Fig. 1, 2), and the distal portion of the hema-
toma was close to the lateral side and above of the sciatic
nerve (Fig. 1-B, 2-B, C). Furthermore, there was partial
tear of left gluteus maximus and gluteus medius muscles
(Fig. 2). There was no definite signal intensity change or
Table 3. Needle Electromyography
Muscle IA Fib PSW MUAP Recruitment pattern Interferential pattern
Both L2-L4 paraspinalis NL None None
Rt. L4-L5 paraspinalis NL None None
Lt. L4-L5 paraspinalis NL None 1+
†Both L5-S1 paraspinalis NL None None
Both Gluteus Maximus NL None None NL NL Full
Both Tensor Fascia Lata NL None None NL NL Full
Both Gastrocnemius (med) NL None None NL NL Full
Both Soleus NL None None NL NL Full
Lt. Gluteus Medius NL None 2+
†NL NL Reduced
‡Lt. Vastus Medialis NL None None NL NL Full
Lt. Tibialis Anterior NL None 2+
†NL NL Discrete
‡Lt. Tibialis Posterior Increased* None None NL NL Full
Lt. Peroneus Longus NL None 2+
†NL NL Discrete
‡Rt. Tibialis Anterior NL None None NL NL Full
Rt. Peroneus Longus NL None None NL NL Full
IA: insertional activity, Fib: Fibrillation, PSW: Positive sharp wave, MUAP: Motor Unit Action Potential, NL: Normal, Poly:
Polyphasic.
*Increased insertional activities at rest.
†
Abnormal spontaneous activities at rest.
‡