78
서 론
간내담관 결석증의 외과적 치료 방법에는 담즙배액술과 간절제술이 있으며 담관 협착부위를 제거하고 잔류 결석의 재발을 최소한으로 하기 위한 간내담관 결석증의 치료 목 적에 부합되는 것은 간절제술이다.1,2 간의 해부 및 영상 기 술의 발달과 수술 술기의 발전으로 안정적인 간절제술이 보편화되고 간내담관 결석의 원인으로 알려진 담관 협착 부위의 완전한 제거가 가능하게 되었지만 수술 후 담즙 누 출이나 잔류 결석 재발 등의 합병증을 자주 경험하게 된다.
최근 일본 연구자의 보고에서 폐쇄성 황달을 가진 72명 의 환자를 대상으로 computed tomography (CT) 담관조영술 을 이용하여 좌내측구역 담관 구조에 관한 영상 분석 결과, 의미 있는 다양한 형태의 해부 구조를 알게 되었다.3 즉 좌 내측구역 담관(B4)이 좌간 주담관으로 배액 되는 경우가 35%, 좌외측구역 후분절(B2)과 좌외측구역 전분절(B3)의 합류부로 배액되는 경우가 25%, 좌외측구역 전분절(B3)로 배액되는 경우가 20%였으며 좌우 간관 합류부로 배액되는
Feasibility of Left Hemi-hepatectomy for the Treat-
ment of Left Intrahepatic Duct Stones
Yong Hoon Kim, M.D., Koo Jeong Kang, M.D. and Tae Jin Lim, M.D.
Department of Surgery, Keimyung University School of Medicine, Daegu, Korea
Purpose: The definite modality for the treatment of intrahe-
patic duct stones (IHS) is a hepatic resection, which can achieve two goals; removal of the stones and stricture of the bile duct, thus reducing the risk of recurrent intrahepatic duct stones. As a procedure, a left lateral sectionectomy has usually been applied, according to the disease location.However, in patients having had a left lateral sectionectomy, the postoperative results have shown increased complication rates. In this study, we investigated the better results of a left hemi-hepatectomy compared to a left lateral sectionec- tomy for the treatment of left IHS in terms of postoperative complications.
Methods: Thirty two patients, who were treated with a
hepatic resection for their IHS, between January 2001 and November 2003, were analyzed. The patients were divided into two groups according to the operative procedure, as follows; group I had a left lateral sectionectomy and group II a left hemi-hepatectomy. The amount of bleeding, duration of surgery, postoperative results and complications were com- pared between the two groups.Results: There were 22 and 10 females and males, re-
spectively, with a mean age of 56.9 (±10.0) years. Of the patients, 14 and 18 were placed into groups I and II, respec- tively. The duration of surgery in groups I and II were 220.0 (±41.6) and 255.0 (±49.8) minutes, respectively. The vol- ume of bleeding was 294.6 (±345.5) and 406.0 (±177.0)좌측 간내담관 결석에 대한 수술로써 좌간절제수술의 타당성
계명대학교 의과대학 외과학교실 김 용 훈․강 구 정․임 태 진
ml in groups I and II, respectively (p>0.05). The incidence of complications (bile leakage, abscess and occurrence of inflammatory pseudotumors) after a left hemihepatectomy were significantly lower than those after a left lateral sec- tionectomy (p<0.05).
Conclusion: This study revealed that a left lateral sectionec-
tomy has greater complications compared to a left hemihepa- tectomy for the treatment of left IHS. This may be caused by anatomic variations in bile duct drainage from the left medial segment. If the anatomy of the medial segmental duct was not identified preoperatively, a standard left hemi-hepa- tectomy should be considered. (Korean J HBP Surg 2005;9:78-83)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Bile ducts, Intrahepatic
Cholelithiasis Hepatectomy Complication
중심 단어: 간내담관 결석증, 좌간절제술, 수술합병증
책임저자:강구정, 대구광역시 중구 동산동 194 ꂕ 700-712, 계명대학교 의과대학 외과학교실 Tel: 053-250-7655, Fax: 053-250-7322 E-mail: kjkang@dsmc.or.kr
본 논문의 요지는 2003년 한국간담췌외과학회 추계학술대회에서 발표되었음.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
경우가 6%였다. 이것을 모식화해 보면 Fig. 1과 같다.
간내 담석증은 좌측 간관이 우측 간관보다 예각이므로 담즙의 흐름에 장애가 있을 수 있어서 좌측 간관에 발생빈 도가 높으며 그 중에서도 좌외측구역에 국한된 경우가 많 기 때문에 간절제수술로는 좌외측구역 절제술이 79%로 대 다수를 차지해 왔다.4-6 간내 담석증에 대한 외과적 절제 후 추적 관찰에 관한 국내 보고는 있으나,7,8 좌측간에 국한된 간내 결석증의 간 절제후 수술 방법에 따른 장기 추적 결과 에 대한 국내 보고는 찾아볼 수 없었다.
저자들은 간내담관 결석에 관한 수술로 간내 담석의 위 치나 협착 위치에 관계없이 무작위로 좌간절제수술과 좌외 측구역 절제수술을 당시의 상황에 따라 시행하였다. 수술 후 담즙 누출이나 간내 농양의 재발 및 절단면 주위에 염증 성 가성종양 등의 합병증 발병 빈도는 간 좌외측구역 절제 수술(left lateral sectionectomy) 후 더 빈번히 발생하게 됨을 경험적으로 알게 되었다. 이런 경험과 최근 보고된 Cho 등3 의 보고를 바탕으로 좌외측구역 절제수술 후에 좌내측구역 담관의 손상 빈도가 높을 수 있다는 것을 알게 되었다. 최근 간내 담석증으로 진단되면 수술 전 자기공명 담췌관 조영
술(magnetic resonance cholangiopancreatography: MRCP)을 통하여 간내담관의 해부구조를 파악하고 수술 범위를 정하 기도 하지만 세밀하게 조영되지 않는 경우도 있다. Fig. 1의 모식도에서 볼 수 있듯이 좌내측구역 담관(B4)의 좌측 담관 과의 합류지점에 관한 정보가 없는 상태에서 좌외측구역 절제수술을 하게 되면 모식도에서 b 혹은 c 형태의 담관해 부구조를 가진 경우 좌내측구역 담관지의 손상이 따를 수 있다. 이 연구결과를 토대로 자기공명 담췌관 조영술이나 수술 중 담관조영술에 의한 간내담관의 해부구조를 모르는 상태에서 간 좌외측구역 절제수술을 시행한다면 최고 45%
까지 담관 손상이 있을 수 있다.
이러한 사실을 근거로 저자들은 최근 3년간 시행한 간내 담석증에 대한 좌간 혹은 좌외측구역 절제 수술한 환자들 을 두 군으로 나누어 수술 후 담관 손상과 관련된 합병증의 빈도를 좌외측구역 절제수술과 좌간절제수술 결과를 합병 증 발생빈도를 중심으로 후향적으로 분석하여 적절한 수술 방법을 알아보고자 했다.
Fig. 1. A schematic diagrams of various intrahepatic biliary drainage of the left medial segmental duct (B4) of the liver (adopted from reference 3, Hepatogastroenterlogy 2003;50:1073-1077). This figure shows 45% of medial segmental duct (b+c) may be injured by left lateral sectionectomy.
7
7
7
7 8
8
8
8 2
2
2
2 3
3
3
3 4a
4a
4a
4a 4b
4b
4b
4b 5
5
5
5 6
6
6
6 35%
20%
25%
6%
a
c
b
d
방 법
2001년 1월부터 2003년 11월까지 계명대학교 의과대학 외 과학교실에서 좌측 간내담관 결석증으로 진단되고 간절제 수술을 시행한 32명의 환자를 대상으로 하여 좌외측구역 절제술(left lateral sectionectomy)을 시행한 군을 I 군, 좌간절 제술(left hemihepatectomy)을 시행한 군을 II 군으로 나누었 고 이들의 연령, 성별 분포, 수술 방법, 수술 결과, 수술 합병 증 및 임상경과 등을 후향적으로 비교 분석하였다. 수술은 한 명의 술자에 의해 이루어졌으며 간실질의 절제는 초음 파 분쇄 흡인기(CUSA, Cavitron Ultrasonic Surgical As- pirator, Valley lab, Colorado, USA)와 전기소작기를 적절히
사용하였으며 간절제 동안 중심정맥압 하강 기법과 간헐적 혈류 차단법(프링글 기법, Pringle maneuver)을 이용하였다.
두 군 간의 수술 결과 즉 수술 시간과 출혈량을 비교하였고 담즙 누출과 농양의 발생, 그리고 염증성 가성 종양(inflam- matory pseudotumor) 등 합병증 발생 정도를 비교 분석하였 다.
통계 처리는 SPSS 11.0 for Windows (Chicago, IL)을 사용 하였고 평균값의 비교는 t 검증(independent sample t-test), 수 술 후 합병증의 빈도는 Fisher's Exact test를 이용하였다.
결 과
전체 환자 32명 중 남자는 10명(31.2%), 여자는 22명(68.8%)
Fig. 3. (a, b) A 46-year-old womam: magnetic resonance (MR) imaging scans taken 8 months after the left lateral sectionectomy show left intrahepatic duct stones and intrahepatic abscess formation in B4.
a b
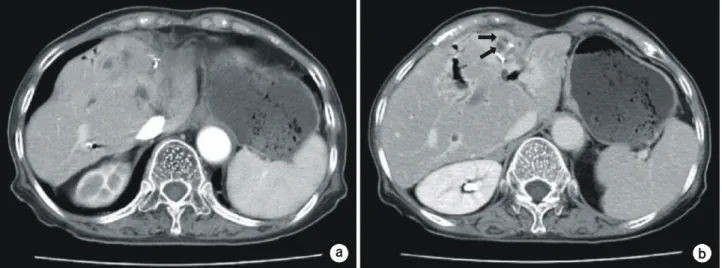
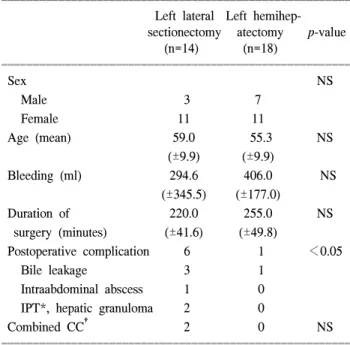
Fig. 2. (a, b) A 63-year-old woman: computed tomography (CT) scans taken 6 months after left lateral sectionectomy show inflammatory pseudotumor in S4, and adjacent S1 and S8 and cholangitis in B4.
a b
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 이었고 평균 연령은 56.9 (±10.0)세였다. 좌외측구역 절제
술 14명(43.8%), 좌간절제술을 18명(56.3%)에서 시행했다.
평균 출혈량은 415 ml (±312.1), 평균 수술 시간은 241.8분 (±49.4)이었다. 합병증은 7예(21.9%)에서 발생했었고, 담즙 누출 혹은 복강 내 농양이 5예, 육아종 혹은 염증성 가성종 양이 2예(6.3%)에서 있었다(Fig. 2, 3). 수술과 관련된 사망 예는 없었다. 경과 관찰 중에 절제연에 담관암이 발생한 경 우가 2예 있었다. 예후 추적 중 사망은 2예(6.3%)에서 발생 했고 담관암에 의한 경우가 1예, 심근경색증에 의한 경우가 1예 있었다.
좌외측구역 절제술 환자군은 남자 3명, 여자 11명이었고 평균 연령은 59.0 (±9.9)세였으며 수술 중 출혈은 294.6 (±
345.5) ml 수술 시간은 220.0 (±41.6)분이었다. 좌간절제술 환자군은 남자 7명, 여자 11명, 평균 연령은 55.3 (±9.9)세 였으며 수술 중 출혈은 406.0 (±177.0) ml 수술시간은 255.0 (±49.8)분이었다.
수술 시간과 출혈량에서 통계적으로 유의한 차이는 없었 다. 수술 후 발생한 담즙 누출 및 복강 내 농양의 발생률은 좌외측구역 절제술 후 4예(28.6%), 좌간절제술 후 1예(5.6%) 있었으며 추적 기간 동안 확인된 염증성 가성종양 및 육아 종은 2예 모두 좌외측구역 절제술 후 발생하여 합병증 빈도 는 좌외측구역 절제술 군에서 통계적으로 유의하게 높았다 (p<0.05)(Table 1).
고 찰
최근의 간해부에 관한 지식을 바탕으로 간염이나 간경화 증을 동반하지 않는 간내 결석증 환자에 있어서 좌간절제 수술 환자를 중심으로 좌간절제수술 혹은 좌외측구역 절제 수술을 시행 후 추적검사에서 수술 방법에 따른 합병증을 중심으로 연구하였다.
간내담관 결석증은 좌, 우 간내담관 합류부의 근위부에 위치하는 것을 일컬으며9 주로 좌측 간내담관에 발생하고10 이것은 좌측 간관이 우측 간관보다 예각이므로 담즙의 흐 름에 장애가 있을 수 있어서 좌측 간관에 발생빈도가 높은 것으로 알려져 있다.11
간내담관 결석의 치료법으로 담도경에 의한 결석제거 (cholangioscopic lithotripsy), 담도협착 부위에 경피적, 중재 적 시술에 의한 확장 및 금속 스텐트 삽입술은 비수술적 방법으로 간내 결석의 제거율 또한 수술적 방법에 비하여 못하지 않다.6,12,13 그러나 간내담관 결석 환자의 42∼96%에 서 담관 협착이 보고되었고 이러한 협착부위의 완전한 제 거없이 일시적인 결석의 제거나 협착부위의 확장은 간내 결석의 치료 후 재발의 가장 많은 원인이 되고 있다.12 간내 담관 결석의 치료 원칙은 간내외 담관 결석의 완전한 제거 와 협착이 있는 담관의 절제 및 이환된 담관 분지와 장관 문합에 의한 담즙의 원활한 배액이다.14 1985년 이전까지만
해도 간내담관 결석의 외과적 치료방법으로 술식의 편이성 때문에 간절제 대신 담관-공장 문합술 등의 담즙배액술이 많이 시행되었다. 그러나 수술 후에 잔류 담석의 발생률이 많게는 56%까지 보고되어서6 담즙배액술 단독으로 간내담 관 결석증을 치료하는 것은 적절치 않다.
자기공명영상촬영 및 다중 채널 전산화 단층촬영 등의 정확한 영상기법의 발전과 더불어 간절제 수기의 발달로 간내담관 결석의 수술적 치료로 간절제가 표준화된 술식으 로 자리 잡게 되었고5 수술 후 잔류 담석 발생률 또한 4.5∼
9.5%로 담즙배액술보다 나은 결과를 보고하였다.15,16 간내담 관 결석의 치료로 간절제술을 해야만 하는 또 다른 이유는 담관암의 발생 가능성이 약 10% 가량으로 어떤 질병보다 높다는 것이다.17,18 담관암의 발생 원인은 분명치 않으나 감 염된 담즙과 간내 결석에 의한 담관상피세포의 만성적인 자극이 원인이라는 보고가 있고19 최근 보고에 의하면 분자 생물학적 수준에서의 관련성을 제시한 경우도 있다.20 간내담관 결석의 근본적 치료방법으로 간절제술이 보편 화되었으나 간절제 범위에 따른 주술기 합병증과 수술 후 잔류결석에 의한 담관염의 재발, 염증성 가성 종양의 발생 에 관한 다양한 보고가 있다. 여기에 따르면 1990년대 초까 지만 해도 좌측 간내담관 결석의 이환된 분절만 제거하는 좌외측구역 절제술이 대부분의 기관에서 이루어졌고21 이 는 좌외측구역 절제술의 수기가 간편하며 수술 시간도 단 축시킬 수 있고 수술 중 출혈량도 좌간 절제술보다 적을 것이라는 생각에서 이루어진 듯하다.
Table 1. Results of hepatectomy for treatment of intrahepatic stones
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Left lateral Left hemihep-
sectionectomy atectomy p-value (n=14) (n=18)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Sex NS
Male 3 7
Female 11 11
Age (mean) 59.0 55.3 NS
(±9.9) (±9.9)
Bleeding (ml) 294.6 406.0 NS
(±345.5) (±177.0)
Duration of 220.0 255.0 NS
surgery (minutes) (±41.6) (±49.8)
Postoperative complication 6 1 <0.05
Bile leakage 3 1
Intraabdominal abscess 1 0 IPT*, hepatic granuloma 2 0
Combined CC† 2 0 NS
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*IPT = inflammatory pseudotumor, †CC = cholangiocarcinoma.
최근들어 영상 기술의 발달로 간내담관의 해부구조를 더 자세히 알게 되었고 안정적인 간절제가 가능하게 되어 좌 외측구역 절제술보다 좌간절제술을 선호하게 되었다. Sun 등21은 좌측 간내담관 결석의 수술적 치료에 대한 보고에서 좌간절제술과 비교한 좌외측구역 절제술은 수술 시간과 수 술 중 출혈량 및 주술기 합병증에서 통계적으로 유의한 차 이가 없었으나 수술 후 발생한 복강내 농양과 담즙 누출 및 장기 추적결과 잔류 결석 발생률은 좌간절제술 시에 통 계적으로 유의하게 낮은 발생률을 나타내었다. 본 연구에 서도 좌외측구역 절제술을 시행한 예에서 수술 후 좌내측 구역에 염증성 가성 종양이 발생한 경우가 1예 있었고, 좌 내측구역에 잔류 결석과 육아종이 발생한 경우가 1예 있었 다.
또한 좌측 간내담관 결석의 수술적 치료에 있어서 좌간 절제술의 장점을 주장한 앞의 연구결과를 뒷받침 할만한 보고가 있었는데3 여기에 따르면 좌내측구역 담관은 몇 가 지 형태로 좌측 간내담관과 합류한다고 알려져 있으며 즉, 좌측 담관으로 분지하는 경우가 35%, 좌외측 상하담관의 합류부(B2, B3)로 분지되는 경우가 25%, 좌외측 하부담관 (B3)으로 분지되는 경우가 20%, 좌우 간내담관의 합류부로 분지되는 경우가 6%로 분석되었다. 이와 같은 담관의 분지 형태를 근거로 좌외측구역 담관 결석의 수술적 치료로 좌 외측구역 절제수술을 시행했을 경우 좌내측구역 담관(B4) 이 좌외측구역 담관(B2, B3)으로 담즙이 모아지는 해부구 조를 가졌을 때 좌내측구역 담관(B4)에서의 담즙배설 장애 를 유발하여 담즙 누출, 간내담관 결석 재발 등의 합병증이 발생할 수 있다. 본 연구에서 결과와 비교하면 좌내측구역 담관 분절이 좌외측 상하 담관의 합류부(B2, B3)로 분지되 는 형태의 담관 분지를 가지는 환자에서 좌외측구역 절제 술 후에 좌내측구역에 농양이 발생한 것을 경험하였다(Fig.
4).
결론적으로 경화증이 아닌 정상 간세포를 가진 좌측 간
내담관 결석의 수술적 치료에 있어서 수술 전 영상진단에 의한 좌측 간내담관의 해부학적 구조를 명확하게 확인할 수 없다면 좌외측구역 절제술 후 발생하는 좌내측구역 담 관분지의 배출 장애에 의한 담관 합병증을 예방하고 간내 담관 결석증에 병발하는 담관암 발생 위험을 줄이기 위해 서 표준 좌간절제술을 시행하는 것이 좌외측구역 절제수술 에 비하여 담관해부구조의 변형가능성에 의거하여 합병증 빈도가 적을 것으로 이해되며 이 원칙은 좌외측구역 절제 술을 적응증으로 하는 모든 간내 종양의 수술적 치료에도 적용하는 것이 바람직하리라 생각한다.
참 고 문 헌
1) Fan ST, Lai ES, Wong J. Hepatic resection for hepatolithiasis.
Arch Surg 1993;128:1070-1074.
2) Hung CJ, Lin PW. Role of right hepatic lobectomy in the treat- ment of isolated right-sided hepatolithiasis. Surgery 1997;121:
130-134.
3) Cho A, Ryu M, Kinoshita T, et al. Radiological anatomy of the medial segmental bile duct of the liver assessed by CT cholangiography. Hepatogastroenterology 2003;50:945-948.
4) Song CY, Lee KS, Jeong JH, et al. Hepatic resection for intra- hepatic stones. J Korean Surg Soc 1997;52:552-558.
5) Chen DW, Tung-Ping Poon R, Liu C, Fan ST, Wong J. Imme- diate and long-term outcomes of hepatectomy for hepato- lithiasis. Surgery 2004;135:386-393.
6) Uchiyama K, Onishi H, Tani M, Kinoshita H, Ueno M, Ya- maue H. Indication and procedure for treatment of hepa- tolithiasis. Arch Surg 2002;137:149-153.
7) Park SD, Keum JW, Lee SM, et al. Surgical experiences with hepatectomy for intrahepatic stones. Korean J HBP Surg 2004;
8:105-110.
8) Park JS, Lee MK, Park JS, Kang YJ, Hoe BS, Kim CN. Cli- nical review of the hepatic resection for hepatolithiasis. Korean Fig. 4. (a) A 53-year-old man: magnetic resonance cholangiopancreatography (MRCP) imaging scans taken preoperatively, B4 branch (arrow) joined to form a single medial segmental duct, which joined the confluence of the lateral inferior (B3) and superior (B2) branches.
(b, c) Computed tomography (CT) scans taken one month after the left lateral sectionectomy show a left intrahepatic abscess formation in B4 (b, c).
a b c
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ J HBP Surg 2004;8:160-165.
9) Harris HW, Kumwenda ZL, Sheen-Chen SM, Shah A, Schec- ter WP. Recurrent pyogenic cholangitis. Am J Surg 1998;176:
34-37.
10) Koga A, Miyazaki K, Ichimiya H, Nakayama F. Choice of treatment for hepatolithiasis based on pathological findings.
World J Surg 1984;8:36-40.
11) Simi M, Loriga P, Basoli A, Leardi S, Speranza V. Intrahepatic lithiasis. Study of thirty-six cases and review of the literature.
Am J Surg 1979;137:317-322.
12) Lee SK, Seo DW, Myung SJ, et al. Percutaneous transhepatic cholangioscopic treatment for hepatolithiasis: an evaluation of long-term results and risk factors for recurrence. Gastrointest Endosc 2001;53:318-323.
13) Jeng KS, Sheen IS, Yang FS. Percutaneous transhepatic chol- angioscopy in the treatment of complicated intrahepatic biliary strictures and hepatolithiasis with internal metallic stent. Surg Laparosc Endosc Percutan Tech 2000;10:278-283.
14) Liu CL, Fan ST, Wong J. Primary biliary stones: diagnosis and management. World J Surg 1998;22:1162-1166.
15) Lee KT, Sheen PC, Tsai CC, Chen JS, Ker CG. Long-term results of one hundred and seven hepatic resections for intra-
hepatic stones. Dig Surg 1992;19:298-302.
16) Jan YY, Chen MF, Wang CS, Jeng LB, Hwang TL, Chen SC.
Surgical treatment of hepatolithiasis: long-term results. Surgery 1996;120:509-514.
17) Lee CC, Wu CY, Chen GH. What is the impact of coexistence of hepatolithiasis on cholangiocarcinoma? J Gastroenterol He- patol 2002;17:1015-1020.
18) Chen MF, Jan YY, Hwang TL, Jeng LB, Yeh TS. Impact of concomitant hepatolithiasis on patients with peripheral chol- angiocarcinoma. Dig Dis Sci 2000;45:312-316.
19) Koga A, Ichimiya H, Yamaguchi K, Miyazaki K, Nakayama F. Hepatolithiasis associated with cholangiocarcinoma. Pos- sible etiologic significance. Cancer 1985;15:2826-2829.
20) Terada T, Ueyama J, Ukita Y, Ohta T. Protein expression of double-stranded RNA-activated protein kinase (PKR) in intra- hepatic bile ducts in normal adult livers, fetal livers, primary biliary cirrhosis, hepatolithiasis and intrahepatic cholangiocar- cinoma. Liver 2000;20:450-457.
21) Sun WB. Han BL. Cai JX. The surgical treatment of isolated left-sided hepatolithiasis: a 22-year experience. Surgery 2000;
127:493-497.