Vol.22 No.2 p191-198, Dec. 2005
책임저자:김용대, 705-717, 대구광역시 남구 대명5동 317-1, 영남대학교 의과대학 이비인후과학교실, Tel: (053) 620-3784, Fax: (053) 628-7884, E-mail: ydkim@med.yu.ac.kr
비부비동 반전성 유두종의 전산화 단층촬영상과 자기공명영상의 분석
배창훈․서영중․이석춘․천승민․백운회․정은채․송시연․김용대
영남대학교 의과대학 이비인후과학교실Evaluation of Computed Tomography and
Magnetic Resonance Imaging of Sinonasal Inverted Papilloma Chang Hoon Bai, Young Jung Seo, Seok Choon Lee, Seung Min Chen,
Un Hoi Baek, Eun Chae Jung, Si Youn Song, Yong Dae Kim
Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Yeungnam University, Daegu, Korea
-Abstract-
Background: Computed tomography (CT) is commonly used to evaluate the degree of sinus involvement in cases of inverted papilloma (IP). However, CT cannot differentiate tumor from adjacent inflammatory mucosa or retained secretions. By contrast, magnetic resonance imaging (MRI) has been reported to be useful in distinguishing IP from paranasal sinusitis. This study investigated whether preoperative assessment with MRI and CT accurately predict the extent of IP.
1)Materials and methods: CT and MRI were retrospectively reviewed in 9 cases of IP.
Patients were categorized into stages based on CT and MRI findings, according to the staging system proposed by Krouse. The involvement of IP in each sinus was also assessed.
Results: Differentiation of IP from inflammatory disease may be more successful in routine
cases where the inflammatory mucosa has low signal intensity on T1-weighted images and
very high signal intensity on T2-weighted images. CT imaging could not differentiate tumor
from adjacent inflammatory mucosa or retained secretions.
서 론
전통적으로 비부비동의 반전성 유두종은 내 측 상악절제술과 외측 비절개 또는 구순하 안 면중앙접근법을 이용한 완전한 일괴 절제가 추 천되었으나
1)최근에는 수술기법의 발달로 비 교적 덜 침습적인 비내시경을 이용한 절제가 선호되고 있다.
종양 절제를 위한 수술법을 결정하기 위해 서 반전성 유두종의 범위 및 위치에 따른 병기 설정의 필요성이 주장되어 최근에 TNM 병기 분류를 응용한 방법과 Krouse가 종양의 부비 동 침범 정도 및 악성화 여부에 따라 반전성 유두종의 4군으로 나눈 병기법이 제안되었 다.
2-4)Han 등
5)도 수술 접근법을 결정하기 위 해 종양을 위치와 범위에 따라 4군으로 나누는 시도를 하였다. 그러나 세계적으로 표준화되고 합의된 병기 분류법은 없는 실정이다.
비부비동의 전산화 단층촬영(CT)은 반전성 유두종에 있어서 술전 종양의 부비동 침범 범 위를 확인하고 수술법을 결정하는데 있어서 가 장 널리 쓰이는 방사선 검사법이다. 그러나 전 산화 단층촬영술은 두개저부나 안와같은 인접 한 골조직의 침범이나 미란 등은 구별해낼 수 있으나 염증성 점막과 저류된 비부비동 분비물 을 감별해낼 수 없는 단점이 있어 종종 종양의 범위를 과도하게 추측하게 하기도 한다.
이에 반해 자기공명영상(MRI)은 부비동염에 서 반전성 유두종을 구별하는데 매우 유용한
검사법이다. 최근 수년간 자기공명영상상의 강 도 차이를 이용하여 비부비강의 병변을 구별하 는 연구가 보고되고 있으며 특히 T2 강조영상 과 조영증강 T1 강조영상에서 특징적으로 격 막을 가진 층구조 (septate striated appearance or convoluted cerebriform pattern or columnar pattern appearance)를 보이므로 반전성 유두 종과 염증성 변화를 구분하는데 탁월한 것으로 보고되고 있다.
6-8, 12)이 연구의 목적은 반전성 유두종에서 술전 검사로서 전산화 단층촬영과 자기공명영상의 효용성과 정확성을 비교하고 반전성 유두종에 서 기원한 편평세포암의 수술전 진단에도 도움 이 되는지를 알아보기 위한 것이다.
재료 및 방법
2002년 8월부터 2004년 7월까지 2년 동안 영남대학병원 이비인후과 외래를 방문하여 비 내시경적 비내 수술 또는 비외 접근법을 이용 한 절제술을 통하여 비부비동의 반전성 유두종 으로 진단된 환자 중 술전 전산화 단층촬영과 자기공명영상을 동시에 시행한 9명을 대상으로 하였다. 남자 7명, 여자 2명이었고 평균 연령은 53세(39-72세)였다. 평균 외래 추적관찰 기간 은 18개월(8-30개월)이었다. 7예에서 비내시경 을 이용한 절제가 시행되었고, 1예에서는 비내 시경을 이용한 내측 상악절제술, 1예에서는 Caldwell-Luc 접근법과 비내시경을 이용한 내 Conclusion: Preoperative MRI of IP can predict the location and extent of the tumor involvement in the paranasal sinuses and sometimes predicts malignant changes.
Key Words: Computed tomography, Inverted papilloma, Magnetic resonance imaging
측 상악절제술을 동시에 시행하였다.
전산화 단층촬영은 Siemens사의 SOMATOM Plus 4를 이용하였고 자기공명영상은 Siemens 사의 MAGNETOM Vision을 이용하였다. T1 강조영상에서 repetition time(TR)은 337-735ms 였고 echo time(TE)은 11-14ms였다. T2 강조 영상에서는 TR은 3055-6000ms, TE는 100- 120ms였다. 조영증강을 위해 Gadolinium이 0.1 mM/kg의 용량으로 투여되었다.
반전성 유두종의 범위 및 악성도 유무에 따 라 Krouse가 제안한 병기 분류법을 시행하였 다. 종양이 비강 내에 국한된 경우는 T1, 사골 동에 국한되어 있거나 상악동의 내측과 상부에 국한된 경우는 T2, 상악동의 외측, 하부, 전벽 또는 후벽에 있으면서 접형동을 침범하거나 전 두동을 침범한 경우는 T3, 종양이 비부비강을 벗어나 안와나 두개를 침범하거나 악성 종양과 연관된 경우는 T4로 분류하였다(Table 1). 술
전 전산화 단층촬영과 자기공명영상의 특징적 인 소견을 조사하였다. 술전 전산화 단층촬영 및 자기공명영상에 의한 병기와 수술 소견과 병리 조직 결과에 따른 병기를 분류하여 서로 비교하였다(Table 2). 또 반전성 유두종에서 기원한 편평세포암이 동반된 경우, 전산화 단 층촬영 및 자기공명영상에서 악성화로 추측되 어지는 부분이 수술 소견과 비교하여 일치하는 지 확인하였다.
결 과
대상 환자 9명 중 7명이 반전성 유두종이였 고 2명이 반전성 유두종 및 그에 기원한 편평 세포암이였다. 편평세포암으로 진단된 2예는 각각 두개내 침범과 익상판(pterygoid plate) 침범으로 인해 AJCC (The American Joint Committee on Cancer)의 Cancer 병기상 4기 Table 1. Staging System for Inverted Papilloma by Krouse
Stage Description
T1 Tumors limited to nasal cavity
T2 Tumors limited to ethmoid sinus and/or medial and superior portions of maxillary sinus
T3 Tumors involving lateral, inferior, anterior, or posterior walls of maxillary sinus, sphenoid sinus, or frontal sinus
T4 Tumors extending outside sinonasal cavities (ie, orbital or intracranial extension) or tumors associated with malignancy
Table 2. Comparison Between CT stage, MRI stage and Postoperative stage
CT stage (n) MRI stage (n) Postoperative stage (n)
T1 (1) T1 (4) T1 (4)
T2 (1) T2 (1) T2 (1)
T3 (5) T3 (2) T3 (2)
T4 (2) T4 (2) T4 (2)
에 해당하였다. 9예 모두에서 술전 전산화 단 층촬영과 자기공명영상이 시행되었다. 술후 병 리조직 결과 및 수술 소견에 의한 Krouse 병 기 분류를 시행하였으며 각각 T1 4예, T2 1예, T3 2예, 그리고 T4는 2예였다(Table 2).
전산화 단층촬영상 병기와 술 후 병기가 일 치하는 경우는 T1에서 4예 중 1예였으며 T2, T3 및 T4로 판단한 경우는 각각 1예, 2예, 2 예로 일치하였다. 전산화 단층촬영상 병기가 T2인 경우 1예와 T3인 경우 2예는 실제 술 후 병기상 T1으로 확인되었다. T2인 경우 1예
에서는 비강내의 연부조직강도와 비슷한 상악 동 내측의 병변이 보여 T2로 진단하였으나 실 제 병리조직 결과상 염증성 병변으로 확인되어 T1으로 수정되었다. 그리고 전산화 단층촬영상 T3인 경우 2예는 각각 상악동과 접형동 내의 연부조직강도의 병변이 병리조직 결과상 염증 성 병변으로 밝혀졌다(Fig. 1).
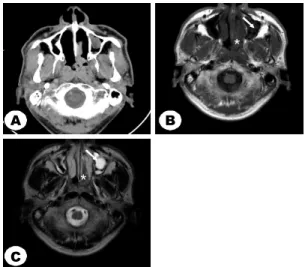
이에 반해 자기공명영상에 의한 병기는 모 든 예에서 술 후 병기와 일치하는 소견을 보였 으며, 전산화 단층촬영에서 동일하게 연부조직 강도의 병변을 보이는 경우에서도 염증성 점막 Fig. 1. A 72-year-old man with inverted papilloma (IP). Axial CT image (A) demonstrates opacification
of the right maxillary sinus. An axial T1-weighted MRI scan (B) shows IP as a hypointense signal mass and an axial T2-weighted MRI scan (C) as a intermediate signal mass involving the anterior and medial portion of the right maxillary sinus (white asterisk). Lateral portion of right maxillary sinus demonstrates low signal intensity in T2-weighted MRI scan (white arrow).
In post-gadolinium T1-weighted MRI scan (D) shows heterogeneously high signal intensity signal at the anterior and medial portion of the right maxillary sinus (black asterisk), but lateral portion of right maxillary sinus demonstrates relatively low signal intensity (black arrow). This case was judged as stage T3 by CT. But MRI and postoperative staging were identical stage T2 (Surgical biopsy of lateral portion of right maxillary sinus reported as aspergillosis, non-invasive).
C
D
B A
*
*
C
D
B A
*
C
D
B
A C C C
D D D
B B B A
A A
*
*
과 반전성 유두종으로 정확하게 구별해냈다.
반전성 유두종은 자기공명영상상 T1 및 T2
강조영상에서 저신호에서 중간신호 강도의 종 괴로 보였고 Gadolinium으로 조영증강시 정상 Fig. 2. A 48-year-old man with inverted papilloma
(IP). Axial CT image (A) demonstrates opacification of the left maxillary sinus and nasal cavity. An axial T1-weighted MRI scan (B) shows IP as a hypointense signal mass and a axial T2-weighted MRI scan (C) as a intermediate signal mass (white asterisk), whereas obstructed secretion in left maxillary sinus is indicated as high signal intensity (white arrow) in T2-weighted scan. This case was judged as stage T2 by CT. But MRI and pathologic findings showed an inflammation, and the case was judged as stage T1.
A B
C
*
*
A B
C A
A B B
C C
*
*
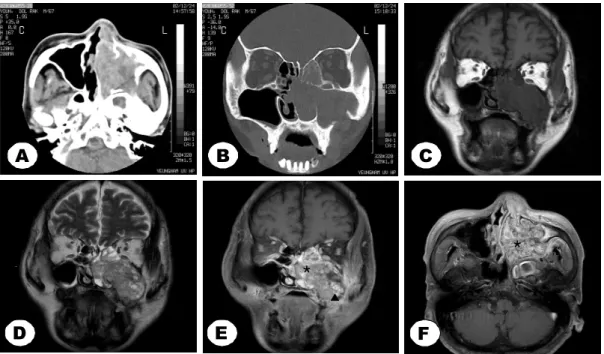
Fig. 3. A 47-year-old man with concomitant inverted papilloma (IP) and squamous cell carcinoma. An axial CT image (A) and a coronal CT image (B) demonstrate opacification of the both maxillary sinuses, nasal cavities, right orbit and brain. IP produce imaging characteristics similar to malignant lesions showing low to intermediate signal and heterogeneous pattern on T1 (C) and T2-weighting (D). In post-gadolinium T1-weighted MRI scan (E) shows low intensity signal with homogeneous enhancement at the mass in right ethmoid sinus, orbit and frontal lobe area (arrowhead), whereas IP is indicated as high signal intensity with heterogeneous enhancement (asterisk). This low signal portion suggests the diagnosis of squamous cell carcinoma.
D E
A B C
*
D E
A B C
D D
D E E E
A
A B B C C
*
비부비강 점막처럼 고신호 강도의 이질적인 증 강소견을 나타내었다. 이에 반해 염증성 점막 이나 저류된 분비물인 경우는 T1 강조영상에 서 저신호 강도, T2 강조영상에서 고신호 강도 의 소견을 보였으며 Gadolinium 조영증강시 상대적으로 저신호 강도로 관찰되었다. 전산화 단층촬영에서 실제 T1인 병변을 T2, T3로 진 단하였던 경우 T1 강조영상에서 상악동 및 접 형동 내의 병변이 저신호 강도로, T2 강조영상 에서 고신호 강도로 보였으며 조영증강 T1 강 조영상에서 조영증강되지 않는 소견을 보여 부 비동 내의 염증 또는 저류된 분비물로 생각되 었다(Fig. 2).
편평세포암으로 악성화가 된 2예에서 전산 화 단층촬영상으로는 광범위한 부비강 외 침범 및 두개저, 안와 침범 소견으로 악성화를 의심 할 수는 있었으나 연부 조직 강도 자체를 구별 해낼 수는 없었으나 자기공명영상상 1예에서 반전성 유두종의 조영증강 소견과는 다른 성질 의 종괴가 구별되어 어느 정도 악성화의 범위 를 추측할 수 있었다(Fig. 3). 그러나 다른 1예 에서는 자기공명영상상에서 반전성 유두종과 편평세포암의 범위를 구별할 수 없었다(Fig. 4).
편평세포암 2예 중 1예는 Caldwell-Luc 접 근법 및 내시경을 이용한 내측 상악절제술을 시 행하였으나 완전한 절제를 확신하지 못하였고
Fig. 4. A 69-year-old man with concomitant inverted papilloma and squamous cell carcinoma. An axial CT image (A) and a coronal CT image (B) demonstrate opacification of the left maxillary sinus, ethmoid sinus and nasal cavity. The tumor shows low signal intensity on T1-weighting (C) and intermediate signal intensity on T2-weighting (D). In post-gadolinium T1-weighted MRI scan (E, F) show intermediate intensity signal with heterogeneous enhancement in left maxillary sinus, ethmoid sinus and nasal cavity (asterisk). Lateral wall of left maxillary sinus is destructed and the mass is extruded from the sinus (arrowhead). There is no distinguishable homogeneous enhancement in the sinus.
F C
D E
B A
*
*
F C
D E
B A
FF C C
D
D E E
B B A
A
*
*
술후 추가적 처치와 방사선 치료를 계획하였으 나 치료 거부 후 외래 추적이 소실되었다. 나머 지 1예는 자기공명영상 검사 당시에 이미 안와 및 두개내 침범이 있어 항암화학요법 및 방사선 치료를 우선적으로 시행하였고 치료 효과를 확 인할 목적으로 비내시경으로 절제(debulking surgery)를 시행하였다.
고 찰
비부비동 유두종은 드문 질환으로 모든 비 부비동 종양 중 0.5-7%를 차지하며 수술로 완 전히 절제하는 것이 최선의 치료법으로 알려져 있다.
5)수술 전 검사로서 전산화 단층촬영과 자기 공명영상은 반전성 유두종의 범위와 비부비강 바깥으로의 침범을 확인하고 수술 계획 수립에 있어 널리 사용되고 있다. 특히 자기공명영상 은 골조직 침범 외에 종양과 염증성 점막 및 저류된 분비물을 감별하는데 탁월하다. 본 연 구에서 전산화 단층촬영이 부비동 내의 병변과 종양을 구별하는데 있어서 주로 T1 및 T2, T3인 비교적 낮은 병기때 구별이 쉽지 않았다.
이에 반해 자기공명영상은 T2 강조영상 및 Gadolinium 조영증강 T1 강조영상에서 염증성 점막과 반전성 유두종을 정확하게 구별하였다.
자기공명영상을 이용하여 반전성 유두종과 악성 종양을 감별하는데 있어서는 논란이 있 다. 둘 다 T1 및 T2 강조영상에서 저신호 강 도에서 중간정도 강도의 신호 강도의 소견을 보인다. Yousem 등
8)을 비롯한 많은 연구자들 이 Gadolinium으로 조영증강한 T1 강조영상 에서 반전성 유두종과 편평세포암은 비슷한 신호 강도를 보인다고 주장하였다.
9, 10)그러나
Roobottom 등
11)은 편평세포암의 경우 조영증강 T1 강조영상에서 대부분 균질적인(homogeneous) 증강 형태를 보여 이질적(heterogeneous)으로 증강되는 반전성 유두종과 차이를 보인다고 설 명하였다. Maroldi 등
12)은 반전성 유두종이 조 영증강 T1 영상에서 정상 비점막 보다 더 이 질적인 고신호 강도로, 편평세포암과 같은 악 성 종양은 저신호 강도로 나타나고 반전성 유 두종과 악성 종양의 감별점으로 위에서 언급한 조영증강 T1 영상 소견, 골파괴 정도 및 범위 의 차이, T2 및 조영증강 T1 영상에서의 특징 적인 반전성 유두종 소견(columnar pattern)이 라고 보고하였다. 본 연구의 경우에서는 반전성 유두종 및 그에 기원한 편평세포암으로 진단된 2예 중 1예는 T1 및 T2 강조영상, Gadolinium 조영증강 T1 강조영상에서 반전성 유두종과 편평세포암의 범위를 구별 할 수 없었으나 (Fig. 4), 1예에서는 하부 비강에 위치한 중간 신호 강도를 보이는 반전성 유두종과 사골동 및 안와, 두개내로 침범된 저신호 강도로 관찰 되는 종괴가 서로 다른 신호 강도를 보여 편평 세포암으로 의심이 되었고 이는 조직검사 결과 와 일치하는 소견을 보였다(Fig. 3).
요 약
확실한 자기공명영상의 효과를 판정하기 위
해서는 아직도 증례가 많이 부족한 것이 사실
이지만 본 연구의 결과에서도 알 수 있듯이 반
전성 유두종에 있어 술전 자기공명영상으로 종
양의 범위와 위치를 구별하는데 탁월한 효과를
확인하였다. 앞으로도 많은 환자를 대상으로
체계적인 연구가 이루어져야 하겠고 향후 지속
적인 자기공명영상 촬영술의 발달이 뒷받침 된
다면 좀 더 정확한 결과를 얻을 수 있을 것으 로 기대된다.
참 고 문 헌
1. Myers EN, Fernau JL, Johnson JT, Tabet JC, Barnes EL. Management of inverted papilloma.
Laryngoscope 1990 May;100(5):481-90.
2. Skolnik EM, Loewy A, Friedman JE. Inverted papilloma of the nasal cavity. Arch Otolaryngol 1966 Jul;64(1):83-9.
3. Krouse JH. Development of a staging system for inverted papilloma. Laryngoscope 2000 Jun;110(6):965-8.
4. Krouse JH. Endoscopic treatment of inverted papilloma: safety and efficacy. Am J Otolaryngol 2001 Mar-Apr;22(2):87-99.
5. Han JK, Smith TL, Loehrl T, Toohill RJ, Smith MM. An evolution in the management of sinonasal inverting papilloma. Laryngoscope 2001 Aug;111(8):1395-400.
6. Oikawa K, Furuta Y, Oridate N, Nagahashi T, Homma A, Ryu T, et al. Preoperative staging of sinonasal inverted papilloma by magnetic resonance imaging. Laryngoscope 2003 Nov;
113(11):1983-7.
7. Ojiri H, Ujita M, Tada S, Fukuda K. Potentially distinctive features of sinonasal inverted papilloma on MR imaging. Am J of Roentgenol 2000 Aug;175(2):465-8.
8. Yousem DM, Fellows DW, Kennedy DW, Bolger WE, Kashima H, Zinreich SJ. Inverted papilloma: evaluation with MR imaging. Radiology 1992 Nov;185(2):501-5.
9. Som PM, Shapiro MD, Biller HF, Sasaki C, Lawson W. Sinonasal tumors and inflammatory tissues: differentiation with MR imaging.
Radiology 1988 Jun;167(3):803-8.
10. Lanzieri CF, Shah M, Krauss D, Lavertu P.
Use of gadolinium-enhanced MR imaging for differentiating mucoceles from neoplasms in the paranasal sinuses. Radiology 1991 Feb;178 (2):425-8.
11. Roobottom CA, Jewell FM, Kabala J. Primary and recurrent inverting papilloma: appearances with magnetic resonance imaging. Clin Radiol 1995 Jul;50(7):472-5.
12. Maroldi R, Farina D, Palvarini L, Lombardi D, Tomenzoli D, Nicolai P. Magnetic resonance imaging findings of inverted papilloma:
differential diagnosis with malignant sinonasal tumors. Am J Rhinol 2004 Sep-Oct;18(5):
305-10.