大짧放 9‘t 線醫웰會품‘ 第 24卷 第2 號 pp. 201 - 212, 1988 Journal 01 Korean Radiological Society, 24(2) 201-212, 1988
Computed Tomography of Cavernous Sinus Diseases
Jin Wook Chung, M.D., Kee Hyun Chang, M.D., Moon Hee Han, M.D., 80 Hyun Kim, M.D., Chi Sung Song, M.D., Hyo Keun lim, M.D., Jong Chul Kim, M.D. *
Department of Radiology, College of Medicine, 5eoul National Univerisity
〈국문초록〉
해면정맥동 질환에서의 전산화단층촬영술
서울대 학교 의 파대 학 방사선과학교실
정 진 욱 • 장 기 현 • 한 문 희 • 김 보 현 • 송 치 성 • 임 효 근 • 김 종 칠.
저자들은 강밸진안에 도움이 되는 CT소견을 찾기 위해서 최근 5 년간 경험한 21 례의 해연정액동 영변 을 역행석무로 분석하였다. 21례를 원인별로 분류하연 패혈성 혈전증 5 례, 경동액-해연정액동류 5 례, 양성종양 5례, 악성전이암 6 례였마. CT 소견은 해연정액동의 모양, 조영증강양상, 양측성여부, 주위골 변화, 안와변화 및 두개강내 이상소견의 동반여부에 중점을 두어 분석하였마.
패혈성 해연정액옹 헐천증 5례중 4례에서 조영증강을 보이는 해연정액동 내부에 다수의 불규칙한 음 영결손。 1 일측성 또는 양측성으로 판찰되었고, 안와를 판찰할 수 있었띤 3 례중 2 례에서 안와의 영증성 변화가 동반되었마. 정동액 -해연정액동류 5 례중 4례에서는 한측 해연정액동의 미만성 팽창파 아울러 강한 균질성 조영증강을 보였고 쿠불구불하게 확장된 상안정액 (superior ophthalmic vein) 을 관찰할 수 있었£며 특정석으로 2 례에서는 3차 신경절 등의 정상음영이 소질되어 있었마. 양성종양 5 례중 4 례에서 는 해 연정액동에 국한펀 구행종괴로 경계 가 뚜렷하고 주위골변화가 없거 냐 골칭식 (bone erosion) 또는 골갱화 (bone sclerosis) 를 보이는 것이 특정석이었고, 악성전이성 종양에서는 6 례중 5례에서 골파괴 또 는 뱅밴의 두개낭내 미만성 파급 둥 뱅변의 악성성향을 시사하는 소견을 말견힐 수 있었다. 결론적우로 모든 례에서 득이한 조직학적 진단을 L~ 릴 수는 없지만 소수의 예외를 제외하고는 CT 소견만으혹 21 례 의 해연정액동 명변을 영증성질환, 헬판성질환, 양성종양 빛 악성건이성종양으로 구분지을 수 있었다.
횡단스캔은 판상스캔에 비해 해연정액동 뱅소와 전후좌우 안정쿠조물과의 판계를 밝히고 안와연화 및 연판된 두개강내 명변을 찾는데 우월하였마. 직접 판상스캔은해연정액동내부의 신경헐판구조물의 평 가, 양쪽 해연정액동의 비교판찰, 뇌히수체와의 판계 빛 투개기저의 골변화를 판찰하는데 횡단스캔보 다 우월하였다. 따라서, 임상적으로 해연정액동의 명밴이 의심될때 횡안 및 직접판상 선산화단층촬영 을 모두 시챙하는 것이 바람직하다고 생각된다
Summary. We retrospectively analyzed CT scans 01 21 cavernous sinus lesions in an attempt to lind the CT lindings helplul to the differential diagnosis. With the integration 01 various CT lindings it was possible to categorize the lesions into inllammatory, vascular, benign neoplastic and malignant metastatic lesions with lew exceptions. Four 01 5 cases 01 septic cavernous sinus thrombophlebitis revealed unilateral or bilateral multiple irregular lilling delects in the enhancing cavernous sinus with or without orbital inllammatory change
• 경 상대 학교 의 파대 학 방사선파학교실
• Department of Radiologκ College of Medicine, Kyung 5ang National University 이 논운은 1988 년 1월 22 일에 접수하여 1988년 2월 24 일에 채택되었음.
Received January 29, 1988, Accepted March 16, 1988
- 201-
-大韓放射線醫學會誌: 第24 卷 第 2 號 1988-
Four of 5 cases of carotid-cavernous fistula demonstrated unilateral or bilateral diffuse bulging and homogeneous enhancement of cavernous sinus with obliteration of normallow densities of cranial verves and gasserian ganglion.
미 latation and tortuosity of superior ophthalmic vein were also associated. Four of 5 cases of benign neoplastic lesion showed well-circumscribed enhancing mass confined to cavernous sinus with pressure erosion or hyperostosis of adjacent bone. Five of 6 cases of malignant metastatic lesion showed various findings sug- gesting malignant nature such as destruction of adjacent bone or associated manifestation of intracranial spread‘
As compared with axial scan, coronal scan proved to be more sensitive in detection of subtle cavernous sinus expansion, and superior in evaluation of intracavernous neural structures, relationships with pituitary gland and osseous change of skull base. Axial scan, however, was superior in detection of associated orbital and intracranial abnormalities. Scans in both projections are needed in the evaluation of most cavernous sinus diseases
KEY WORDS; Cavernous sinus-computed tDmography
Introduction
Ophthalmplegia, complete or incomplete, usual- ly painful and commonly associated with sensory deficits in the first or second division of the trige- minal nerve, alerts the clinician to the presence of a pathologic process in the cavernous sinus1). The added finding of visual loss further localizes the lesion to the anterior cavernous sinus and orbital apex. Despite the anatomical specificity provided by the clinical findings
,
it is often difficult to diffe- rentiate local masses from non-mass lesions. This dilemma is attributable to the wide variety of dis- eases that affect this region and to their frequently overlapping clinical presentations2). That is, accu- rate etiologic diagnosis of the parasellar lesion is not made on clinical grounds but is contingent upon supplementary examinations, such as appro- priate blood tests, inspection of the nasopharynx, and radiographic studies.In the past, radiographic examination has been limited; skull films or conventional tomography have demonstrated only osseous change and sphe- noid sinus abnormality and angiography has delin- eated only the vascular components. However, with the introduction of high resolution(HR)CT, direct visualization of the neurovascular structures
within the cavernous sinus and accurate definition of its dural boundaries have been possible 3,4,5)
Now
,
CT findings of several cavernous sinus dis- eases have been reported and specific diagnosis of them has been possible on occasionZ-13).
Changes in size, density, and configuration of the cavernous sinus are useful findings in detecting abnormality by CT. Among these, contour bulging of lateral boundary is the most sensitive indicator of pathologic involvemene,4l. The purpose of this paper is to describe CT findings of various disea- ses causing cavernous sinus bulging and to eluci- date differential points in CT diagnosis
Materials and Methods
A retrospective review of all CT studies at the Seoul National University Hospital from January 1983 to December 1987 uncovered 21 cavernous sinus Iesions. These included 5 cases of septic cavernous sinus thrombophlebitis, 5 carotid-caver- nous fistulas, 5 benign neoplasms, and 6 malignant metastatic neoplasms(Table 1). Ten patients were male and eleven were female. Age ranged from 6 to 72 years. We excluded trigeminal neuroma with severe extension into middle and posterior cranial fossas
,
and lesions which arised from adjacent organ and secondarily invaded cavernousSH뼈
202 -
} 5 특gr nrζ그@-m〔 ∞- 〔。g건드@(} 、[。g 。m【∞〔〕r〕、。{ηα〈엌그(〕ζα mgzω [〕}@@∞ω@@|
Exophthalmos, prominent Abnormal thick ophthalmic vein enhancement of ipsilateral tentonum (-)
Associated Intracranial Abnormality Cerebellar abscess (-)
(-) (-) (-) (-)
(-) (-) (-) Exophthalmos, prominent ophthalmic vein
Exophthalmos, prominent ophthalmic vein Exophthalmos, prominent ophthalmic vein Prominent ophthalmic vein, bulbar wall thick- ening, EOM thickening, periorbital swelling Bulbar wall thickening, periorbital swelling
Orbital Change (-) (-) (-)
No scan
No scan Erosion of lateral wall of sphenoid sinus, and petrous apex
Bone Change (-) (-) (-) (-) (-) (-) (-) (-) (-) (-)
Enhancement Pattern Bilaterality Unilateral
Unilateral Unilateral
Unilateral Unilateral Unilateral
Unilateral Bilateral
Bilateral Bilateral Bilateral
CT Findings of Cavernous Sinus Homogeneous and isodense
Homogeneous and mtense Homogeneous and mtense Homogeneous and mtense Homogeneous and mtense
Homogeneous and mtense Multiple irregular filling defects Multiple irregular filling defects
Multiple irregular filling defects Multiple irregular filling defects Single large fill- ing defect Diffuse widening with slightly convex border Round mass with Round mass with smooth convex convex border border
Diffuse widening with straight border Diffuse widening with straight border Diffuse widening with straight border Diffuse widening with slightly concave border Diffuse widening with slightly convex border Diffuse widening with straight border Diffuse widening with straight border Diffuse widening with slightly convex border Diffuse widening with straight border
Coronal Contour Axial Contour Septic cavernous sinus thrombo phlebitis Septic cavernous sinus thrombo- phlebitis 34/ M Septic cavernous sinus thromb。 phlebitis Septic cavernous sinus thrombo- phlebitis Carotid-cavernous Smooth lateral fistula convex bulging
Smooth lateral convex bulging Smooth lateral convex bulging Smooth lateral convex bulging Carotid-cavernous Smooth lateral fistula convex bulging Carotid-cavernous Smooth lateral fistula convex bulging
Smooth lateral convex bulging Carotid-cavernous No scan fistula
No scan Cerotid-cavernous No scan fistula
Summary of the 21 Cases Benign neoplasm Trigeminal neunnoma
Septic cavernous sinus thrombo- phlebitis
Age & Diagnosis Gender 46/M 55/F 58/F 54/F 56/F 53/F 72/F 60/F 46/F 6/F
Table 1. Case N。 10 5 6 8 9 2 3 4 7 11
t'V ζ〉 μJ
Associated Intracranial Abnormality
CT Findings of Cavernous Sinus Age & Diagnosis Gender
Orbital Change Bone Change Case No Enhancement Pattern Bilaterality Coronal Contour Axial Contour (-) ]/
(-) (-)
lu가짧냥옆앓빼빼깨뼈뼈빼애야” W생NA뺑
(-) (-) (-)
니
/(-) No scan
Erosion of poste- rior clinoid, lateral wall of sphenoid sinus H yperostosis of posterior clinoid, lateral wall of sphenoid sinus Destruction of orbital apex, posterior ethmoid (-)
(-) Unilateral Unilateral
Ring enhancement Homogeneous and isodense
Round mass with convex border Round mass with Round mass with smooth convex convex border border
No scan Benign neoplasm Trigeminal neunnoma Benign neoplasm Cavernous hemangioma
191M 421F
12 13 Unilateral Homogeneous and isodense with central low density
Round mass with Diffuse widening smooth convex with straight border border
Benign neoplasm Meningioma 45/F 14 Unilateral Unilateral Subdural spread No scan (-) Unilateral Homogeneous and isodense
@얘 N 뽕
Another supra- sellar mass
(-) (-) Unilateral Homogeneous and isodense } 잉∞∞ j (-) No scan
」l
(-) Direct invasion into temporal lobe, meningeal spread
Homogeneous and isodense Homogenous and isodense (-)
Destruction of dorsum sellae, lateral wall of sphenoid sinus Destruction of orbital apex, posterior ethmoid (-)
Unilateral Homogeneous and isodense
Diffuse widening with straight border Round mass with smooth convex border Round mass with Diffuse widening smooth convex with slightly border convex border Round mass with No sc뻐 smooth convex border Smooth lateral convex bulging
No scan No scan
Benign neoplasm Eosinophilic granuloma Metastatic ca From salivary gland Metastatic ca Lymphoma
6/M 301M
15 16
l N()A | 121M 17 Diffuse widening with straight border
Metastatic ca Germ cell tumor Metastatic ca From para nasal sinus
151M 18 281M 19 Unilateral Inhomogeneous Unilateral Homogeneous and isodense
Diffuse widening with straight border Irregular mass with fuzzy border
Smooth lateral convex bulging
Metastatic ca Lung cancer 54/M 20 Irregular mass with fuzzy border Metastatic ca From naso- pharynx
391M 21
- Jin Wook Chung, et al.: Computed Tomography 01 Cavernous Sinus Diseases
gioma of sphenoid wing and petrous apex, metas- tasis to skull base, chordoma, chondroosseous tumor of skull base, etc).
Their diagnosis was confirmed by biopsy in tumors, by angiography in vascular lesions, and by clinical manifestation in septic cavernous sinus thrombophlebitis. Biopsy was not performed in cases of metastatic disease with known primary slte.
AIl patients were scanned on GE CT /T 8800 and / or 9800 scanners with variable thickness from 1.5mm to 5mm. Sixteen patients were scanned in both axial and coronal planes, four in axial plane only
,
and one in coronal plane only. In the major- ity of cases, only contrast enhanced scans were obtained after bolus injection of 60ml of Telebrix 30(iodine content 18gm) followed by drip infusion of 100ml of Telebrix 38(iodine content 38gm).The CT scans were retrospectively analyzed in viewpoint of pattern of enhancement, bilaterality, configuration of boundary of cavernous sinus
,
adjacent bone change
,
orbital change,
and asso- ciated intracranial abnormality. In 16 cases, it was possible to evaluate orbit.Result
The CT findings of all 21 cases were summari- zed in Table 1.
1. Septic cavernous sinus thrombophlebitis(5 cases)
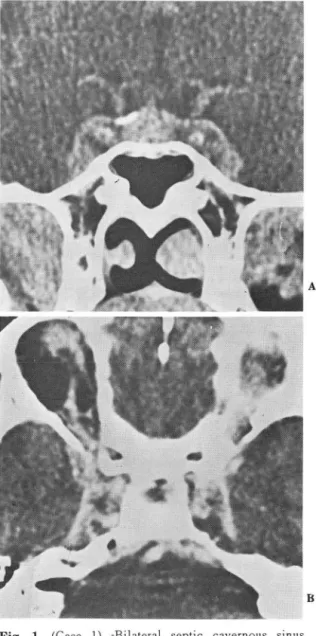
In all cases, direct visualization of septic throm- bi was possible; four cases showed multiple irre- gular filling defects(Fig. 1) and one case showed single large filling defect(Fig. 2) in the enhancing cavernous sinus. They ranged roughly from 3mm to lOmm in size. Lateral boundary of the sinus was sharp, smooth and showed diffuse bulging in all cases. Three cases showed bilaterality. The other two case were left-sided. Orbital changes were associated in two out of three cases in which orbital scans were performed. Orbital abnor-
Fig. 1. (Case 1) -Bilateral septic cavernous sinus thrombophlebitis with multiple defects A. Coronal enhanced scan shows lateral bulging
of both cavernous sinuses and irregular enhan- cement with irregular delects. Lateral wall of cavernous sinus, intracavernous internal caro.
tid artery and pituitary gland enhance more intensely than the rest 01 the cavernous sinus B. Axial enhanced scan shows widening of both
cavernous sinuses, irregular filling defects,
and linear enhancement of lateral wall of the sinus. Note that lateral borders of both caver- nous sin uses appear straight, but not convex Subdural extension along greater wing of spe noid and dilated superior ophthalmic vein in right orbit are also demonstrated
- 205-
A
B
-大韓放射線醫學會註、. 第24 卷 第 2 號 1988-
malities included tortuous dilated superior ophthalmic vein, thickening of extraocular muscle, bulbar thickening with fuzzy border, periorbital swelling, and increased soft tissue strands at retro- bulbar fat. There was apparent discrepancy in de- gree of bulging between coronal and axial scan.
On . coronal scan convex bulging of lateral boun- dary was evident
,
but on axial scan it was rather straight in all cases. Instead, there was diffuse widening of the involved cavernous sinus on axial scan. In three cases of extensive cavernous sinus thrombosis, intracavernous carotid artery and pitu- itary gland showing norrnal enhancernent were readily identified within thrombosed cavernous sinus by density difference(Fig. 1-a). Cerebellar abscess was associated in a case with rnycotic aneurysrn of intracavernous carotid artery. No adjacent bony abnorrnality was found.2. Carotid-cavernous fistula(including direct in- ternal carotid-cavernous fistula and dural AVM of cavernous sinus; 5 cases).
All cases showed hornogeneously intense εnhan
cernent of bulging cavernous sinus with non-vi- sualization or smaller size of normal low densities of intracavernous cranial nerves and gasserian gan- glion. One case was bilateral(Fig. 3) and four cases were unilateral(Fig. 4). The lateral wall of involved cavernous sinus was sharp andsrnooth in all cases. There was discrepancy in appearance of the sinus bulging between coronal and axial scan.
On coronal scan lateral boundary showed convex lateral bulging, but on axial scan it appared widen ed but remained rather straight or slightly convex in lateral border. Degree of bulging seems to be related with amount of shunting. In two cases of large carotid-cavernous fistula, ipsilateral gasse- rian ganglion was obliterated(Fig. 4). In four cases, orbital changes including proptosis, enlar gernent of ophthalrnic vein and thickening of ex traocular muscle were associated(Fig. 4). The case without orbital change had small dural A VM on angiography. Abnormal thick enhancement of ipsi-
- 206
’
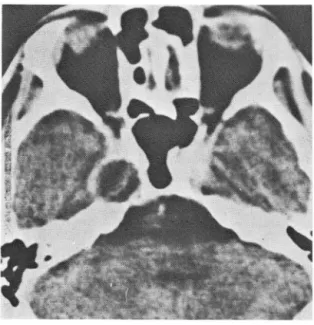
Fig. 2. (Case thrombophlebitis 5) -Unilateral with septic single defect cavern* ‘-。따’·
sinus B A. Coronal enhanced scan shows unilateral convex bulging of left cavernous sinus with large single filling defect. Low density of oculo.
motor nerve within left cavemous sinus is also obliterated
B. Axial scan shows unilateral widening of left cavernous sinus with slightly concave lateral border. The filling defect in left cavernous sinus appears not well defined and not separa ble from normal area probably due to partial volume averaging
A
- Jin Wook Chung, et al.: Computed Tomography of Cavernous Sinus Diseases-
Fig. 3. (Case 6) -Bilateral carotid-cavernous fistula A. Coronal enhanced scan shows convex lateral
bulging and homogeneous enhancement 01 both cavernous sinuses
B. Axial enhånced scan shows bilateral expan- sion 01 cavernous sinus with mild convexity
。1 lateral border and intense homogeneous en hancement. Note that the low density area 01 gasserian ganglion is obliterated
lateral tentorium was assoicated in one case of dural A VM. No adjacent bony abnormality was found.
3. Benign neoplastic lesion(5 cases)
Five cases of benign neoplastic lesion inc\uded
two trigeminal neurinomas, a meningioma, a eosi- nophilic granuloma, and a cavernous hemangioma.
All cases were unilateral and their lateral border was sharp and smooth. Except a ring-enhancing trigeminal neurinoma(Fig. 5), all other four tumors showed homogeneous isodense enhan- cement compared with the density of pituitary gland or contralateral cavernous sinus. The mases appeared not separable from normal portion of the sinus and obliterated normal intracavernous neural structures. Three cases(two trigeminal neurinomas and a cavernous hemangioma) showed round mass expanding cavernous sinus with smooth convex border on both axial and coronal scans. In a meningioma and a eosinophilic granu- loma, the involved sinus showed diffuse widening and straight lateral border on axial scan but round mass-like appearance with convex border on coronal scan(Fig. 6). In four cases, abnormality of adjacent bone was observed; pressure erosion at lateral wall of sphenoid sinus and petrous apex in
Fig. 4. (Case 7)-Unilateral carotid-cavernous fistula Axial enhanced scan shows unilateral widening 01 right cavernous sinus with intense enhan- cement. The low density 01 right gasserian gan- glion is obliterated. Ipsilateral exophthalmos and thickening 01 extraocular muscle are als。
noted - 207-
-大轉放射線홉學會誌 : 第 24 卷 第 2 號 1988-
Fig. 5. (Cases 12)-Trigeminal neurinoma
Axial enhanced scan shows round mass with ring-enhancement at right Meckel’s cave area
a trigeminal neurinoma, pressure erosion at post- erior c1inoid process and lateral wall of sphenoid sinus in a cavernous hemangioma, hyperostosis at posterior c1inoid process, and lateral wall of sphe- noid sinus in a meningioma(Fig. 6), irregular focal destruction of sphenoid bone at orbital apex and planum sphenoidale, and posterior ethmoid air cells in a eosinophilic granuloma. There was no orbital change.
4. Malignant metastatic Iesion(6 cases)
Primary sites of six metastatic lesions were as follows; a nasopharyngeal cancer, two adenoid cystic carcinomas of paranasal sinus and salivary gland, a lung cancer, a Iymphoma, and a ectopic germinoma. AIl cases revealed unilateral bulging of the cavernous sinus. Four cases were left-sided and two cases were right-sided. Pattern of enhan- cement was homogeneously isodense in four cases(two adenoid cystic carcinomas of salvary gland and paranasal sinus, a ectopic germinoma, a nasopharyngeal cancer), homogeneously hypodense in a lymphoma(Fig. 7) and slightly inhomogeneous in a metastatic lung cancer. Later-
al wall was fuzzy and indistinct only in the metas- tatic Iesion of nasopharyngeal cancer. The other five cases showed sharp and smooth lateral mar- gin. Metastatic lesion without bone destruction showed round mass expanding cavernous sinus on both axial(Fig. 8) and coronal scans. Metastatic
Fig. 6. (Case 14)-Meningioma
Coronal(A) and axial(B) enhanced scans show convex lateral bulging and diffuse widening of left cavernous sinus, respectively. There is hyperostosis at greater wing of sphenoid bone,
posterior clinoid process and lateral wall of sphenoid sinus
- 208-
A
B
Jin Wook Chung, et al.: Computed Tomography of Cavernous Sinus Diseases-
Fig. 7. (Case 17)-Malignant Iymphoma
Coronal enhanced scan shows expansion of right cavernous Slnus with homogeneously hypodense enhancement relative to the lateral dural wall and internal carotid artery
Fig. 8. (Case 16)-Metastatic lesion from adenoid cystic carcinoma of salivary gland. Axial enhanced scan . demonstrates homogeneously enhancing round mass without definite bone change
Fig. 9. (Case 20)-Metastatic lesion from lung cancer Axial enhanced scan shows hypodensely en- hancing mass in widened left cavernous sinus, orbital apex and posterior ethmoid air cells with adjacent bony destruction. Lateral border is slightly concave in spite of extensive invol- vement
lesions with bone destruction(a adnoid cystic carci- noma of paranasal sinus, a lung cancer) showed diffuse widening of the involved cavernous sinus and rather straight lateral margin on axial scan- (Fig. 9) in contrast to convex bulging on coronal scan. Focal bone destruction was found at dorsum sellae and lateral wall of sphenoid sinus in a metastatic adenoid cystic carcinoma of paranasal sinus, and at orbital apex, sphenoid sinus and pos- terior ethmoid air cells in a metastatic lung cancer.
Various intracranial abnormalities were associated;
direct parenchymal invasion into temporal lobe in a nasopharyngeal cancer, sheet-like meningeal en- hancement suggesting meningeal spread in a lym- phoma and a nasopharyngeal cancer, and a sepa- rate suprasellar mass with no apparent connεctiO n
to the sinus lesion in a ectopic germinoma.
209 -
-大韓放射線뿔學會誌 ; 第24 卷 第 2 號’ 1988-
Discussion
The cavernous sinus is one of the dural venous sinuses located between the meningeal and perio- steal layers of the dura and contains trabeculated network of venous channels, intracavernous por- tion of internal carotid artery, and cranial nerve- s(oculomotor nerve, trochlear nerve, abducens nerve, ophthalmic division of trigeminal nerve and gasserian ganglion)3,14l. Consequently
,
diseases of the cavernous sinus can be classified into inflamm- atory(e.g., cavernous sinus thrombophlebitis), vas- cular(e.g., fistula, aneurysm), and neoplastic lesion(e.g., neurinoma, meningioma, metastatic tumor). No matter what the cause is, it leads to volume expansion of the involved cavernous sinus,
demonstrating bulging of lateral boundary of the cavernous sinus on CT. If the disease process is unilateral, lesion of the cavernous sinus is easily detected by asymmetricity. Both cavernous sinuses are connected by intercommunicating venous channels, which provide the route of disease spread into contralateral side and explain bila- terality of some cavernous sinus lesions.
For evaluation of cavernous sinus by CT it is essential to perform intravenous contrast enhan- cement. Amount of contrast media should be large enough to enhance the cavernous sinus and pitui- tary gland adequately. Contrast enhancement highlights cavernous sinus and its dural boundary in degree similar to internal carotid artery and pituitary gland, but not the Meckel’s cave and intracavernous cranial nerves. Intracavernous in- tracranial nerves are seen as low attenuation areas at specific location of cavernous sinus along its anatomical course3). Among these, κ1eckel’s cave and oculomotor nerve are consistently visible and usually symmetric. They can be obliterated by any kind of disease that involves cavernous sinus. Non- visualization of normal low density of Meckel’s cave within homogeneously enhancing cavernous
-210
sinus seems to be one of the important CT fin- dings suggesting carotid-<.:avernous fistula, because it may manifest as subtle expansion of cavernous sinus as those of our cases 9 and 10.
If not dynamic scan, prominent linear enhan- cement of dural lateral border or identification of intracavernous carotid artery or pituitary gland by density difference suggests abnormal enhancement of entire cavernous sinus and can be a sign helpful to the detection of cavenrous sinus disease. 1n our series
,
3 cases of septic thrombophlebitis and one case of lymphoma show this CT finding(Fig. 1-a, Fig. 7).Besides the contrast enhancement, the other technical factors of CT scan such as section thick- ness and planes are crucial for the detection of small lesion of cavernous sinus. The section thick- ness is advised to be 1.5-3.0mm for avoiding par- tial volume effects, even though the lesions were seen with 5mm thickness in our some cases. Which projection of scanning is superior, coronal or axial? Coronal scan is more sensitive in detection of subtle cavernous sinus expansion, easier to compare both cavernous sinuses, and superior in evaluation of intracavernous neural or vascular structures
,
relationship with pituitary gland and osseous change of skull base. Axial scan is superi- or in display ofaxial relationship with adjacent structures and in detection of orbital change or intracranial abnormality. Scans in both projections are needed for complete evaluation of cavernous sinus disease. 1n our series, a thrombus was more clearly visible on coronal scan(Fig. 2), while meningeal spread was seen only on axial scan in Iymphoma patient. All of the cavernous sinus le sions showed convex bulging of lateral border on coronal scan only with difference in degree, but configuration of cavernous sinus on aixal scan is greatly different between different etiologies, which is thought to be helpful in differential di- anosis. Neoplastic lesions without bone destruction or meningeal spread usually showed round mass- Jin Wook Chung, et al.: Computed Tomography of Cavernous Sinus Diseases-
expanding cavernous sinus on both axial and coronal scans, which might be due to confinement of the mass within the dural boundary of the sinus. But, destruction of adjacent bone or menin- geal spread in neoplastic lesion caused disruption of dural confinement of the neoplasm, leading to loss of round convexity of lateral border. 1n in- flammatory or vascular lesion of cavernous sinus, involved sinus was diffusely expanded and its lateral boundary remained to be rather straight on axial scan.
There are many causes that show filling defects within enhancing cavernous sinus. Partial or com- plete thrombosis of cavernous sinus
,
neurinomas of intracranial nerves, intracavernous metastasis, and spontaneous aseptic thrombosis of the caver- nous sinus in a preexisting carotid-cavernous fistu- la may all demonstrate abnormal low attenuation values within the enhancing cavernous sinus8)But
,
in our series m비 tiple irregular filling def,εctswithin the enhancing cavernous sinus were found solely in septic cavernous sinus thrombosis and seems to be specific finding. The filling defects due to septic thrombi are irregular and do not correspond to the anatomic course of neural struc- tures. Additionally, air in the cavernous sinus can be a sign of septic cavernous sinus thrombosis9)
,
but not seen in our cases. Fatty tissue also appears as low attenuation value within the cavernous sinus in normal person or in association with Cushing disease8). Neoplasms with inhomogeneous or little enhancement should be differentiated from inflammation. But, it is not difficult to diffe- rentiate them because neoplastic lesion usually shows focal bulging, unilateral involvement and bony change.
Bilateral involvement is usually demonstrated in cavernous sinus thrombophlebitis or carotid-caver- nous fistula as those in our series. Bilateral caver- nous sinus involvement may also be seen in bila- teral neurogenic tumors such as trigeminal neuri- noma in neurofibromatosis and bilateral metastatic
lesions2). But, they are very rare diseases. Abnormality of adjacent bone was also very helpful in differential diagnosis. Bone destruction and pressure erosion usually indicate malignant and benign neoplastic nature of the lesion, resp- ectively. But
,
there are exceptions. Benign neo-이asm such as eosinophilic granuloma may show gross bopy destruction as shown in our case 15.
Also, the carotid-cavernous fistula can cause en- largement of superior orbital fissure by pressure erosion. Hyperostosis adjacent to the bulging cavernous sinus is characteristic of meningioma 13)
Orbital changes are usually associated with only cavernous sinus thrombosis and carotid-cavernous fistula, but not with the neoplasm. Dilatation and tortuosity of superior ophthalmic vein is the hall- mark of the carotid
•
avernous fistula, even though it may be associated with other conditions such as orbital venous malformation and varices, and vascular tumor7). Other orbital abnormalities such as thickening of extraocular muscle,
bulbar wall thickening with fuzzy border, periorbital swelling, and increased soft tissue strands at retro- bulbar fat are nonspecific and may be found in Grave’s ophthalmopathy, orbital cellulitis, acute orbital pseudotumor, etc. These lesions, however, usually demonstractes normal cavernous sinus. No neoplastic lesion of our cases was associated with orbital change.Associated intracranial abnormality can also assist to make a correct differential diagnosis and lead to specific diagnosis on occasion, as those of our cases 4,9,17,18 and 21. Cavernous sinus invol- vement in ectopic germinoma( case 18) might be caused by cisternal drop metastasis at subarach- noid -space around gasserian ganglion
Most difficult situation to judge the nature of the lesion is benign-Iooking tumorous lesion which is demonstrated as well circumscribed mass with uniform enhancement on CT. Magnetic resonance imagíng may be greatly useful in the differential diagnosis of these patients, even thgough there are - 211-
-大韓放射線훌훌學會註 : 第24 卷 第 2 號 1988-
only a few descriptions in the literature to date. Angiography is essential for the verification of the carotid-cavernous fistula and intracavernous aneurysm and is usually hεlpful to the diagnosis of meningioma or cavernous hemangioma. With no aid of angiography, there are still diverse possi- bilities including trigeminal neurinoma, menin- gioma without hypervascularity, chronic granulo- matous lesion \0), and metastasis. However, com- bined analysis of all the radiologic examinations in association with clinical and neurologic symptoms lead to correct preoperative diagnosis in most of the patients.
REFERENCES
5. Kapila A, Chakeres DW, Blanco E(1984) The Meck el cave; computed tomographic study. Radiology 152.425'433
6. Bonneville JF, Cattin F, Dietemant JL(1986) Com.
puted tomography o[ the pituitary gland. Springer, Berlin Heidelberg New York, pp 205.212 7. Ahmadi J, Teal JS, Segall HD, Zec CS, Han JS,
Becker JS(1983) Computed tomography o[ carotid' cavernous fistula. A]NR 4:131,136
8. Ahmadi J, Keane JR, Segall HD, Zee CS(1985) CT observations pertinent to septic cavernOUS sinus thrombosis. A]NR 6:755,758
9. Curnes JT, Creasy JL, Whaley RL, Scatliff JH(1987) Air in the cavernous sinus; a new sign of septic cavernous sinus thrombosis. A]NR 8:176,177 10. Atri M, Robertson WD, Durity F A, Dolmn CL(1987) Actinomycotic granuloma of the trige
1. Thomas JE, Yoss RE(1970) The parasellar syn. minal ganglion. A]NR 8:167'169
dorme: problems in determining etiology. Mayo 11. Raymond J. Therson J(1986) Intracavernous aneur.
CJin Proc 45:617,623 ysm; treatment by proximal balloon occlusion of the 2. Post MJ, Mendez DR, Kline LB, Acker JD, Glaser internal carotid artery. A]NR 7:1087,1092
JS(1985) Metastatic diseases to the cavernous 12. Goldberg R, Byrd S, Winter J, Takahashi M, Joyce sinus; clinical syndrome and CT diagnosis. J Com. P(1980) Varied appearance of trigeminal neuroma put Assist Tomogr 9:115'120 on CT. A]R 134:57'60
3. Kline LB, Acker JD, Post MJ. Vitek ]](1981) The 13. Post MJ, Glaser JS, Trobe JD(1978) The radio.
cavernous sinus; a computed tomographic study. graphic recognition o[ the two clinically elusive
A]NR 2:229'305 mass lesions of the cavernous sinus; meningiomas
4. Hasso AN. Pop PM‘ Thompson JR, et al.(1982) and aneurysms. Neuroradiology 16:499'503 High resolution thin section computed tomography 14. Umansky F, Nathan H(1982) The lateral wall o[ the o[ the cavernous sinus. Radiographics 2:83,100 cavernous sinus. ] Neurosurg 56:228'234
- 212-