Cobb’s Syndrome에 의한 고심박출성 심부전의 색전술을 이용한 치료 1예
6
0
0
전체 글
(2) 주 소:노작성 호흡곤란과 하지부종.. 원 하였다.. 현병력:7년 전 척수 동정맥 기형으로 신경외과에서. 이학적 소견:입원당시 혈압은 110/70 mmHg, 맥박. 6번 경추의 완전 추궁 절제술, 5번과 7번 흉추의 부분. 은 분당 80회, 호흡수 분당 20회, 체온은 36.5℃였다.. 추궁 절제술과 혈관종 부분 제거술을 시행 받고 특별한. 외안상 만성 병색소견 보였고, 경정맥 확장은 관찰되지. 증상 없이 지내다, 내원 1년 전부터 간헐적인 하지부종. 않았다. 흉부 청진상 심박동은 규칙적이었으나 좌측 흉. 있었고 내원 1개월 전부터 노작성 호흡 곤란 있어 내. 골연에서 3도의 수축기 심잡음이 들렸고, 좌하폐야의. A. B. Fig. 1. There are asymptomatic, diffuse, confluent, some irregularly elevated, bright or dark purplish patches and plaques on the trunk.. A. B. Fig. 2. Initial chest PA shows marked cardiomegaly, dilated pulmonary artery and azygous vein, parahilar and peribronchial infiltration and small amount of left pleural effusion (A). Chest PA after fourth embolization shows decreased heart size and disappeared left pleural effusion (B).. 1106. Korean Circulation J 2002; 32(12): 1105-1110.
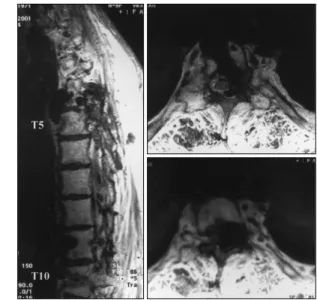
(3) 호흡음의 감소가 있었다. 복부 검사는 특이 소견 없었으. 심초음파 검사 소견:좌심실 구혈율은 60%로 정상. 나 좌측 흉부와 옆구리와 등까지 연결되는 불규칙한 표. 수축기능을 보였으며, 좌심실 및 우심실의 확장과 함께. 면을 지닌 보라색의 미만성 반이 관찰되었고 압통이나. 중등도의 삼첨판 폐쇄부전의 역류 jet의 속도로 계산한. 열감은 없었다(Fig. 1). 하지에 경미한 함요 부종이 관. 수축기 폐동맥압은 65~70 mmHg로서 중등도의 폐동. 찰되었다. 혈액 검사소견:말초 혈액 검사 상 백혈구 4800/μL, 혈색소 11.0 g/dL, 혈소판 165000/μL 이었고, 혈청 전해질과 생화학 검사상 BUN/Creatinine 13.9/0.71 mg/dL, total protein/albumin 6.95/3.77 g/dL, AST/ ALT 25/13 IU/L, LDH/CPK 454/81 IU/L, CK-MB 1.0 IU/L, sodium/potassium 140/4.1 mEq/L, Total cholesterol/Triglyceride 95/45 mg/dL, HDL-cholesterol 33 mg/dL 이었고, 동맥혈 가스 분석 소견은 pH 7.345, pCO2 43.8 mmHg, pO2 65.7 mmHg, SaO2 91% 이었다. 단순 흉부 X선 촬영:심비대, 양폐문 주위와 기관 지 주위의 침윤 소견 및 좌측 늑골횡격각의 둔화 소견 보여, 심부전에 의한 간질성 폐부종 및 좌측 흉수가 있 음을 시사하였다(Fig. 2). 심전도:분당 114회의 빠른 동율동 외에 특이 소견 은 없었다.. Fig. 4. MRI of thoracic spine shows multiple signal void mass in posterior paraspinal, anterior dural and prevertebral area involving T5, T6 and T10. T5, T6 are filled with granulation tissue after total laminectomy.. Fig. 3. Transthoracic echocardiography shows diastolic LV collapse, dilated RA and RV, moderate TR, dilated IVC suggesting volume overload status of RA and RV. LV;left ventricle, RV;right ventricle, LA;left atrium, RA;right atrium, TR;tricuspid regurgitation, IVC;inferior vena cava, PG;pressure gradient.. 1107.
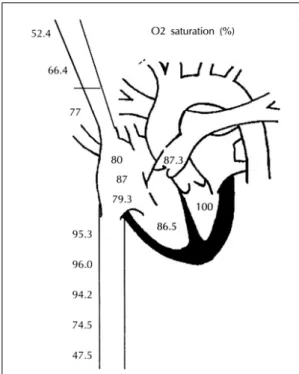
(4) 맥 고혈압 소견을 보였으나 심장내 단락은 관찰되지 않. L/min, 심지수 9 L/min/m2, Fick’ s method로 측정한. 았다(Fig. 3).. 폐관류량 10.2 L/min, 유효 혈류량 2.3 L/min로 단락. 흉부 자기 공명 영상:(Fig. 4).. 량 7.9 L/min로서 77%의 단락비 소견 보였으며 폐 동. 심도자술 소견:심도자술 시행 결과 관상동맥은 정상. 맥압은 65 mmHg였다. 하대정맥의 원위부 부터 우심방. 이었고, thermodilution method로 측정한 심박출량 14. 방향으로 차례로 시행한 산소 포화도는 각각 47.5%, 74.5%, 94.2%, 96.0%, 95.3%로 요추 동정맥 부위에 서 가장 심한 좌우 단락을 보였고, 상대정맥은 쇄골하 정 맥부터 우심방 방향으로 각각 52.4%, 66.4%, 77.5% 소견 보여 단락이 있음을 알 수 있었다(Fig. 5). 치료 및 경과:심도자술 및 심초음파 검사상 심외 단 락의 원인이 동정맥 기형일 것으로 예측되어 확인을 위 해 흉부 대동맥에 대한 혈관 조영술을 시행하였다. 시 행 결과 우측 기관지 동맥, 우측 3, 4 번째 요추 동맥과 8, 9 번째 늑간 동맥, 좌측 6, 8, 9, 11, 12 번째 늑간 동 맥과 1, 2, 3 번째 요추 동맥에서 기인하는 척수 동정맥 기형 소견 보여 코일과 색전제(Contour emboli)를 이 용하여 각각 두차례에 걸쳐 색전술을 시행하였다(Fig. 6). 두차례의 색전술후 시행한 심초음파상 심박출량 9.3 L/min로 호전된 소견이나 아직 단락 소견 남아 있어 세 번째 혈관 조영술을 시행하여 우측 3, 4번째 요추 동맥 에 대해 코일과 색전제(Contour emboli)로 색전술을 시행하였다. 2개월 후 환자의 증상은 호전 된 상태에서 네번째 혈. Fig. 5. Cardiac catheterization before embolization.. A. 관 조영술을 시행하였고, 우측 3,4번째 요추 동맥에서. B. Fig. 6. In initial angiography, there is noted spinal arteriovenous malformation fed by right bronchial artery (A). After embolization of this vessel using coils, there is noted well-occluded feeder (B).. 1108. Korean Circulation J 2002; 32(12): 1105-1110.
(5) 기인하는 동정맥 기형 남아 있어 역시 코일과 색전제. 의한 심부전의 진행은 단락의 양과 기본적 심기능에 의. (Contour emboli)를 이용하여 색전술을 시행하였다.. 해 좌우된다.9). 환자는 색전술 시행 후 양 하지의 감각저하와 통증. 치료를 해야 하는 경우는 신경학적 증상이 있거나 출. 등 일시적 증상 악화가 있었으나 곧 회복되었고, 노작. 혈, 심부전, 통증, 피부괴사, 미관손상 등이 있는 경우. 성 호흡곤란 증세는 호전되었다. 이때 시행한 심초음파. 이고, 대개 동정맥 기형 색전술과 수술적 치료를 병행. 결과 심박출량은 7.8 L/min로 감소하였고(Fig. 3), 입. 해야 하는 경우가 많다.7)10). 원시와 비교한 흉부 단순 촬영에서 심장의 크기 감소와. 최근의 척수 동정맥 기형의 치료는 본 환자의 경우처. 좌흉수와 폐부종이 사라진 호전 소견 보였으나(Fig. 2). 럼색전술이 우선적으로 선택되어 지고, PVA(polyvinyl. 아직도 심비대 소견이 있는 상태로 추가적인 색전술을. alcohol), microfibrillar collagen, coils, detachable. 시행할 예정에 있다.. balloons, NBCA(N-butylcyanoacrylate) 등이 색전 제로 이용된다.2)7)9)11) 여러 보고에 의하면 이러한 색. 고. 찰. 전 치료로 60~90% 가량 호전을 보이나 혈관의 재관 류에 의한 재발이 많아 재색전술이나 수술적 치료가 필. 고심박출성 심부전은 말초 조직의 산소 요구량을 충 족시키기 위해 심박출량이 증가해야 하는 상태로, 빈혈,. 요한 경우가 있었고,12-14) 치료효과가 없거나 합병증으 로 인한 악화도 드물지 않게 보고 되고 있다.15). 갑상선 기능 항진증, 베리베리 심장병, 동정맥류 및 동. 치료 후 경과 판정은 임상적 호전 및 심도자에 의한. 정맥 기형, 골 파제씨병, 섬유 이형성증, 진성 적혈구 증. 심박출량의 측정이 가장 유용하며, James F. Trotter. 다증, 다발성 골수종, 임신, 사구체 신염 등의 신질환, 칼. 등16)의 보고에 의하면 색전술시 심도자를 병행하여 심. 시노이드 증후군, 비만등이 그 원인으로 알려져 있다.1). 박출량의 측정으로 치료 종결을 결정할 수 있었다 하나,. 이러한 질환들 중 동정맥 기형에 의한 경우는 매우. 본 환자의 경우 치료효과는 심초음파를 통한 심박출량. 2). 드물게 보고되어 있고, 그 중 피부뇌막척수 다발성 혈. 의 감소로 판정하였고, 비침습적이며 임상적 편리성을. 관종(cutaneomeningospinal angiomatosis) 이라고 불. 볼 때 더 유용한 것으로 보여 진다.. 리는 Cobb’ s syndrome 은 현재까지 우리 나라 문헌. 또한 4차례의 색전술 후에도 심박출량이 높고 심부. 에서는 단 2예만이 보고 되었고, 그에 의한 고심박출. 전 증상이 남아 있어 추가적인 색전술이 필요할 것으로. 성 심부전의 발생과 그 치료에 대해서는 본 보고가 처음. 사료된다.. 3)4). 이다.. Cobb’ s syndrome 이란 척수 동정맥 기형이 있으면. 중심 단어:우려성 심부전;색전술;동정맥 기형.. 서 동일한 피부 분절에 피부병변이 있는 질환으로, 태. REFERENCES. 아시기에 혈관 구조의 발생 장애로 인해 태아의 모세혈. 1) Anand IS, Florea VG. High output cardiac failure. Curr. 관망과 비슷한 구조가 남아 있기 때문이며,3) 대개 유아 기나 청소년기에 발병한다. 피부 병변으로 혈관각화종. Treat Options Cardiovasc Med 2001;3:151-9. 2) Israel PG, Armstrong BE, Effman EL, Newman GE, An-. (angiokeratoma), 모반(angiolipoma), 해면상 혈관종 (carvenoushemangioma), 혈관지방종(arteriovenous malformation), 동정맥 기형(arteriovenous malformation) 등이 나타날 수 있다.3-7) 이 질환의 초기증상은 대개 척수 병변이나 뇌출혈 등 에 의한 신경학적 이상으로 나타나고 본 예처럼 심부전. 3) 4). 5). 8). 증상으로 처음 진단되는 경우는 드물다.. 또한 동정맥 기형은 기형이 다발성으로 오고 흔히 좁 은 분지를 통과하므로 저항이 유지되어 대개 혈역학적 변화가 경미하거나 없는 경우가 많으나, 이러한 병변에. 6). derson PA. Retroperitoneal arteriovenous malformation, a rare cause of heart failure in infancy: consideration of therapeutic approaches. Pediatr Cardiol 1993;14:49-52. Jong KY, Sung WK, Seung CP, Chung WK, Ji HY. A case of Cobb syndrome. Ann Dermatol 1997;9:64-8. Shim JH, Lee DW, Cho BK. A case of Cobb syndrome associated with lymphangioma circumscriptum. Dermatology 1996;193:45-7. Brant AJ, James HE, Tung H. Cutaneomeningospinal angiomatosis (Cobb syndrome) with tethered cord. Pediatr Neurosurg 1999;30:93-5. Miyatake S, Kikuchi H, Koide T, Yamagata S, Nagata I, Minami S, Asato R. Cobb’s syndrome and its treatment with embolization: case report. J Neurosurg 1990;72: 497-9.. 1109.
(6) 7) Halbach VV, Higashida RT, Dowd CF, Fraser KW,. 8). 9). 10). 11). Edwards MS, Barnwell SL. Treatment of giant intradural (perimedullary) arteriovenous fistulas. Neurosurgery 1993; 33:972-80. Graziani N, Bouillot P, Figarella-Branger D, Dufour H, Peragut JC, Grisoli F. Cavernous angiomas and arteriovenous malformations of the spinal epidural space: report of 11 cases. Neurosurgery 1994;35:856-64. Cho JH, Koh YB, Lee YK. Radical surgery for congenital arteriovenous malformation. J Korean Surg Soc 1983;25: 827-33. Kuga T, Esato K, Zempo N, Fujioka K, Harada M, Furutani A, Akiyama N, Toyota S, Fujita Y. Successful management of a giant spinal arteriovenous malformation with multiple communications between primitive arterial and venous structures by embolization: report of a case. Surg Today 1996;26:756-9. Niimi Y, Berenstein A, Setton A, Neophytides A. Embolization of spinal dural arteriovenous fistulae: results and. 1110. follow-up. Neurosurgery 1997;40:675-83. 12) Lee TT, Gromelski EB, Bowen BC, Green BA. Diagno-. 13). 14). 15). 16). stic and surgical management of spinal dural arteriovenous fistulas. Neurosurgery 1998;43:242-7. Glasser R, Masson R, Mickle JP, Peters KR. Embolization of a dural arteriovenous fistula of the ventral cervical spinal canal in a nine-year-old boy. Neurosurgery 1993;33: 1089-94. Kim DY, Kim SJ, Chung JW, Park JH. Embolization followed by surgical resection for congenital arteriovenous malformation. J Korean Vasc Surg 1994;10:141-6. Mourier KL, Gobin YP, George B, Lot G, Merland JJ. Intradural perimedullary arteriovenous fistulae: results of surgical and endovascular treatment in a series of 35 cases. Neurosurgery 1993;32:885-91. Trotter JE, Suhocki PV, Lina JR, Martin LW, Parrish JL, Swantkowski T. Hereditary hemorrhagic telangiectasia causing high output cardiac failure: treatment with transcatheter emboli-zation. Am J Gatroenterol 1998;93:1569-71.. Korean Circulation J 2002; 32(12): 1105-1110.
(7)
수치

관련 문서
