Introduction
Vitamin Dis an importantmicronutrient inhuman health
.
It hasamajorroleinbonemetabolism andmaybeinvolvedinthe preventionofautoimmunediseases,
certaincancers,
andCVDs.
1)Yet
,
vitaminDdeficiencyisverycommonworldwide.
We aimed to clarifythe relationship between amount of sunlight exposure and serum25(
OH)
D levelsusingThe5thKoreaNationalHealth andNutritionExaminationSurvey(
KNHANES)
data.
Sensiblesunexposureistheprimarymeansbywhichhumans
obtain Vitamin D
.
Afterexposure toUVB(
290~
315nm),
UVB photons causethe photolysis of 7-
dehydrocholesterol(
7-
DHC)
toprevitaminD3.
TheprevitaminD3formedintheskinisthen isomerized to vitamin D3(
calciol)
by a temperature-
dependent process(
37°
C).
Vitamin D3 isfurther processed in the liver to become25(
OH)
D3,
whichisthemaincirculatingmetabolite.
2)Sun exposure can produce an adequate amount of vitamin D3 in human skin
.
Exposure todirect sunlight andultraviolet B radiationfor5 to10 minutes(
depending on thetime ofday,
season,
latitude,
and skin sensitivity)
on the arms and legs한국 성인에서 햇빛 노출과 비타민 D 상태:
2010~2012년 국민건강영양조사
김동후, 이동률*, 이정운, 백래인, 김성종, 고경진
원광대학교 의과대학 산본병원 가정의학과
Sun exposure and Vitamin D status in South Korean adults: Korean National Health and Nutrition Examination Survey(KNHANES) 2010-2012
Dong-Hoo Kim, Dong-Ryul Lee*, Jung-Un Lee, Ra-In Baik, Sung-Jong Kim, Kyung-Jin Ko
Department of Family Medicine, Sanbon Medical Center, Wonkwang University College of Medicine, Gunpo
Background: Vitamin D is an important micronutrient in human health. Yet, vitamin D deficiency is very common. We aimed to clarify the relationship between amount of sunlight exposure and vitamin D status using data from the 5th Korean National Health and Nutrition Examination Survey.
Methods: From the initial KNHANES sample, 17,219 subjects aged 20 years and older were selected who had no sun exposure time value or serum 25(OH)D concentration value missing.
The adjusted mean of serum vitamin D levels and prevalence of vitamin D deficiency according to sun exposure time was calculated. Using logistic regression analysis, the odds ratio of vitamin D deficiency by subgroup was measured and P trend/P interaction was evaluated.
Results: The adjusted mean of vitamin D levels increased with age. The adjusted prevalence of vitamin D deficiency decreased and the adjusted prevalence of vitamin D insufficiency increased as the sun exposure time increased. Analysis of the odds ratio of vitamin D deficiency by subgroup showed that female gender, advancing age, residence in a rural area and occupation with less sun exposure were linearly associated with the vitamin D deficiency.
Conclusion: Sunlight exposure is the single most important factor in vitamin D status. Aging is a risk factor for vitamin D deficiency but increased outdoor activity might help to compensate. Regular sun exposure through outdoor activity is recommended especially for women, the elderly, suburban residents and persons with less occupational sun exposure.
Keywords: vitamin D, prevalence of vitamin D deficiency, sun exposure time
Received February 28, 2015 Revised July 7, 2015 Accepted September 17, 2015 Corresponding Author Dong-Ryul Lee
Tel: +82-31-390-2965 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dong-Hoo Kim, et al. Sun exposure and Vitamin D status in South Korean adults:
Korean National Health and Nutrition Examination Survey (KNHANES) 2010~2012
Korean Journal of Family Practice
KJFP
producesabout3000IUofvitaminD3
.
3)OtherdeterminantsforvitaminDstatusareskinpigmentation
,
aging,
sun protectionbehaviors and nutritional differences.
Oneprospective cohortstudyconductedintheUKshowedthat nationally recommended summer sunlight exposure amounts failtoproducesufficientvitaminDstatusinUKadultsofSouth Asian origin.
These results indicate that skin-
pigmentation differences have a profound effect on the sunlight-
exposure vitaminDresponse.
4)Advanced age is also a known risk factor for vitamin D deficiency
.
Aging decreases the capacity of human skin to produce VitaminD3.
There isan age-
dependent decrease in the epidermal concentrationsof provitaminD3.
A comparison oftheamountofprevitaminD3producedintheskininthe8-
and18-
yr-
oldsubjectswiththeamountproducedintheskinin the77-
and82-
yr-
oldsubjectsrevealedthatagingcandecrease by greater than twofold the capacity of the skin to produce previtamin D3.
5) But,
interestingly,
the elderly in countries includingKorea andThailandhadhigher 25(
OH)
D levelswhen comparedwithyoungpeople.
2)Given these multiplefactorsinfluencing vitamin D status in theSouthKoreanpopulation
,
weexamineddatafromtheKorea National Health and NutritionExamination Survey(
KNHANES V)
inordertoprovideareliablereferenceforappropriatesunlight exposuretimeandvitaminDsupplementation.
Methods
The Korea National Health and Nutrition Examination Survey
(
KNHANES)
is across-
sectional study whichhas been periodicallyconductedbytheKoreaCentersforDiseaseControl andPreventionsince1998.
KNHANES was conducted using a rolling sampling that contains a complex
,
stratified,
multistage,
probability cluster survey of a representative sample of a non-
institutionalized civilian population in South Korea.
The fifth(
2010~
2012)
KNHANESdatawasusedinthiscross-
sectionalanalysis.
Wide-
ranginginformationonhealthstatus,
healthbehavior,
nutritional condition,
andsociodemographicfactorsin576nationaldistricts inKoreawereanalyzed.
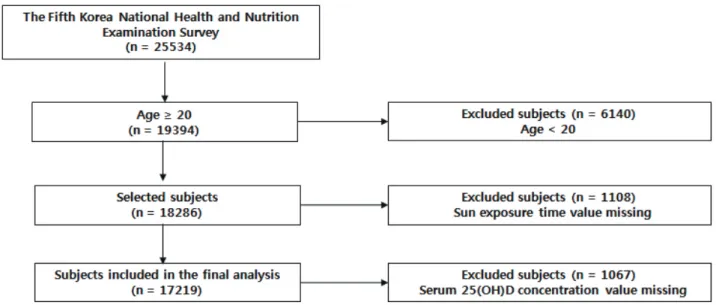
From an initial total of 25
,
534 men and women,
19,
394 subjectsaged20yearsandolderwereselected.
Ofthesesubjects,
1,
108 were excluded due to missing sun exposure time,
and an additional 1,
067 subjects due to missing serum 25(
OH)
D concentration values.
A final 17,
219 men and womenwere evaluated as showninFig.
1.
All participants providedwritten informedconsent.
Vitamin D deficiencywas defined as serum 25
(
OH)
D levels lessthan20ng/
mL,
vitaminDinsufficiencyasequaltoorgreater than20ng/
mLandlessthan30ng/
mL,
andvitaminDsufficiency as greater than 30ng/
mL.
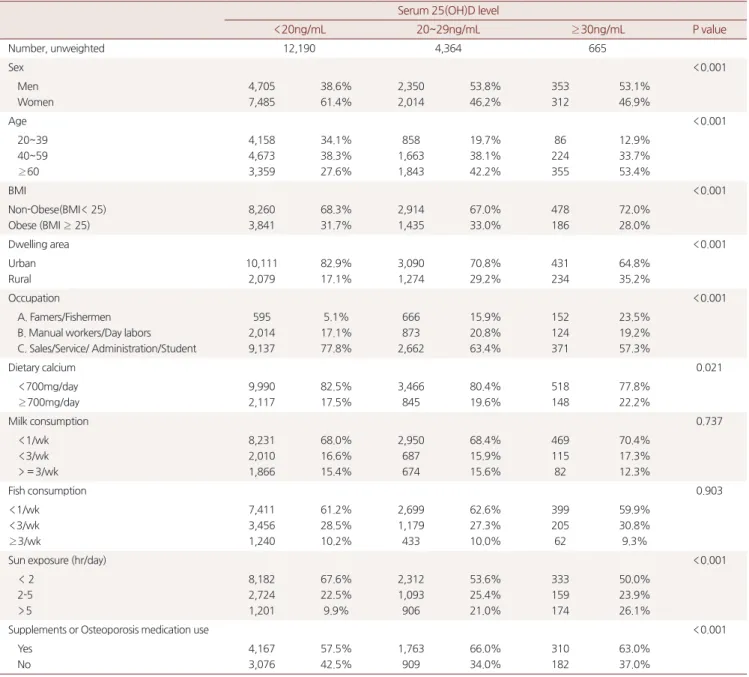
5) The demographic and clinical characteristics of the selected participants by serum25(
OH)
D levelaregiveninTable1.
Figure 1. Flow diagram for the selection of study population
ThesunexposurequestionnaireintheKNHANESisashort
-
form scoring protocolasking howmany hours the participant spent in the sunlight without wearing sunglasses ora hat per day.
Sun exposure time is divided into three groups:
those with less than 2 hours of exposureper day,
those with 2to 5 hours per day,
andthosewith morethan 5 hours per day.
Occupation wasclassified intothreecategories: (
1)
people who usually work indoors,
includingoffice workers,
professions,
managers,
salespeople andserviceindustryworkers,
housewives,
and students; (
2)
people whousually workoutdoors,
includingmanualworkersanddaylaborers
; (
3)
andfarmersandfishermen.
Dietarycalciumwascategorizedintolessthan700mgintakeper dayandequaltoormorethan700mgperday,
anamountwhich isconsideredvitalformaintaininghealthybones.
6)Adjusted prevalence ratio
(
odds ratio)
ofvitamin D deficiency by subgroup was calculated.
The test of linear trend and interactionaccordingtosunexposuretimewasperformedusing logistic regressionanalysis.
Allstatistical analyseswerebasedon two-
sidedprobabilityanda levelofsignificancesetatP<0.
05,
andwereperformedusingSASversion9.
2.
Table 1. Characteristics of subjects
Serum 25(OH)D level
<20ng/mL 20~29ng/mL ≥ 30ng/mL P value
Number, unweighted 12,190 4,364 665
Sex <0.001
Men Women
4,705 7,485
38.6%
61.4%
2,350 2,014
53.8%
46.2%
353 312
53.1%
46.9%
Age <0.001
20~39 40~59
≥ 60
4,158 4,673 3,359
34.1%
38.3%
27.6%
858 1,663 1,843
19.7%
38.1%
42.2%
86 224 355
12.9%
33.7%
53.4%
BMI <0.001
Non-Obese(BMI< 25) Obese (BMI ≥ 25)
8,260 3,841
68.3%
31.7%
2,914 1,435
67.0%
33.0%
478 186
72.0%
28.0%
Dwelling area <0.001
Urban Rural
10,111 2,079
82.9%
17.1%
3,090 1,274
70.8%
29.2%
431 234
64.8%
35.2%
Occupation <0.001
A. Famers/Fishermen B. Manual workers/Day labors C. Sales/Service/ Administration/Student
595 2,014 9,137
5.1%
17.1%
77.8%
666 873 2,662
15.9%
20.8%
63.4%
152 124 371
23.5%
19.2%
57.3%
Dietary calcium 0.021
<700mg/day
≥ 700mg/day
9,990 2,117
82.5%
17.5%
3,466 845
80.4%
19.6%
518 148
77.8%
22.2%
Milk consumption 0.737
<1/wk
<3/wk
>= 3/wk
8,231 2,010 1,866
68.0%
16.6%
15.4%
2,950 687 674
68.4%
15.9%
15.6%
469 115 82
70.4%
17.3%
12.3%
Fish consumption 0.903
<1/wk
<3/wk
≥ 3/wk
7,411 3,456 1,240
61.2%
28.5%
10.2%
2,699 1,179 433
62.6%
27.3%
10.0%
399 205 62
59.9%
30.8%
9.3%
Sun exposure (hr/day) <0.001
< 2 2-5
>5
8,182 2,724 1,201
67.6%
22.5%
9.9%
2,312 1,093 906
53.6%
25.4%
21.0%
333 159 174
50.0%
23.9%
26.1%
Supplements or Osteoporosis medication use <0.001
Yes No
4,167 3,076
57.5%
42.5%
1,763 909
66.0%
34.0%
310 182
63.0%
37.0%
Adjusted for sex, age, bmi, residence, occupation, dietary calcium, sun exposure time and supplements use
Dong-Hoo Kim, et al. Sun exposure and Vitamin D status in South Korean adults:
Korean National Health and Nutrition Examination Survey (KNHANES) 2010~2012
Korean Journal of Family Practice
KJFP
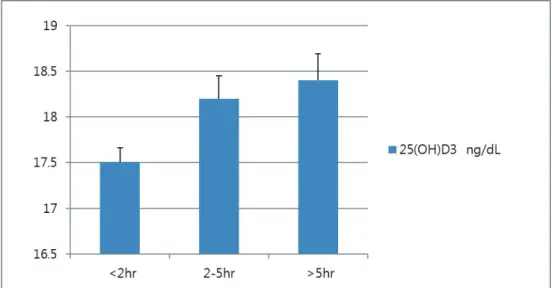
Results
Serum 25
(
OH)
D3 levelaccording to sun exposure time is giveninFig2.
ThePvalueforthegroupwithlessthan2hours ofsunexposureandthegroupwith2to5hoursofsunexposure was 0.
010.
The P value forthe group withless than 2 hours andmore than5hoursofsunexposurewas0.
009.
ThePvalue for the group withless than 2hours and more than 5 hours of sun exposure was 1.
000.
25(
OH)
D3 levels increasedwith age.
Advanced ageis awell-
known risk factor for vitaminDdeficiency
.
Apossibleexplanationforthisisthattheelderlyhave morefreetimeanddomoreoutdooractivities.
Fig 3shows theadjustedprevalence ofvitaminD deficiency
,
insufficiencyandsufficiencyaccordingtosunexposureduration.
Vitamin D deficiency prevalence was 76.
6%
in theless than 2-
hoursun exposuregroup,
69.
4%
inthe2-
to5-
hour group and 54.
1%
in the more than5-
hour group.
Theprevalence of vitamin Ddeficiency decreased assun exposuretime increased and vitaminD insufficiency increased whensun exposuretime increased.
Figure 2. Adjusted serum 25(OH)D3 level (ng/mL) by the duration of sun exposure
Adjusted for age, sex, BMI, residence, occupation, dietary calcium, sun exposure time
Figure 3. Adjusted prevalence of vitamin D deficiency and insufficiency by duration of sun exposure
Adjusted for age, sex, BMI, residence, occupation, dietary calcium, sun exposure time
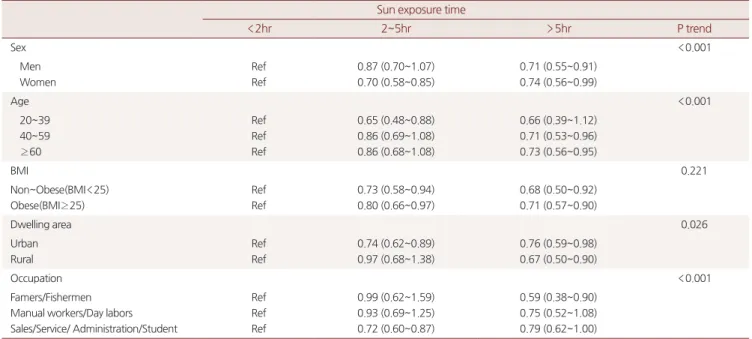
Adjustedprevalenceratio
(
oddsratio)
forvitaminDdeficiency by subgroup is givenin Table2.
Gender,
age,
residential area,
and occupation were linearly associated with prevalence of vitamin D deficiency(
P for trend=
<0.
001,
<0.
001,
0.
026,
<0
.
001,
respectively).
Discussion
Vitamin D deficiency is very common in South Korea
,
especiallyamongpeoplewithlessoutdooractivity.
Withlessthan 2hours of sun exposureper day,
76.
6%
prevalenceof vitamin D deficiencywas observed,
afactwhich is notwellrecognized among healthcare professionals or in the general population.
Aging is known to decrease the capacity of human skin to producevitaminD,
buttheolderagegroupinthisstudyshowed higher serum 25(
OH)
D levels(
vitamin D sufficiencyprevalence was 53.
4%
in the≥
60 year group,
33.
7%
in the 40~
59 year old group,
and 12.
9%
inthe 20~
39 yearold group).
Thesame trend was observed in other cross-
sectional studies usingthe fourth KNHANES data.
7)This trend might indicate that the elderly tendtoengagein moreoutdoor activitiesandlesssun-
protectionbehavior.
Thestudyresultsalsoshowedthatvariables suchasgender,
age,
residentialareaandoccupationwerelinearly associatedwith prevalenceof vitaminDdeficiency.
We assume that sunlight exposure isa more important factor than othervariables
,
andmore regular outdoor activityis recommended especiallyinwomen,
theelderly,
suburbanresidentsandpersons with lessoccupationalsun exposure.
KNHANES dataon sun-
protection behaviors(
such as using a hat or sunscreen lotion)
was not been usedin ourstudy.
Furtherinvestigation ofsun-
protection behaviors might be helpful in clarifying the linear correlationbetweensunlightexposureandvitaminDstatus.
요 약연구배경:
5차 국민건강영양조사 자료를 이용하여 일일 햇빛 노출 시간과 비타민
D상태에 대한 고찰을 하고자 하였다.
방법:
5차 국민건강영양조사 자료 중
20세 이상 성인을 우선 추출 하였다. 햇빛 노출 시간 변수와 혈중
25(
OH)
D농도 변수가 결측치 인 군을 제외하고 최종
17,
219명을 대상으로 연구를 진행했다. 비 타민
D에 대한 보정 평균을 산출하고, 햇빛 노출 시간 군에 따른 비 타민
D결핍 유병율을 구함. 로지스틱 회귀 분석을 사용하여 소집 단에 대한 비타민
D결핍의 오즈비와
ptrend수치도 산출하였다.
결과: 비타민
D의 보정평균은 나이가 증가함에 따라 같이 상승하였 다. 비타민
D결핍 유병율은 고령에서 감소하고 비타민
D부족은 고령에서 증가함이 보였다. 소집단에 대한 비타민
D결핍의 오즈비 분석에 따르면 여성, 고령, 시골 거주, 햇빛 노출이 적은 직업군으 로 갈수록 선형적인 유병률 증가가 있음을 보여주었다.
Table 2. Adjusted prevalence ratio (Odds ratio) of vitamin D deficiency (Serum 25(OH)D3<20ng/dL) by subgroup Sun exposure time
<2hr 2~5hr >5hr P trend
Sex <0.001
Men Women
Ref Ref
0.87 (0.70~1.07) 0.70 (0.58~0.85)
0.71 (0.55~0.91) 0.74 (0.56~0.99)
Age <0.001
20~39 40~59
≥ 60
Ref Ref Ref
0.65 (0.48~0.88) 0.86 (0.69~1.08) 0.86 (0.68~1.08)
0.66 (0.39~1.12) 0.71 (0.53~0.96) 0.73 (0.56~0.95)
BMI 0.221
Non~Obese(BMI<25) Obese(BMI≥ 25)
Ref Ref
0.73 (0.58~0.94) 0.80 (0.66~0.97)
0.68 (0.50~0.92) 0.71 (0.57~0.90)
Dwelling area 0.026
Urban Rural
Ref Ref
0.74 (0.62~0.89) 0.97 (0.68~1.38)
0.76 (0.59~0.98) 0.67 (0.50~0.90)
Occupation <0.001
Famers/Fishermen Manual workers/Day labors Sales/Service/ Administration/Student
Ref Ref Ref
0.99 (0.62~1.59) 0.93 (0.69~1.25) 0.72 (0.60~0.87)
0.59 (0.38~0.90) 0.75 (0.52~1.08) 0.79 (0.62~1.00) Adjusted for sex, age, bmi, residence, occupation, dietary calcium, sun exposure time, supplements use
Dong-Hoo Kim, et al. Sun exposure and Vitamin D status in South Korean adults:
Korean National Health and Nutrition Examination Survey (KNHANES) 2010~2012
Korean Journal of Family Practice
KJFP
결론: 햇빛 노출 시간은 비타민
D유지에 있어 가장 중요한 요소였 다. 노화는 비타민
D결핍의 위험요소이지만 야외활동 시간의 증 가가 위험을 보완해 줄 수 있을 것으로 보이며, 특히 여성, 노인, 시골 거주, 햇빛 노출이 적은 직업을 가진 사람에 있어서 더 추천될 수 있다.
중심단어: 비타민
D, 비타민
D결핍 유병률, 햇빛 노출
REFERENCES1. Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr 2004; 80: 1678S-88S.
2. Hataikarn Nimitphong and Michael F. Holick. Vitamin D status and sun exposure in Southeast Asia. Dermato-Endocrinology 5:1,
34–37; 2013.
3. Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357:266- 81; PMID:17634462;
4. Mark D Farrar, Richard Kift, Sarah J Felton, Jacqueline L Berry, et al. Recommended summer sunlight exposure amounts fail to produce sufficient vitamin D status in UK adults of South Asian origin. Am J Clin Nutr 2011;94:1219–24.
5. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, et al. (2005) Estimates of optimal vitamin D status. Osteoporos Int 16:
713–716.
6. E. Warensjo, L. Byberg, H. Melhus, R. Gedeborg, et al. Dietary calcium intake and risk of fracture and osteoporosis: prospective longitudinal cohort study. BMJ, 2011; 342 (may24 1): d1473 DOI:
10.1136/bmj.d1473.
7. Choi HS1, Oh HJ, Choi H, Choi WH, Kim JG, Kim KM, et al.
Vitamin D insufficiency in Korea - a greater threat to younger generation. J Clin Endocrinol Metab. 2011 Mar;96(3):643-51. doi:
10.1210/jc.2010-2133.