Received: September 12, 2015 Revised: September 26, 2015 Accepted: October 15, 2015
Corresponding Author: Sung-Soo Kim, Department of Orthopedics, Inje University Haeundae-Paik Hospital, 875, Haeun-daero, Haeundae-gu, Busan 48108, Korea
Tel: +82-51-797-0240, Fax: +82-51-797-0249, E-mail: [email protected]
선택적 에스트로겐 수용체 조절제: 작용 기전 및 임상 자료의 고찰
인제대학교 의과대학 해운대백병원 정형외과학교실
김 성 수
Selective Estrogen Receptor Modulators:
A Review of Action Mechanism and Clinical Data
Sung-Soo Kim
Department of Orthopedics, Inje University Haeundae-Paik Hospital, Busan, Korea
Selective estrogen receptor modulators (SERMs) are a diverse group of synthetic non-steroidal compounds that have various levels of estrogen receptor (ER) agonist or antagonist activity depending on the target tissue. This feature of SERMs could be explained by the differential expression of two ER isoforms (ERα or ERβ), the differential ER conformational change and the differential coregulatory proteins (coactivator or corepressor) in a selected tissue. Based on their efficacy and safety, SERMs have been used for the prevention and treatment of breast cancer (tamoxifene and toremifene), prevention and treatment of osteoporosis (relaoxifene and bazedoxifene), treatment for dyspareunia related to vulvovaginal atrophy (ospemifene) and treatment for vasomotor symptoms associated with menopause (tissue selective estrogen complex; TSEC). Many of the available SERMs are well-known for their anti-estrogenic effects in breast and for their estrogenic effects in bone. The effect on the endometrium have played a key role in differentiate SERMs in clinical practice. The effect of SERMs in the vagina also shows clear distinction among different SERMs. This review summarizes their action mechanism and describes their clinical findings in different target tissues. In the osteoporosis treatment, SERMs such as raloxifene and bazedoxifene is a safe and effective option for women who cannot tolerate or are unwilling to take bisphosphonates and may be appropriate for younger woman with the age of ≤70 years old who expect to remain on therapy for many years and are concerned about the long-term safety of bisphosphonates.
Key Words: Agonist, Antagonist, Estrogen receptor, Osteoporosis, Selective estrogen receptor modulator
선택적 에스트로겐 수용체 조절제(selective estro- gen receptor modulator; SERM)는 특정 조직에서는 에스트로겐 작용제(estrogen agonist)로 작용하지만, 다른 조직에서는 에스트로겐 길항제(estrogen anta- gonist)로 작용하는 합성의 비호르몬성 제제이다.
1-5폐경 후 여성은 난소에서 생성되는 에스트로겐의 중
단으로 인해 안면 홍조와 같은 혈관운동 증상, 질이
나 비뇨생식기의 위축, 연부 조직과 피부의 위축, 골
다공증 등의 여러 증상들이 발생한다. 이런 증상을
해결하기 위해 사용되었던 호르몬 치료(hormonal
Fig. 1. Classification and chemical structures of SERMs
therapy)는 자궁이 없는 환자에게는 에스트로겐을, 자궁이 있는 환자에게는 에스트로겐과 프로게스틴 (progestin)를 투여하는 것이었다. 이 호르몬 치료가 앞에서 언급한 여러 증상을 호전시켰을 뿐만 아니라 골재형성(bone remodeling)을 정상화시키고 척추 골 절과 비척추 골절의 위험을 감소시켜 골다공증에 효 과적인 치료법으로 여겨졌지만, 2002년 WHI (Womens’ Health Initiative) 연구에서 유방암, 뇌졸증 과 같은 뇌혈관 질환 및 정맥 혈전 색전증을 증가시 킨다는 것이 알려지면서
6더 이상 골다공증의 일차 치료약으로 고려되지 않고 있다.
에스트로겐처럼 체내에 존재하는 에스트로겐 수용 체(estrogen receptor; ER)에 결합하지만, 조직마다 다 르게 즉, 어떤 조직에서는 작용제의 역할을 하고, 다 른 조직에서는 길항제의 역할을 하는 약물이 존재한 다는 것을 알게 된 것은 타목시펜(tamoxifene)의 연 구에 의해서였다. 타목시펜은 1세대 SERM으로 처 음에는 피임약으로 개발되었지만 실패하였고, 유방 조직에서 ER와 결합하여 길항제로 작용하여 유방암 을 감소시키는 것이 확인되면서 현재에는 유방암의 예방과 치료에 사용되고 있다. 2세대 SERM인 랄록 시펜(raloxifene)은 유방암에 대한 치료제로 개발되었 으나, 골 조직의 에스트로겐 수용체에 작용제로 작 용하여 골 소실을 감소시켜는 효과가 알려지면서 현 재에는 골다공증의 예방과 치료에 사용되고 있다. 3 세대 SERM으로 라소폭시펜(lasofoxifene), 바제독시 펜(bazedoxifene), 오스페미펜(ospemifene)이 있으며 바제독시펜은 골다공증 약물로, 오스페미펜은 폐경 으로 인한 외음질 위축(vulvovaginal atrophy)으로 인 한 성교통(dyspareunia)에 대한 약물로 사용되고 있 다.
2SERM의 분류
SERM은 에스트로겐과 화학 구조가 같지 않지만 ER와 결합하여 효과를 나타내는 다양한 합성물로 구성되어 있으며, 화학 구조에 따라 크게 triphen- yethylene, benzothiophene, naphthalenol, benzopyran, indol로 나눌 수 있다. Triphenyethylene계에는 클로미 펜(clomiphene), 타목시펜, 토레미펜(toremifene), 오스 페미펜이, benzothiphene계에는 랄록시펜이, naphtha- lenol계에는 라소폭시펜이, indol계에는 바제독시펜 이 있다(Fig. 1).
1SERM의 작용 기전
서로 다른 SERM 제제가 조직에 따라 어떻게 에 스트로겐 작용제나 길항제로 나타나는지는 현재까 지도 명확하게 정립되지는 않았으나, 몇 가지 기전 들이 알려져 있다. 흡수된 SERM 제제가 세포내의 에스트로겐 수용체(estrogen receptor; ER)에 결합하 면 ER은 삼차원적인 입체구조 변화(conformational change)가 일어나고, ER 2개가 모여 이합체(dimer)를 이룬다. 우리 몸에는 ERα와 ER β 로 명명된 2개의 ER가 있으며, 조직에 따라 서로 다른 비율로 나타난 다. ERα가 ERβ보다 여러 조직에 광범위하게 분포 하며, 뼈에서는 두 가지가 모두 존재하고 자궁에서 는 주로 ERα가 존재한다. 일반적으로 ERα 비율이 높으면 세포 활성이 증가되고 ERβ의 비율이 높으면 세포 활성이 감소하는 것으로 알려져 있다.
7,8이합체 를 구성한 ER complex는 핵 내로 이동하여 보조 인 자(cofactor, coregulator)와 합쳐지는데, 이 보조 인자 에 의해 특정 유전자의 발현이 또한 결정된다. 즉 보 A. Triphenylethylenes B. Benzothiophene C. Naphthalenols D. Indoles
Tamoxifene Ospemifene Raloxifene Lasofoxifene Bazedoxifene
Fig. 2. Action mechanism of SERMs. Pure agonists allow the estrogen receptor (ER) to interact with only coactivators (CoA) while pure antagonists with only corepressors (CoR). SERMs permit ER complex to interact with different subsets of CoAs and CoRs, determined by the overall conformation of ER and thereby these drugs have different activities in different tissues. ERE; estrogen responding element.
Fig. 3. Important cytokines in the bone that regulate osteoclast (OC) function. Osteoprotegerin (OPG; soluable decoy receptor of RANKL) and transforming growth factor-β (TGF-β) are inhibitory factors (with thin dotted line) and the others are stimulatory factors (with thin solid line). Having positive (+) or negative (-) effects on these regulatory factors, SERMs decrease OC differentiation and activity and increase OC apoptosis. IL; interleukin, TNF; tumor necrosis factor, NF-κB; nuclear factor kappa-light-chain-enhancer of activated B cells, RANKL; receptor activator of NF-κB ligand, RANK; receptor activator of NF-κB, JNK; c-Jun N-terminal kinase, PGE; prostaglandin-E, GM-CSF; granulocyte macrophage-colony-stimulating factor, M-CSF; macrophage-colony-stimulating factor.
조활성 인자(coactivator)와 결합하면 유전자 전사 (gene transcription)가 일어나 세포 활성이 증가되는 반면, 보조억제 인자(corepressor)와 결합하면 유전자
전사가 억제되어 세포 활성이 감소된다(Fig. 2).
9보
조 인자는 알려진 것만해도 현재까지 300개 이상 있
으며, 1~2개의 보조 인자가 아닌 여러 개의 보조 인
Fig. 4. A new mechanism of SERMs in bone. The protective actions of SERMs in bone can be partly attributed to its ability to increase the expression of small heterodimeric partner (SHP) in preosteoblasts. This protein are a negative regulator of the LXR/RXR, which itself increase bone loss by upregulating the expression of genes associated with osteoclasto- genesis. The 27-hydroxycholesterol (27HC), which is a cholesterol metabolite, can act as both an inhibitor of estrogen receptor (ER) and an activator of LXR.
E2; estradiol, LXR; liver X receptor, RXR; retinoid X receptor.
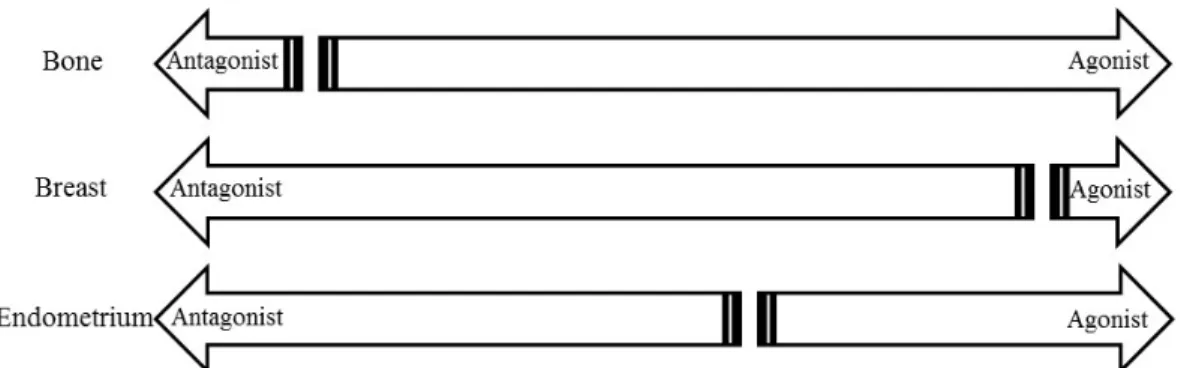
Fig. 5. Activity of SERMs in different target tissues. SERMs exhibit a spectrum of activities in estrogen target tissues.
자가 ER complex에 작용하여 유전자 전사를 결정하 는 것으로 이해되고 있다.
10이와 같은 유전자 경로 (genomic pathway)외에도 SERM은 세포막이나 세포 내의 ER와 결합하는 비유전자 경로(non-genomic pathway)를 통해 세포 활성에 영향을 주기도 한다.
결국, SERM 제제가 여러 조직에서 다양하게 반응
이 나타나는 이유는 조직마다 다른 ERα와 ERβ의 분포, 결합된 ER의 입체 구조 변화의 차이, 보조 인 자의 차이, 세포 환경의 차이에 의해 발생된다고 할 수 있다. 이중에서 특히 특정 조직에 존재하는 보조 인자가 유전자 전사 발현에 중요한 역할을 하는 것 으로 알려지게 되면서, 우리 몸에서 에스트로겐이 좋은 효과를 보이는 조직에서는 ER complex에 보조 활성 인자가 결합하여 작용제(agonist)로 작용하게 하고, 나쁜 효과를 보이는 조직에서는 ER complex에 보조억제 인자가 결합하여 길항제(antagonist)로 작용 하게 하는 물질에 대한 연구를 체외에서 분자 분석 (in vitro molecular assay)을 이용하여 시행하게 되었 다. 라소폭시펜과 바제독시펜은 이런 방법으로 개발 된 3세대 SERM이다.
11SERM은 일반적으로 뼈에서는 ER 작용제로 작용
하여 파골세포(osteoclast)의 분화와 활동을 직접적으
로 억제시키고 조골세포(osteoblast)의 증식과 활동을
촉진시킨다.
12SERM은 파골세포의 분화와 활동에
주요한 사이토카인(cytokine)인 T세포에서 분비되는
TNFα (tumor necrosis factor alpha)와 조골세포에서
분비되는 RANKL (receptor activator nuclear factor κB
ligand)를 감소시키고, 조골세포에서 분비되는 OPG
(osteoprotegrin)를 증가시켜 RANKL를 불활성화시킨
다.
13이런 작용으로 파골세포형성(osteoclastogensis)
이 억제되어 골흡수가 저하된다(Fig. 3). 최근 SERM
의 뼈에 미치는 구체적인 작용 기전이 고콜레스테롤
혈증(hypercholesterolemia) 연구에서 보고되었다. 고
콜레스테롤혈증은 폐경 여성에서 골다공증의 위험
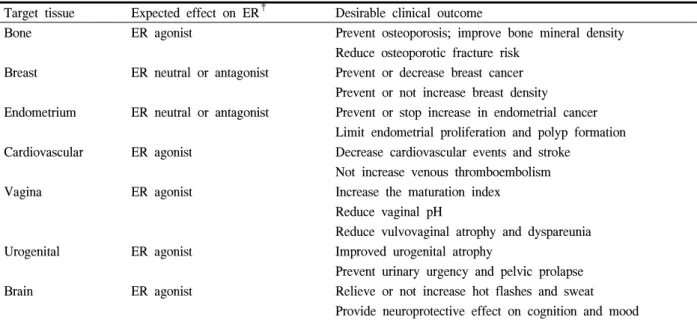
Table 1. The ideal SERM
†Target tissue Expected effect on ER
‡Desirable clinical outcome
Bone ER agonist Prevent osteoporosis; improve bone mineral density Reduce osteoporotic fracture risk
Breast ER neutral or antagonist Prevent or decrease breast cancer Prevent or not increase breast density Endometrium ER neutral or antagonist Prevent or stop increase in endometrial cancer
Limit endometrial proliferation and polyp formation Cardiovascular ER agonist Decrease cardiovascular events and stroke
Not increase venous thromboembolism
Vagina ER agonist Increase the maturation index
Reduce vaginal pH
Reduce vulvovaginal atrophy and dyspareunia
Urogenital ER agonist Improved urogenital atrophy
Prevent urinary urgency and pelvic prolapse Brain ER agonist Relieve or not increase hot flashes and sweat
Provide neuroprotective effect on cognition and mood
†
SERM: Selective estrogen receptor modulator,
‡ER; Estrogen receptor.
인자로, 이것은 콜레스테롤 대사물인 27-OH 콜레스 테롤(27-hydroxycholesterol)에 의해 LXR (liver X receptor)를 증가되고, 증가된 LXR은 조골세포에서 RXR (retinoid X receptor)와 결합하여 RANKL의 분 비를 촉진시켜 골흡수가 일어나기 때문이다. SERM 은 ER에 작용하여 유전자 전사를 통해 SHP (small heterodimeric partner) 발현시키고, 이 SHP가 LXR과 RXR에 결합하여 그 작용을 억제함으로써 골흡수를 저하시킨다(Fig. 4).
14이상적인 SERM (ideal SERM)
SERM 제제가 뼈, 뇌, 심혈관계, 질, 비뇨생식기계, 피부와 같은 조직에서는 에스트로겐 작용제의 활동 을 보이고, 유방, 자궁내막, 골반저(pelvic floor), 정맥 혈전에서는 중립적이거나 에스트로겐 길항제의 활 동을 보인다면 이상적인 SERM이라고 할 수 있을 것이다(Table 1).
5,15하지만 현재까지 밝혀진 SERM 의 약리학을 기초로 판단해 본다면, 이상적인 SERM 의 조건을 모두 만족하는 하나의 제제가 개발되기는 어려울 것으로 생각된다. 이런 문제점을 극복하기 위해 개발된 것이 복합 제제이며, 현재 바제독시펜 과 결합에스트로겐(conjugated estrogen)의 합성물인
조직선택적 에스트로겐 복합체(tissue selective estrogen complex; TSEC)가 사용 중이다. TSEC은 두 약제의 장단점이 보안되어 폐경 후의 안면 홍조와 질 위축 을 호전시키고,
16,17유방과 자궁 내막을 자극하지 않 으면서 골 소실을 방지하는 것이 확인되었다.
18,19현재 사용 중인 SERM
1. 적응증
미국 식약청(FDA)의 승인을 받은 최초의 SERM은 클로미펜으로, 이 제제는 1976년 배란유도제로 허가 되었다. 1977년 미국 FDA는 타목시펜을 유방암(상 피내암) 수술 및 방사선 치료 후 침윤성 유방암의 감소 목적이나 전이성 유방암의 치료, 유방암의 보 조 치료 또는 고 위험 여성에서 유방암의 예방을 위 한 약물로 승인하였다. 그리고 20년 후인 1997년에 폐경 후 여성에서 발생된 ER 양성이나 원인 미상의 전이성 유방암의 치료로 토레미펜을, 폐경 후 여성 의 골다공증 예방과 치료, 그리고 침윤성 유방암의 예방 목적으로 랄록시펜을 미국 FDA는 승인하였다.
풀베스트랜트(fulvestrant)는 항에스트로겐 요법(anti-
estrogen therapy) 이후에도 상태가 악화된 폐경 후 여
성의 호르몬 수용체 양성 전이성 유방암의 치료로
2002년 미국에서 허가되었다. 이후 2009년에 라소폭 시펜과 바제독시펜은 폐경 후 여성의 골다공증 치료 로 유럽에서 승인되었으나 미국에서는 승인되지 못 하였는데, 이 중 라소폭시펜은 실제 시판되지는 않 았다. 2013년에 오스페미펜은 폐경으로 인한 외음질 위축으로 인한 성교통(dyspareunia)에 대한 치료로, TSEC는 폐경과 연관된 중등도에서 중증의 혈관운동 증상의 치료 및 폐경 후 골다공증 예방으로 미국에 서 승인하였다.
국내에서는 앞에서 언급된 SERM 중에서 라소폭 시펜과 오스페미펜을 제외하고 사용되고 있다.
2. 폐경 후 여성에서 SERM의 일반적 효과 현재 임상에서 사용되고 있는 대부분의 SERM은 뼈에서 에스트로겐 작용제의 역할을 하며 유방에서 는 에스트로겐 길항제나 중립적인 작용을 한다. 폐 경 후 여성에서 SERM은 골 소실로부터 뼈를 보호 하여 골밀도를 증가시키고, 궁극적으로 골절 위험을 감소시킨다. 골밀도 증가 정도는 에스트로겐이나 다 른 골흡수 억제제인 비스포스포네이트(bisphospho- nate)에 비해 SERM이 낮지만 골절 위험도의 감소 효과는 비슷한 것으로 보고되는데,
20이는 골의 미세 구조 개선과 같은 골질(bone quality)의 향상에 의한 것으로 여겨지고 있다. SERM은 혈중 총 콜레스테롤 과 LDL (low-density lipoprotein)-콜레스테롤을 감소 시키지만, 전체적으로 심혈관 질환, 전제 사망률 및 심혈관 사망률에 영향을 주지 않는다. 정맥 혈전 색 전증은 에스트로겐과 비슷하게 증가시키며, 중추 신 경계나 인지(cognition)에 미치는 영향은 다양하게 보 고되어 명확하지 않다. 그리고 SERM은 에스트로겐 길항제로 작용하여 안면 홍조를 증가시킨다.
1,5,21자궁 내막과 질에서의 효과는 SERM 제제마다 서 로 다른 차이가 있고(Fig. 5), 특히 자궁내막에 대한 안정성이 새로운 SERM 제제의 개발에 중요한 고려 사항이 되어 왔다.
22자궁내막에서 타목시펜은 에스 트로겐 작용제로, 랄시펜은 중립적으로, 바제독시펜 은 에스트로겐 길항제로 작용하며, 질에서 타목시 펜, 랄록시펜, 바제독시펜은 중립적이지만 라소폭시 펜과 오스페미펜은 에스토로겐 작용제로 작용한다.
43. Tamoxifen
타목시펜은 반감기(half-life)가 5~7일로 작용 기간 이 길며, 활성 대사물인 4-OH 타목시펜(4-hydroxy tamoxifen)이 ER에 강한 결합력을 나타내어 일정의 전구약물(prodrug)이라고 할 수 있다.
31) 유방: 타목시펜은 유방에서 에스트로겐 길항제 로 작용하여 ER 양성의 초기 유방암을 가진 여성에 서 보조 요법으로 사용되거나 전이성 유방암에 일시 적 완화를 위해 사용되었을 때 재발률과 사망률을 줄인다. 메타 분석에서 타목시펜은 유방암을 38%
감소시키고, ER 양성 유방암을 48% 감소시켰다.
2310년간 사용으로 유방암의 재발률은 3.7%로 낮았으 며 사망률을 위약 대비 2.8% 감소시켰다. 타목시펜 의 부작용으로 50세 이상에서 발생하는 자궁 내막 암, 정맥 혈전 색전증, 폐 색전증, 뇌졸증을 들 수 있 는데,
24이것으로 인한 사망률이 증가될 수 있다는 것은 주지하여야 한다.
2) 뼈: 타목시펜은 뼈에서 에스트로겐 작용제로 부분적으로 작용한다. 폐경 후 여성에서 타목시펜복 용으로 요추 골밀도는 1년에 0.61% 증가되었으나, 위약군에서는 1.0% 감소되었다. 이처럼 폐경 후 여 성에서는 골밀도가 의미 있게 증가하는 반면, 폐경 전 여성에서는 타목시펜은 반대의 소견을 보여 뼈에 부정적인 효과를 보인다.
25,263) 자궁내막: 타목시펜은 자궁 내막증(endometrial hyperplasia)과 자궁 내막암(endometrial cancer)을 증 가시킨다.
27,28자궁 내막암은 2.5배 증가되었는데, 이 중에서 50세 미만에서는 의미 있는 증가가 없었으나 50세 이상에서는 5.4배 증가시켰다. 특히 오랜 기간 사용한 경우와 비정상적으로 자궁 내막이 두꺼운 경 우에는 위험이 증가되었다.
28그러므로 50세 이상에 서 사용하는 경우 자궁 내막에 주의를 요한다.
4) 심혈관과 정맥 혈전 색전증 위험도: 혈중 지질
농도를 향상시키지만 심혈관에 대한 영향은 명확하
지 않으며, 정맥 혈전 색전증은 2~3배 증가시킨다.
295) 그 외: 안면 홍조가 50%이상에서 나타난 것으
로 보고되어 있지만 16%만이 치료가 필요하였다고
한다.
54. Toremifene
토레미펜의 효과와 안전성은 타목시펜과 비슷하 나, 부작용이 다소 낮다. 자궁 내막암이 타목시펜과 비교하여 낮게 보고되었지만 의미 있는 차이는 보이 지 않았다.
55. Raloxifene
랄록시펜은 ERα에 높은 친화력을 가지고 있으며 우리 몸에서 ERα에 대한 결합력은 estradiol의 46%이 다.
30반감기는 27시간으로 짧으며 대부분 배변으로 배설된다. 이 약물에 대한 효과는 폐경 후 여성을 대 상으로 3년과 4년간 관찰한 MORE (multiple out- comes of raloxifene evaluation) 연구
31-34와 추적 관찰을 4년 더 연장한 CORE (continuing outcomes relevant to evista) 연구,
35,36관상동맥 질환이나 관상동맥 질환의 여러 위험 인자를 가진 여성을 대상으로 한 RUTH (raloxifene use in the heart trial) 연구,
37유방암의 위험 인자를 가진 여성을 대상으로 한 STAR (study of tamoxifen and raloxifene) 연구
38등에서 보고되었다.
1) 뼈: 요추 골밀도는 3년간 랄록시펜 하루 60 mg 투여시 위약 대비 2.6% 상승하였고, 하루 120 mg은 2.7% 상승하였다.
32이러한 효과는 지속되어 7년간 투여로 두 용량의 자료를 합하여 2.2% 상승하였다.
36골흡수 표지자는 랄록시펜 하루 60 mg 3년간 투여 로 34% 감소하였고, 골형성표지자는 26% 감소하였 다. 3년째 새로운 척추 골절은 랄록시펜 하루 60 mg 으로는 30%, 하루 120 mg으로는 50% 감소하였으며, 기존 척추 골절이 없는 경우에는 55%, 기존 척추 골 절이 있는 경우에는 30% 감소하였다.
324년째 새로 운 척추 골절은 기존 척추 골절이 없는 경우에는 49%, 기존 척추 골절이 있는 경우에는 34% 감소하 여 유지되었다.
34비척추 골절에는 8년째 사용으로 뚜렷한 효과가 없었지만, 사후 분석에서 기존 골절 이 있는 여성에서는 비척추 골절이 22% 감소하였 고, 심한 척추 골절(압박률 40% 이상)이 있는 여성 에서는 비척추 골절이 36% 감소하였다.
36랄록시펜 의 골밀도 증가 효과나 골표지자 감소 효과는 비스 포스포네이트의 절반 수준이나 척추 골절 감소 효과 는 비스포스포네이트와 유사한 결과를 보였다.
202) 유방: 랄록시펜은 침윤성 유방암의 발생을 3년 째에는 76%, 4년째에는 72% 감소시켰다.
31,33침윤성 유방암의 감소는 ER 양성 유방암의 위험도 감소에 기인한 반면 ER 음성 유방암의 위험도는 유의하게 감소하지 않았다. 8년째에는 침윤성 유방암의 발생 은 59%, ER 양성 유방암은 66% 감소하였다.
35STAR 연구에서 침윤성 유방암의 예방 효과는 타목시펜과 유사하였는데, 자궁 내막암, 정맥 혈전 색전증 등의 부작용은 랄록시펜에서 적게 나타났다.
383) 자궁내막: 랄록시펜은 자궁 내막증이나 자궁 내막암의 발생을 유의하게 증가시키지 않는다. 자궁 내막의 두께는 3년째 위약군에서는 0.27 mm 감소하 였으나 랄록시펜에서는 0.01 mm 증가하였고,
318년 째 자궁 내막용종은 위약 대비 3.2% 증가되었다.
394) 심혈관계과 정맥 혈전 색전증 위험도: 랄록시 펜은 혈중 총 콜레스테롤과 LDL-콜레스테롤을 감소 시키지만 HDL-콜레스테롤과 중성 지방의 변화는 없 었다.
40MORE 연구에서 랄록시펜은 전반적으로 관 상동맥이나 뇌졸증에 영향을 주지 않았지만, 심혈관 계 질환의 위험도가 증가된 경우에는 심혈관계 위험 성을 유의하게 감소시켰다.
41하지만 이를 확인하기 위한 RUTH 연구에서 평균 5.6년간 투여시 관상동맥 질환, 뇌졸증, 전체 사망률은 유의하게 감소하지 않 아 심혈관계에 영향을 주지 않는 것으로 판단되었 다. 다만 치명적 뇌졸증은 유의하게 49% 증가하였 다.
37정맥 혈전 색전증은 3년째 위약대비 3.1배 증가 하였고,
328년째 1.7배 증가하였다.
39정맥 혈전 색전 증이 발생한 환자의 69%에서 장기간의 부동 및 혈 전 색전증의 과거력과 같은 위험 인자가 있었다.
425) 그 외: 부작용으로 안면 홍조와 다리 경련이 있 다. 안면 호조는 25%(위약군은 18%)에서 나타나지 만,
5대부분 증상은 가벼워 약물 복용을 중단할 정도 는 아니었고 자연 경과에 영향을 주지 않았다.
43안 면 홍조는 폐경 초기에 발생할 가능성이 높아 이 시 기를 지난 후에 사용하는 것을 권장한다.
6. Lasofoxifene
라소폭시펜은 생체이용률이 매우 향상된 제제로
ERα와 ERβ에 대한 결합력은 estradiol가 비슷하며,
랄록시펜과 4-OH 타목시펜과 비교하여 ERα에 대한
결합력이 10배 높다.
44,45이 약물의 효과는 폐경 후 여성을 대상으로 5년간 관찰한 PEARL (postmeno- pausal evaluation and risk-reduction with lasofoxifene) 연구에서 보고되었다.
461) 뼈: 요추 골밀도는 5년간 라소폭시펜 하루 0.25 mg 투여시 위약 대비 3.0% 상승하였고, 하루 0.5 mg 은 3.1% 상승하였다. 골흡수 표지자와 골형성 표지 자는 1년째 40~50% 감소하였다. 척추 골절은 3년간 투여 하루 0.25 mg 투여에서 31% 감소하였고 하루 0.5 mg에서는 42% 감소하였으며, 5년간 투여에도 동일한 효과가 유지되었다. 비척추 골절은 5년간 하 루 0.25 mg 투여에서는 효과는 없었지만, 하루 0.5 mg에서는 24% 감소하였다. 고관절 골절의 감소 효 과는 보이지 않았다.
462) 유방: 락소폭시펜 5년간 하루 0.5 mg 투여시 침 윤성 유방암은 85%, ER 양성 유방암은 81% 감소하 였다. 하지만 하루 0.25 mg 투여에서는 이러한 의미 있는 효과는 없었다.
463) 자궁내막: 라소폭시펜은 자궁 내막증이나 자궁 내막암을 증가시키지는 않았지만 자궁 내막이 의미 있게 두꺼워졌다(5년째 하루 0.25 mg은 1.19 mm, 0.5 mg은 1.43 mm). 그리고 자궁 내막용종과 질 출혈이 유의하게 증가되었다.
47이런 자궁 내막의 안정성 문 제로 인해 라소폭시펜은 시판되지 못하였다.
4) 심혈관계와 정맥 혈전 색전증 위험도: 락소폭 시펜은 3년간 투여시 혈중 LDL-콜레스테롤을 감소 시켰고, 중성지방은 증가시켰으며 HDL-콜레스테롤 에는 영향을 주지 않았다. 5년간 하루 0.5 mg 투여시 관상동맥 질환은 32% 감소되었으나, 하루 0.25 mg 투여시에는 유의한 효과는 없었다. 두 용량 모두 뇌 졸증 위험을 유의하게 감소시켰다. 정맥 혈전 색전 증은 하루 0.25 mg은 2.7배, 하루 0.5 mg은 2.1배 증 가하였다.
485) 그 외: 라소폭시펜은 질 위축을 호전시키고 질 pH를 감소시킨다. 안면 홍조는 증가되었다. 그리고 하루 0.25 mg은 사망률을 유의하게 증가시켰지만, 하루 0.5 mg은 이러한 효과를 보이지 않았다.
467. Bazedoxifene
바제독시펜은 ERα와 ERβ에 모두 결합하지만 ER
α에 대한 결합력이 약간 높으며 랄록시펜보다 ER α에 대한 선택력은 낮고, estradiol보다 ERα에 대한 결합력은 약 10배 낮다.
49이 약물의 효과는 폐경 후 여성을 대상으로 3년간 관찰한 연구와 이것을 2년과 4년 연장한 연구에서 보고되었다.
50,511) 뼈: 요추 골밀도는 3년간 바제독시펜 하루 20 mg 투여시 위약 대비 2.2% 상승하였고, 하루 40 mg 은 2.4% 상승하였다. 골흡수 표지자와 골형성 표지 자는 1년째 40~50% 감소하였다. 척추 골절은 3년간 하루 20 mg 투여서 42% 감소하였고 하루 40 mg에 서는 37% 감소하였으나 비척추 골절에 대한 효과는 없었다. 하지만 사후 분석에서 고위험군(대퇴경부 골밀도 -3.0 이하, 중등도나 중증의 척추 골절 1개 이상, 경증의 척추 골절 2개 이상)에서는 바제독시 펜 하루 20 mg은 비척추 골절을 위약 대비 50% 감 소시켰고, 랄록시펜 대비 44% 감소시켰다.
50바제독 시펜의 골절에 대한 자료는 FRAX (fracture risk assessment tool)에 의해 재평가 되었는데, 척추 골절, 모든 임상 골절, 비척추 골절에 대한 골절 감소 효과 는 10년 골절 위험도(10-year fracture probability)가 올라갈수록 증가하였다. 즉, 척추 골절은 10년 골절 위험도가 6.9% 이상에서, 모든 임상 골절은 16% 이 상에서, 비척추 골절은 20% 이상에서 유의하게 감 소하였다.
52바제독시펜 하루 20 mg의 척추 골절 감 소 효과는 7년(5년째 35% 감소, 7년째 30% 감소)까 지 유지되었고 전체 환자에서 비척추 골절에 대한 효과는 없었지만, 고위험군에서의 비척추 골절 감소 효과는 5년(5년째 37% 감소)까지 유지되었다.
512) 유방: 바제독시펜은 유방에 대한 자극은 없어 유 방 통 , 유 방 낭 종 , 유 방 암 을 증 가 시 키 지 않 았 다.
51,53,543) 자궁내막: 바제독시펜은 자궁 내막증, 자궁 내
막암, 자궁 내막용종을 증가시키지는 않았고, 자궁
내막의 두께를 증가시키지 않았다.
50,51,537년간의 사
용으로 자궁 내막암은 유의하게 감소하였다.
544) 심혈관과 정맥 혈전 색전증 위험도: 바제독시
펜의 혈중 지질에 대한 영향은 랄록시펜과 유사하였
으며 심혈관 질환을 일으키지 않았다. 정맥 혈전 색
전증은 랄록시펜과 비슷하게 증가되었고 주로 심부
정맥 혈전증이 증가되었다.
535) 그 외: 가장 흔한 부작용은 랄록시펜과 마찬가 지로 안면 홍조와 다리 경련이었다.
50,538. Tissue Selective Estrogen Complex (TSEC) TSEC은 바제독시펜과 결합형 에스트로겐(conju- gated estrogen)의 복합 제제로 에스트로겐의 장점인 폐경 후의 안면 홍조와 같은 혈관 운동 증상이나 질 위축으로 인한 증상은 개선하면서, 에스트로겐의 단 점인 자궁 내막과 유방에 대한 자극 효과는 바제독 시펜이 억제하여 부작용을 줄이고, 두 약물의 공통 된 장점인 뼈에 대한 효과는 유지하도록 개발되었 다. 바제독시펜 이외의 다른 SERM 제제와 에스트로 겐의 복합체는 이러한 효과를 보여 주지 못하였다.
55바제독시펜 20 mg과 결합형 에스트로겐 0.45 mg 복 합체가 폐경과 관련된 중등도 이상의 혈관 운동 증 상에 대한 치료와 골다공증 예방 목적으로 미국 FDA의 승인을 받은 유일한 TSEC으로, 국내에서도 2015년 2월부터 동일한 적응증에 사용되고 있다. 이 복합 제제의 효과는 폐경 후 여성을 대상으로 한 SMART (selective estrogens, menopause and response to therapy; SMART1~5) 연구에서 보고되었다.
16-19,56-59알려진 SMART 연구들은 3개월~2년간의 비교적 짧 은 연구 기간에 의한 결과로 장기 데이터는 좀 더 기다려 보아야 할 것이다.
1) 뼈: 다양한 용량의 바제독시펜(10 mg, 20 mg, 40 mg)과 결합형 에스트로겐(0.45 mg, 0.625 mg) 복 합체의 2년간 복용은 사용한 모든 용량에서 골 표지 자가 의미 있게 감소하고 요추부 골밀도가 증가되었 으며, 랄록시펜과의 비교에서도 대부분의 용량에서 요추부 골밀도가 더 높이 증가되었다.
57에스트로겐/
프로게스틴 복합체와의 비교에서 골밀도 증가 정도 는 다소 떨어졌다.
192) 안면 홍조와 질 위축: 바제독시펜 20 mg과 에 스트로겐 0.45 mg 또는 0.625 mg의 12주간 복용으로 안면 홍조는 75% 감소하여, 안면 홍조의 빈도와 정 도가 의미 있게 줄어들었다.
16그리고 질에서 표층 세포(superficial cell)를 증가시키고 기저 세포(basal cell)를 감소시켜 질 위축이 향상되었고, 질의 pH와 관련된 증상도 호전되었다.
173) 자궁 내막 및 유방: 바제독시펜(20 mg)과 에스
트로겐(0.45 mg, 0.625 mg)의 복합체는 자궁 내막증 이나 자궁 내막암을 유의하게 증가시키지 않았고 유 방통이나 유방 밀도도 증가시키지 않아, 자궁 내막 과 유방에 대한 부작용은 위약과 비슷하였다.
18,194) 심혈관과 정맥 혈전 색전증 위험도: 혈중 총 콜 레스테롤과 LDL-콜레스테롤을 감소시켰고, HDL-콜 레스테롤과 중성 지방을 증가시켰다.
58심혈관 질환 과 정맥 혈전 색전증은 증가되지 않았다.
605) 그 외: 근육 경련이 가장 흔한 부작용으로 보고 되었다.
589. Ospemifene
오스페미펜은 토레미펜의 대사물로 약한 에스트 로겐 작용제로 작용한다.
21) 질: 오스페미펜은 질에서는 에스트로겐 작용제 로 작용하여 표층 세포(superficial cell)와 중층 세포 (intermediate cell)의 비율을 증가시켰고 기저 세포 (basal cell)의 비율을 감소시켰다.
61,62그리고 질 건조 증과 성교통을 호전시켰고 질 pH를 감소시켰다.
632) 자궁내막: 자궁 내막에서 약한 에스토로겐 작 용제로 작용하나, 자궁 내막증이나 자궁 내막암은 발견되지 않았고 자궁 내막 두께 1 mm 이하로 증가 되었다.
643) 뼈와 유방: 오스페미펜은 골 표지자를 용량 의 존적으로 감소시켜 랄록시펜 효과와 비슷하였으나
65,66
골밀도와 골절에 대한 자료는 없다. 유방에 대해 서는 현재까지 임상 연구는 없지만 중립적인 효과를 가진 것으로 생각된다.
4) 심혈관과 정맥 혈전 색전증 위험도: 혈중 총 콜 레스테롤, LDL-콜레스테롤, HDL-콜레스테롤에 대한 영향은 없었으나 중성 지방은 증가시켰다.
67전반적 으로 심혈관 질환에는 영향이 없는 것으로 생각되지 만 장기 효과에 대해서는 관찰이 필요하다. 혈전색 전증과 관련된 뇌졸증과 심부 정맥 혈전증은 증가되 지 않았다.
685) 그 외: 가장 흔한 부작용은 두통이었고, 외음질
위축을 가진 여성의 임상 연구에서 안면 홍조는 악
화되지 않았지만 1년 연장 연구에서 안면 홍조의 빈
도는 증가되었다.
68임상 개발 중인 새로운 SERM
현재 임상 개발 중인 SERM 제제로는 유방에는 강력한 길항 작용을 보이나 자궁 내막을 자극하지 않은 것으로 알려진 acolbifene
69과 중추 신경계에 작 용하는 RAD1901
70등이 있다. 이런 제제들이 가지는 뼈에 대한 효과에 대해서는 좀 더 연구를 기다려 보 아야 할 것이다. 그리고 ER에 결합하지 않지만 ER 가 DNA에 결합하는 것을 억제시켜 SERM과 비슷한 효과를 보이는 TPBM (8-alkylthiothiated theophylline) 도 연구 중에 있다.
71요약 및 결론
SERM은 에스트로겐 수용체에 결합하여 조직에 따라 에스트로겐 작용제나 길항제로 작용하는 제제 이다. 현재 사용 중인 SERM은 대부분 뼈에서 에스 트로겐 작용제의 역할을 하며 유방에서는 에스트로 겐 길항제로 작용을 하지만 자궁이나 질에 대해서는 제제마다 서로 다른 작용을 보인다. 이런 효과로 인 해 타목시펜과 토레미펜은 유방암의 예방과 치료제 로, 랄록시펜과 바제독시펜은 골다공증의 치료제로, 오스페미펜은 질 위축으로 인한 성교통(dyspareunia) 에 대한 치료제로, TSEC는 폐경과 연관된 중등도에 서 중증의 혈관운동 증상의 치료제로 승인되었다.
라록시펜과 바제독시펜은 비스포스포네이트와 비교 하여 골밀도의 상승 효과는 떨어지지만 척추 골절 감소 효과는 비슷하며, 위장관 문제, 악골 괴사(osteo- necrosis of jaw), 비전형 대퇴 골절(atypical femoral fracture)을 일으키지 않고 장기간의 안정성(랄록시펜 8년, 바제독시펜 7년)이 보고되어 있다. 그러므로 골 다공증 치료에 있어 라록시펜과 바제독시펜은 위장 관 문제나 복용의 불편함 등으로 비스포스포네이트 를 원치 않는 여성이나 장기간 약물을 사용하여야 하는 70세 미만의 상대적으로 젊은 폐경 후 여성에 서 비교적 안전하게 사용할 수 있을 것이다.
Conflict of Interest statement:
The author (Sung-Soo Kim) has no conflict of interest related with this article.
참 고 문 헌