Renal arteries are usually is the largest paired visceral branches of the abdominal aorta. A single renal artery supplies each kidney in most individuals. The renal ar- teries typically arise just below the origin site of the su- perior mesenteric artery and they travel laterally behind the renal veins (1, 2). Among the various types of renal
artery anomalies, the most clinically important variation is the accessory renal artery. Accessory renal arteries are especially important in situations when accurate de- piction of the renal circulatory system is required. These situations include surgical reconstruction of the abdomi- nal aorta, renal transplantation and renovascular hyper- tension (3-5).
When studying the radiographs of the abdomen and pelvis, abnormally vertical renal axes were seen in some patients. Some of these patients had underlying diseases such as scoliosis of the lumbar spine, horseshoe kid- neys, renal masses, renal cysts or other retroperitoneal lesions that might cause a mass effect (6, 7). In clinical
Radiologic Evaluation of the Renal Axis in Patients with an Accessory Renal Artery
1Joon Ho Choi, M.D., Hyoung Jung Kim, M.D., Joo Won Lim, M.D., Young Tae Ko, M.D., Eun-Ha Lee, M.D.2
1Department of Radiology, Kyung Hee University Medical Center, Korea
2Department of Preventive Medicine, Seoul National University College of Medicine, Korea
Received September 24, 2009 ; Accepted October 27, 2009
Address reprint requests to : Hyoung Jung Kim, M.D., Department of Radiology, Kyung Hee University Medical Center, 1, Heogi-dong, Dongdaemun-gu, Seoul 130-702, Korea.
Tel. 82-2-958-8623 Fax. 82-2-968-0787 E-mail: seonju98@hanmail.net
Purpose: The purpose of this study is to evaluate the association between an accessory renal artery (ARA) and the renal axis seen on radiographs.
Materials and Methods: The MDCT axial images of 428 patients were used to detect the presence of an ARA and its location. The plain radiographs were used to measure the renal axis angle, which was the angle between the longitudinal spinal axis and the renal axis. We correlated these results to determine the association between an ARA and the renal axis.
Results: Of the 856 kidneys (428 patients), 19 kidneys had an ARA in the upper pole, 63 kidneys had an ARA in the hilum and 20 kidneys had an ARA in the lower pole.
The mean renal axis angles of these three groups were 16.7 degrees, 15.9 degrees and 11.2 degrees respectively. The mean renal axis angle without an ARA was 16.8 de- grees. The renal axis angles with an ARA in the upper pole or hilum showed no signifi- cant differences compared to those without an ARA. However, the renal axis angle with an ARA in the lower pole was significantly smaller than those without an ARA.
Conclusion: On plain radiographs, the axis of kidneys with an ARA in the lower pole maybe more vertical than those without an ARA.
Index words :Renal axis
Accessory renal artery Radiography
practice, we have experienced several cases of vertical renal axes where an accessory renal artery was found in the lower pole of the kidney. This led us to suspect the association between the renal axis and the accessory re- nal artery not only in the lower pole, but also in the up- per pole and the hilum. To the best of our knowledge, there have been no previous studies on the relationship between these two factors. The purpose of this study is to evaluate the association between an accessory renal artery and the renal axis seen on radiographs.
Materials and Methods
Study Population
From March 1, 2008 to April 1, 2008, 500 consecutive patients who underwent abdominal multidetector row computerized tomography (MDCT) were chosen for possible entrance into this study. The patients with no arterial phase images or 3-D angiography images were chosen because the patients who underwent these stud- ies usually had an underlying disease such as a renal mass or chronic renal disease. Therefore, we used the axial images that were taken during the portal phase as the reference standard. Fifty patients were excluded from this study because they’d had no radiographs tak- en in the past. Additional, another 22 patients were ex- cluded from this study because of various reasons that might have an effect on the renal axis; 12 cases of lum- bar spine scoliosis, two cases of renal mass, two cases of renal cysts, two cases of polycystic kidneys, one case of a post-kidney transplantation state, one case of nephrec- tomy, one case of hematoma in the psoas muscle and one case of autosomal dominant polycystic kidney dis- ease. The final study population was 428 patients (244 males and 184 females; age range: 4-85 years, mean age: 55.7 years). Since there were two kidneys in each patient, a total of 856 kidneys were examined. The radi- ographs used in this study were the KUB (n = 127), the IVP (n = 102), the simple abdominal radiograph in the supine position (n = 136) and the lumbar spine AP view (n = 63). CT topograms were not used because clear vi- sualization of the renal poles was difficult with using this modality.
CT Examination
MDCT examinations were performed on a 16-detector row CT scanner (LightSpeed Pro; General Electric Medical System, Milwaukee, WI, USA) or on a 64-detec- tor row CT scanner (Brilliance 64; Philips Medical
Systems, Cleveland, OH, USA). The parameters for the 16-detector row CT were a gantry rotation speed of 0.5 seconds, a detector configuration of 1.25 mm×16 mm and a table feed of 20 mm per gantry rotation. The para- meters for the 64-detector row CT scanner were a gantry rotation speed of 0.75 seconds, a detector config- uration of 0.625 mm × 64 mm and a table feed speed of 40 mm per gantry rotation. The MDCT procedure and breathing techniques were explained to each patient be- fore scanning. A 20-gauge peripheral or central line was inserted into a median cubital vein for administering in- travenous contrast material. Any oral contrast medium was not given. A power injector was used to inject 100 mL of iopromide (Ultravist 370; Schering, Berlin, Germany) through the veins at a flow rate of 3 mL/s.
The portal phase was defined as 70 seconds after the in- jection of the contrast media. Continuous 5-mm-thick sections and 5-mm intervals were used for both scan- ners for the axial images.
Image Interpretation
All image interpretation was performed on a PACS monitor. The senior resident measured the angle of the renal axis. On the radiographs, the angle between the longitudinal axis of the spine and the renal axis was measured and this was rounded off to the first decimal point. The longitudinal axis of the spine was decided by
Fig. 1. A 44-year-old male. The longitudinal axis of the spine was determined by drawing a line (a) from the spinous process of the first lumbar vertebra to the spinous process of the fifth lumbar vertebra. A perpendicular line (b) was drawn to this longitudinal axis (a) and the angle (c) between this line and the renal axis (d) was measured and rounded off to the first deci- mal. The angle (e) between the longitudinal axis of the spine and the renal axis was obtained by subtracting angle (c) from 90 degrees.
drawing a line from the spinous process of the first lum- bar vertebra to the spinous process of the fifth lumbar vertebra. The renal axis was decided by drawing a line from the upper most pole to the lower most pole (Fig. 1).
Four weeks later, two radiologists reviewed all the pa- tients’ MDCT images for the presence of accessory renal arteries and they reached a consensus. One radiologist had 9 years experience and the other radiologist was a resident with 3 years of training. The MDCT images were reviewed for the presence of accessory renal arter- ies. The accessory renal artery was defined as an ex-
trarenal artery originating from the aorta and entering directly into the renal capsule or the renal hilum (8). The distributions of the accessory renal arteries were divid- ed into three groups; the upper pole of the right/left kid- ney, the hilum of the right/left kidney and the lower pole of the right/left kidney.
Statistical Analysis
In each group, the angles of the right and left kidneys were compared with each other. The Wilcoxon signed- rank test was used, and a p value of less than 0.05 indi-
Fig. 2. A 32-year-old female. The intravenous pyelography film of the left kidney with no accessory renal arteries. The angle between the renal axis and the longitudinal axis of the spine was 19.6 degrees.
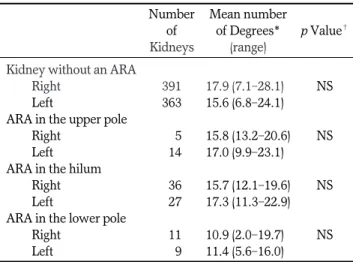
Table 1. Association of an Accessory Renal Artery (ARA) with the Renal Axis Angle Seen on Radiographs
Number Mean number of of Degrees* p Value� Kidneys (range)
Kidney without an ARA
Right 391 17.9 (7.1-28.1)0 NS
Left 363 15.6 (6.8-24.1)0
ARA in the upper pole
Right 005 15.8 (13.2-20.6) NS
Left 014 17.0 (9.9-23.1)0
ARA in the hilum
Right 036 15.7 (12.1-19.6) NS
Left 027 17.3 (11.3-22.9)
ARA in the lower pole
Right 011 10.9 (2.0-19.7)0 NS
Left 009 11.4 (5.6-16.0)0
Note.- The angles of the right and left kidneys were compared to each other in each group; NS = non-significant
*The angle between the renal axis and the longitudinal axis of the spine.
�Significance between the right and left kidneys in each group.
A B C
Fig. 3. A 57-year-old female.
A. The intravenous pyelography film of the left kidney. The angle between the renal axis and the longitudinal axis of the spine was 20.6 degrees.
B, C. Axial images of the CT scan taken during the portal phase show an accessory renal artery originating from the aorta (B, arrow) and inserting directly into the upper pole (C, arrow).
cated that the results had a statistically significant differ- ence. We then we used ANOVA to compare the angles of the four groups with one another. If the results showed that some groups had significant differences with each other, then a post-hoc test was done to deter- mine which two groups were involved. The SPSS pro- gram for Windows (Version 16.0, SPSS Inc., Chicago, Illinois, USA) was used for all the statistical analysis.
Results
The mean angles of the right and left kidneys, accord- ing to the location of the accessory renal artery, are
shown in Table 1. There were no significant differences between the right and left kidneys in every group.
The mean angle of the kidneys without an accessory renal artery (n = 754; right: 391, left: 363) was 16.8 de- grees (range: 6.8 - 28.1 degrees) (Fig. 2). The mean angle of the kidneys with an accessory renal artery in the up- per pole (n = 19; right: 5, left: 14) was 16.7 degrees (range: 9.9 - 23.1 degrees) (Fig. 3). The mean angle of the kidneys with an accessory renal artery in the hilum (n = 63; right: 36, left: 27) was 15.9 degrees (range: 11.3 - 22.9 degrees) (Fig. 4). The mean angle of the kidneys with an accessory renal artery in the lower pole (n = 20;
right: 11, left: 9) was 11.2 degrees (range: 2.0 - 19.7 de-
A B C
Fig. 4. A 31-year-old female.
A. Intravenous pyelography film of the left kidney. The angle between the renal axis and the longitudinal axis of the spine was 20.1 degrees.
B, C. The axial images of the CT scan taken during the portal phase show an accessory renal artery originating from the aorta (B, ar- row) and inserting directly into the middle pole (C, arrow).
A B C
Fig. 5. A 65-year-old male.
A. The intravenous pyelography film of the left kidney. The angle between the renal axis and the longitudinal axis of the spine was 5.6 degrees.
B, C. The axial images of the CT scan taken during the portal phase show an accessory renal artery originating from the aorta (B, ar- row) and inserting directly into the lower pole (C, arrow).
grees) (Fig. 5). These results showed that there were no significant differences among the first three groups;
those without an accessory renal artery, those with an accessory renal artery in the upper pole and those with an accessory renal vein in the hilum. However, the group with an accessory renal artery in the lower pole had significant differences compared with these three groups (p < 0.05) (Table 2).
Discussion
There are several conditions that may cause an abnor- mal renal axis. These include horseshoe kidneys, spina bifida or retroperitoneal tumors such as renal tumors (6, 7). But as we studied the radiographs of the patients without these underlying diseases, we noticed some kid- neys that had unusually vertical axes. Further studies showed that some of these patients had an accessory re- nal artery in the lower pole. This led us to believe that an accessory renal artery was another condition that may result in an abnormal renal axis.
Different variations of the renal arteries are caused by the development of the mesonephric arteries during the process of embryogenesis. A vascular network that orig- inates from the mesonephric arteries supplies the kid- neys, the suprarenal glands and the gonads located on both sides of the aorta. This network is known as the rete arteriosum urogenitale and it is located between the sixth cervical vertebra and the third lumbar vertebra.
During the sixth through the ninth week of gestation, the kidneys ascend from their original location in the pelvic cavity to the first lumbar vertebra level, while maintaining their arterial supply from these mesonephric arteries. Over time, most of the arteries regress in a sequential fashion and leave only one mesonephric artery. This becomes the single main renal artery (9-11). During this ascent, the psoas muscle, which travels inferolaterally in an oblique fashion, has
an effect on the renal axis. The upper pole comes to lie more closely to the lumbar spine than the lower pole.
But when one of the mesonephric arteries fails to regress, an accessory renal artery is formed and this ad- ditional vascular structure is thought to have an influ- ence on the renal axis. When this accessory renal artery is formed in the upper pole, there is no significant change in the renal axis because the upper pole is natu- rally closer to the spinal axis. The accessory renal artery that enters the hilum also has no effect on the renal axis because it courses along the main renal artery.
However, an accessory renal artery in the lower pole is suspected of giving resistance to the lower pole and so this kidney moves farther away from the spinal axis.
Accessory renal arteries were previously defined as aberrant arterial branches that originated directly from the aorta and they usually served a small portion of the kidney (11-13). Kadir et al. (8) divided these accessory renal arteries into two types. The common type is when the accessory artery enters into the renal hilum along with the main renal artery. The other type is when the accessory artery enters directly into the capsule of the polar regions. Ozkan et al. (14) named the second group of accessory renal arteries polar or aberrant arteries.
There are a few other renal vascular variations that must be differentiated from an accessory renal artery (15, 16). The extrahilar branching variant is when the main renal artery branches before it reaches the renal hilum. When this occurs within 2 cm of the renal artery origin, it is referred to as an early branching artery (17).
Detection of this variant is important before renal trans- plantations because a proper anastomosis is needed.
Another variant is capsular arteries where tiny arteries perfuse the renal capsule. They may arise from the main renal arteries, the renal artery branches or other retroperitoneal vessels (15, 16).
Although conventional angiography has traditionally been used for evaluating renal artery variations, it is a very invasive and time-consuming procedure that uses large amounts of ionizing radiation and nephrotoxic con- trast media (18). Therefore, the minimally invasive MD- CT angiography has replaced conventional angiography as the gold standard for evaluating kidneys via vascular imaging (19). Even though a plain radiograph can never replace MDCT angiography for detecting an ARA, a more vertical renal axis seen on a plain radiograph might warn the radiologist of a possible ARA in the low- er pole, which will lead to a more careful observation of the MDCT angiograms.
Table 2. Association of an Accessory Renal Artery (ARA) with the Renal Axis Angle seen on Radiographs
Number of Mean number Kidneys of Degrees* (range) Kidney without an ARA 754 16.8 (6.3-28.1) ARA in the upper pole 019 16.7 (9.9-23.1) ARA in the hilum 063 015.9 (11.3-22.9) ARA in the lower pole 020 11.2 (2.0-19.7) Note. - The angle of the renal axis in each of the four groups.
*The angle between the renal axis and the longitudinal axis of the spine.
Our study has several limitations. First, our study showed an ARA occurrence rate of 13.5% which was slightly lower compared to that of a previous study by Kawamoto et al. (20), which reported that accessory re- nal arteries were found in 17.6% of 74 kidneys. This dif- ference may be due to fact that we used the MDCT axial scan images that were taken during the portal phase with a 5 mm thickness as the reference standard, unlike the previous study that used MDCT angiography im- ages during the arterial phase to detect the presence of an accessory renal artery. We chose the portal phase im- ages rather than the arterial phase images because the patients who underwent arterial phase scans usually had underlying renal diseases. By using the arterial phase images as the reference standard, more patients would have been excluded, and so this would have led to a much smaller pool of subjects. Since the branching of every accessory renal artery from the aorta was thor- oughly examined, the possibility of misinterpreting an accessory renal artery with an accessory renal vein was minimized. Second, the renal poles were unclear on some of the radiographs, which might have led to some error in determining the renal axis. Since the angle of the renal axis was measured manually by a single ob- server, there might have been some error in measure- ment. To minimize these errors, we studied a larger pool of patients than that of the previous studies, and since the presence of the ARA was unknown when the renal axis was determined and the angle was measured, there was no bias toward a certain group.
In conclusion, the angle of the axis of the kidneys with an ARA in the hilum and the upper pole showed no sig- nificant differences compared to those kidneys without an ARA. However, the angle of the axis in the kidneys with an ARA in the lower pole was significantly smaller, and this resulted in a more vertical renal axis being seen on simple radiographs.
References
1. el-Galley RE, Keane TE. Embryology, anatomy, and surgical appli- cations of the kidney and ureter. Surg Clin North Am 2000;80:381- 401
2. Kadir S. Kidneys. In: Kadir S. Atlas of normal and variant angio- graphic anatomy. Philadelphia, Pa: W. B. Saunders, 1991:387-428 3. Langos J, Docolomansk A, Blazicek P, Novotn J, Krcmery S,
Rozhold Z, et al. Accessory renal arteries and their significance in the pathogenesis of systemic hypertension. Bratisl Lek Listy 1972;58:188-198
4. Tsakadze LO, Solovev VA. Multiple renal arteries and their impor- tance in surgery of aneurysm of the abdominal aorta. Vestn Khir 1975;114:53-58
5. Oesterwitz H, Strobelt V, Scholz D, Mebel M. Extracorporeal mi- crosurgical repair of injured multiple donor kidney arteries prior to cadaveric allotransplantation. Eur Urol 1985;11:100-105
6. Fernbach SK, Davis TM. The abnormal renal axis in children with spina bifida and gibbus deformity - the pseudohorseshoe kidney. J Urol 1986;136:1258-1260
7. Mandell GA, Maloney K, Sherman NH, Filmer B. The renal axes in spina bifida: issues of confusion and fusion. Abdom Imaging 1996;21:541-545
8. Kadir S. Angiography of the kidneys. In: Kadir S. Diagnostic angiogra- phy. Philadelphia, Pa: W. B. Saunders, 1986:445-495
9. Boijsen E. Anomalies and malformations. In: Baum S. Abrams’ an- giography, 4th ed. Philadelphia: Little, Brown and Company, 1997:1217-1229
10. Felix W. Die Entwicklung der Harn-und Geschlechts-organe. In:
Keibel K, Mali FP. Handbuch der Entwicklungs-geschichte des Menschen. Leipzig: Hirzel, 1911:732
11. Larsen, WJ. Human embryology. New York, NY: Churchill Livingstone, 1993:235-253
12. Satyapal KS, Haffejee AA, Singh B, Ramasaroop L, Roobs JV, Kalideen JM. Additional renal arteries: incidence and morphome- try. Surg Radiol Anat 2001;23:33-38
13. Glodny B, Cromme S, Wortler K, Winde G. A possible explanation for the frequent concomitance of arterial hypertension and multi- ple renal arteries. Med Hypotheses 2001;56:129-133
14. Ozkan U, Oguzkurt L, Tercan F, Kizilkilic O, Koc Z, Koca N. Renal artery origins and variations: angiographic evaluation of 855 con- secutive patients. Diagn Interv Radiol 2006;12:183-186
15. Renal vasculature. In: Netter FH, Shapter RK, Yonkman FF. The Ciba collection of medical illustrations: kidneys, ureters, and urinary bladder. Vol. 6. Summit, NJ: Ciba-Geigy, 1979:15-17
16. Cuttino JT, Clark RL. The normal vasculature of the genitourinary tract: embryology, anatomy, and hemodynamics. In: Hillman BJ.
Clinical urography. Vol. 3. Philadelphia, Pa: Saunders, 1990:2076- 2091
17. Raman SS, Pojchamarnwiputh S, Muangsomboon K, Schulam PG, Gritsch HA, Lu DS. Surgically relevant normal and variant renal parenchymal and vascular anatomy in preoperative 16-MDCT evaluation of potential laparoscopic renal donors. AJR Am J Roentgenol 2007;188:105-114
18. Rydberg F, Kopecky KK, Tann M, Persohn SA, Leapman SB, Filo RS, et al. Evaluation of prospective living renal donors for laparo- scopic nephrectomy with multisection CT: the marriage of mini- mally invasive imaging with minimally invasive surgery.
Radiographics 2001;21:S223-S236
19. Fishman EK. From the RSNA refresher course: CT angiography:
clinical applications in the abdomen. Radiographics 2001;21:S3-S16 20. Kawamoto S, Montogomery RA, Lawler LP, Horton KM, Fishman
EK. Multidetector CT angiography for preoperative evaluation of living laparoscopic kidney donors. AJR Am J Roentgenol 2003;180:
1633-1638
대한영상의학회지 2010;62:263-269
부 신동맥이 있는 사례에서 신장 축의 방사선학적인 평가1
1경희의료원 영상의학과
2서울대학교병원 예방의학과
최준호∙김형중∙임주원∙고영태∙이은하2
목적: 부 신동맥과 신장축의 연관성을 방사선학적으로 평가하고자 하였다.
대상과 방법: 2008년 3월 1일부터 2008년 4월 1일까지 총 428명 환자의 복부 컴퓨터단층촬영 사진을 조사하였다.
부 신동맥의 유무를 평가하는데 문맥기 시기에 촬영한 사진만 사용하였다. 그리고 방사선 사진에서 척추의 장축과 신장축이 이루는 각도를 측정하였다. 그 후에 부 신동맥과 신장축과의 연관성을 조사하였다.
결과: 428명의 환자 (총 856개의 신장) 중에 19개의 신장은 상극에 부 신동맥이 있었고, 63개의 신장은 신문에 부 신동맥이 있었고, 20개의 신장은 하극에 부 신동맥이 있었다. 신장축의 평균 각도는 신장의 상극에 부 신동맥이 있 는 경우에 16.7도, 신문에 부 신동맥이 있는 경우는 15.9도, 신장의 하극에 부 신동맥이 있는 경우는 11.2도이었다.
신장에 부 신동맥이 없는 경우는 신장축의 평균 각도가 16.8도 이었다. 부 신동맥이 신장의 상극과 신문에 있는 경 우에 신장축의 각도는 부 신동맥이 없는 신장축의 각도와 유의한 차이가 없었다. 그러나 신장의 하극에 부 신동맥이 있는 경우는 신장축의 각도가 유의한 차이를 보이는 작은 수치로 측정되었다.
결론: 부 신동맥이 신장의 하극에 존재한 경우, 부 신동맥이 없는 신장보다 비교적 곧추선 신장축이 방사선 사진에서 관찰되었다.