Current Status of Recanalization Therapy in Acute Ischemic Stroke with Symptomatic Intracranial Arterial Occlusion
in Korea
Min Uk Jang,MD,*Jeong-Ho Hong,MD,† Jihoon Kang,MD,†Beom Joon Kim, MD,†
Moon-Ku Han,MD,† Byung-Chul Lee,MD,‡Kyung-Ho Yu, MD,‡ Mi Sun Oh, MD,‡
Keun-Sik Hong,MD,xYong-Jin Cho,MD,xJong-Moo Park,MD,kKyusik Kang, MD,k Jae Kwan Cha, MD,{ Dae-Hyun Kim,MD,{Tai Hwan Park, MD,#
Kyung Bok Lee, MD,**Soo Joo Lee, MD,†† Youngchai Ko, MD,†† Jun Lee, MD,‡‡
Ki-Hyun Cho, MD,xxJoon-Tae Kim,MD,xxJuneyoung Lee, MD, PhD,kk Ji Sung Lee, MD, PhD,{{ and Hee-Joon Bae, MD†
Background: Recent methodological advances in recanalization therapy may alter recanalization strategies and clinical outcomes in patients with symptomatic occlu- sion of intracranial cerebral arteries. However, few studies have analyzed these changes at a national level, with none conducted in Korea.Methods:On the basis of a prospective multicenter stroke registry database in Korea, 642 consecutive pa- tients hospitalized within 12 hours of the onset with symptomatic occlusion of intra- cranial major cerebral arteries between March 2010 and November 2011 were identified. Recanalization therapy was used in 48% (n5 307) of patients; intrave- nous thrombolysis only (IVT) in 46%, intra-arterial thrombolysis only (IAT) in 16%, and combined thrombolysis (CMT) in 38%. Of the 166 patients treated by IAT or CMT, the Penumbra system or the Solitaire was used in 58% of patients.Re- sults:Early neurologic improvement (ENI), 3-month modified Rankin scale (mRS) score of 2 or less, and symptomatic hemorrhagic transformation (SHT) were observed in 43%, 39%, and 9% of the patients in the IVT group; 52%, 27%, and 12% of the patients in the IAT group; and 54%, 39%, and 12% of the patients in the CMT group, respectively. Compared with no treatment, adjusted odd ratios (95% confidence intervals) of recanalization therapy were 1.59 (1.04-2.42) for ENI,
From the *Department of Neurology, Hallym University Sacred Heart Hospital, Chuncheon; †Department of Neurology, Seoul Na- tional University Bundang Hospital, Seongnam; ‡Department of Neurology, Hallym University Sacred Heart Hospital, Anyang;
xDepartment of Neurology, Ilsan Paik Hospital, Inje University, Goyang;kDepartment of Neurology, Eulji General Hospital, Eulji University School of Medicine, Seoul;{Department of Neurology, Dong-A University Hospital, Pusan; #Department of Neurology, Seoul Medical Center, Seoul; **Department of Neurology, Soonchun- hyang University College of Medicine, Seoul; ††Department of Neurology, Eulji University Hospital, Eulji University School of Med- icine, Daejeon; ‡‡Department of Neurology, Yeungnam University Medical Center, Daegu;xxDepartment of Neurology, Chonnam Na- tional University Hospital, Gwangju;kkDepartment of Biostatistics, Korea University College of Medicine, Seoul; and{{Biostatistical
Consulting Unit, Soonchunhyang University Medical Center of Biostatistics, Seoul, Korea.
Received October 21, 2013; revision received December 9, 2013;
accepted December 16, 2013.
This study was supported by a grant of the Korea Healthcare Tech- nology R&D Project, Ministry of Health and Welfare, Republic of Ko- rea (HI10C2020).
Address correspondence to Hee-Joon Bae, MD, Department of Neurology, Seoul National University Bundang Hospital, 82 Gumi- ro 173 Beon-gil, Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea. E-mail:[email protected].
1052-3057/$ - see front matter Ó 2014 by National Stroke Association
http://dx.doi.org/10.1016/j.jstrokecerebrovasdis.2013.12.027
Journal of Stroke and Cerebrovascular Diseases, Vol. 23, No. 5 (May-June), 2014: pp e339-e346 e339
1.37 (.81-2.30) for 3-month mRS score of 2 or less, and 2.58 (1.12-5.91) for SHT.Con- clusions:The variety and active use of endovascular approaches were quite notice- able. As a whole, recanalization therapy tended to contribute to favorable outcomes despite a significant increase of symptomatic hemorrhage. Key Words:
Recanalization therapy—endovascular treatment—thrombolysis—acute ischemic stroke—intracranial arterial occlusion—Korea—outcome—registry.
Ó 2014 by National Stroke Association
Introduction
Intracranial large vessel occlusion accounts for up to 40% of ischemic stroke and is known as an independent predictor of poor outcome.1,2 The recent advances in endovascular devices have made them a major emerging target for stroke intervention.3,4
The unsatisfactory efficacy of intravenous tissue plas- minogen activator (IV t-PA) can be partly attributed to low reperfusion rates.5-7New mechanical thrombectomy devices have been developed to achieve higher recanalization and lower hemorrhagic transformation rates.3,4,8,9 The success of these devices is change the practice; in the United States, the use of endovascular devices increased 6-fold between 2004 and 2009.10How- ever, this technical success has not been proven to improve a clinical outcome through adequately powered randomized clinical trials.11
Few studies described how acute intracranial large vessel occlusion was treated and what the treatment outcome was in a nationally representative popula- tion.5,12,13Furthermore, these few studies had a limitation that they did not compare various recanalization strategies with respect to clinical outcomes.
Aims
The aims of the present study were to describe—among ischemic stroke patients who presented within 12 hours of the onset, when diagnosed with symptomatic intracra- nial occlusion of major cerebral arteries and were hospi- talized to nationally representative regional stroke centers in South Korea—the following: (1) which of the patients were treated with recanalization therapy; (2) what strategies were applied to them; and (3) what were the treatment outcomes.
Methods Study Subjects
A consecutive series of patients who were hospitalized because of acute ischemic stroke between March 1, 2010 and November 31, 2011 were identified from a prospec- tive, multicenter, nationwide web-based acute stroke reg- istry database in Korea.14,15Ten university hospitals or regional centers participated in this study. They are
scattered throughout a major part of South Korea; 5 metropolitan areas: Seoul (the largest one), Pusan (the second largest one), Daegu, Kwangju, and Daejeon and the largest provincial area, Gyeonggi; more than 60%
of the Korean population resides in these areas (Supplementary Figure 1).
Among these patients, those who met the following criteria were included in this study: (1) the time interval from their first symptom onset to arrival at 12 hours or earlier, (2) a clinical diagnosis of acute ischemic stroke confirmed by relevant lesions on brain images; and (3) intracranial major cerebral artery occlusion on initial angiographic evaluation including magnetic resonance angiography, computed tomography angiography, or dig- ital subtraction angiography. Intracranial major cerebral arteries were defined as the distal portion of the internal carotid artery (d-ICA), anterior cerebral artery, middle ce- rebral artery (MCA), posterior cerebral artery (PCA), or basilar artery (BA). Patients who did not undergo angio- graphic evaluation or who had occlusion of proximal ICA or proximal vertebral artery were excluded. Patients who received recanalization therapy were divided into 2 groups: an intravenous thrombolysis only (IVT) group and an endovascular treatment (EVT) group. EVT included intra-arterial use of chemical thrombolytic agents, clot maceration by multiple passages of a micro- catheter/microwire through the clot,16use of mechanical thrombectomy devices, and stent placement. The EVT group was further divided into an intra-arterial thrombol- ysis only (IAT) group and a combined thrombolysis (CMT) group.
In all participating centers, approval was obtained from the institutional review boards for collection of anonymized clinical data without patients’ consent into the stroke registry database to improve the quality of stroke care. We got further approval for collection of additional data and the use of the registry database for this study.
Data Collection
Patients’ clinical and laboratory information and 3- month functional outcome were obtained directly from the registry database or by reviewing medical records.
Digital subtraction angiography images of patients who underwent EVT were collected from each center, and
successful recanalization, defined as achieving thrombol- ysis in cerebral infarction IIa, IIb, or III flow17in all treat- able vessels, was determined by independent assessment of 2 stroke neurologists (M.U.J, J-H.H) who were blinded to clinical outcomes. The discrepancies in thrombolysis in cerebral infarction scoring were resolved by consensus (kappa value5 .83).
Early neurologic improvement (ENI) was defined as a discharge National Institutes of Health stroke scale (NIHSS) score of 0 or 1 or an improvement of 8 or more in the NIHSS score from the baseline to the discharge.18 Favorable functional outcome was defined as a 3-month modified Rankin scale (mRS) score of 2 or less. Safety
outcome was symptomatic intracranial hemorrhage (SHT) defined as any hemorrhage plus a neurologic dete- rioration of 4 points or more in the NIHSS score from the baseline or from the lowest NIHSS value after the base- line, or leading to death.19
Statistical Analysis
Comparisons of baseline characteristics and clinical outcomes were made between patients who had recanali- zation therapy and those who did not, between the IVT and EVT groups, between the IAT and CMT groups, and according to major endovascular devices in the EVT
Table 1. Comparisons of baseline characteristics between patients with and without recanalization therapy
No recanalization therapy (n5 335)
Recanalization therapy
(n5 307) P value*
Age (y)
Mean6 SD 68.36 13.9 68.86 11.7 .67
Age, 80 260 (77.6%) 249 (81.1%) .27
Age$ 80 75 (22.4%) 58 (18.9%)
Sex (male) 178 (53.1%) 189 (61.6%) .03
Onset to arrivaly
Mean6 SD 5.266 3.32 2.406 2.47 ,.001
#3 h 103 (30.7%) 228 (74.3%) ,.001
.3 and #4.5 h 53 (15.8%) 34 (11.1%)
.4.5 and #6 h 43 (12.8%) 13 (4.2%)
.6 h 136 (40.6%) 32 (10.4%)
Initial NIHSS
Median (IQR) 9 (3, 15) 15 (9, 19) ,.001
0-3 99 (29.6%) 14 (4.6%) ,.001
4-9 78 (23.3%) 68 (22.1%)
10-25 154 (46.0%) 213 (69.4%)
26-44 4 (1.2%) 12 (3.9%)
Occluded arteryz
d-ICA 42 (42.9%) 56 (57.1%) .045
ACA 20 (60.6%) 13 (39.4%) .320
MCA 213 (51.0%) 205 (49.0%) .396
PCA 64 (70.3%) 27 (29.7%) ,.01
BA 34 (47.9%) 37 (52.1%) .443
Prestroke mRS .01
0 262 (78.2%) 264 (86.0%)
$1 73 (21.8) 43 (14.0%)
Risk factors
HTN 198 (59.1%) 208 (67.8%) .01
DM 65 (19.4%) 77 (25.1%) .08
HL 51 (15.2%) 56 (18.2%) .30
Smoking 106 (31.6%) 87 (28.3%) .36
A-fib 128 (38.2%) 176 (57.3%) ,.001
Abbreviations: ACA, anterior cerebral artery; A-fib, atrial fibrillation; BA, basilar artery; d-ICA, distal portion of the internal carotid artery;
DM, diabetes mellitus; HL, hyperlipidemia; HTN, hypertension; IQR, interquartile range; MCA, middle cerebral artery; mRS, modified Rankin scale; NIHHS, National Institutes of Health Stroke Scale; PCA, posterior cerebral artery; SD, standard deviation.
Values are number of patients (%) if not indicated.
*P values are calculated by the Student t test, Pearson chi-square test, and Mann–Whitney U test, whichever appropriate.
yTime interval from last normal time to arrival at hospitals.
zValues are the number of the occluded vessels, which can be overlapped in patients who have multiple occlusions. P values were calculated by comparison of proportion of treatment between patients with and without each occlusion.
group. In comparisons by endovascular devices, the final device used was chosen as representative and the ana- lyses were limited to the cases in which the final device could be determined clearly. Three-month mRS score, ENI, and SHT were used as outcome variables. Recanali- zation rate was adopted as an outcome variable to analyze those who underwent EVT. Patients whose 3-month mRS scores were unavailable (n 5 64) were excluded from the analysis when 3-month mRS score was an outcome variable.
Multivariable logistic regression models were devel- oped for estimating the adjusted odds ratios (ORs) of recanalization therapy compared with that of no therapy, the OR of EVT compared with that of IVT, and the OR of CMT compared with that of IAT for the previously mentioned outcome variables. Variables for adjustment in each model were selected on the basis of (1) P# .20 in comparisons according to methods of recanalization therapy or (2) clinical relevance of their associations with stroke outcomes. In the models in which SHT was an outcome variable, we confined the number of variables for adjustment to no greater than 4. All analyses were per- formed using IBM SPSS 19.0.1 (IBM Corporation, Armonk, NY). A 2-tailed P, .05 was considered a mini- mum level of statistical significance.
Results
General Characteristics
During the study period, among 6070 patients who pre- sented with acute ischemic stroke, 642 patients met the eligibility criteria (Supplementary Figure 2). The occluded vessels were MCA in 65% of patients, d-ICA in 15%, PCA in 14%, BA in 11%, and anterior cerebral ar- tery in 5%. Overall, intravenous tissue plasminogen acti- vator (IV t-PA) was used in 257 patients (40.0%); .9 mg/kg in 54% and .6 mg/kg in 46% (Supplementary Table 1). The 77% of the patients in the IVT group used .9 mg/kg and the 73% in the CMT group used .6 mg/kg.
Recanalization Therapy versus no Recanalization Therapy
Compared with patients without recanalization ther- apy, those with recanalization therapy were mostly male, arrived at hospitals earlier, and had higher initial NIHSS scores (Table 1). Seventy-four percent of patients who had recanalization therapy arrived within 3 hours of the onset, whereas 41% of those who did not have recanalization therapy arrived after 6 hours. Recanaliza- tion therapy was preferred in d-ICA occlusion, and no therapy was preferred in PCA occlusion. ENI and SHT
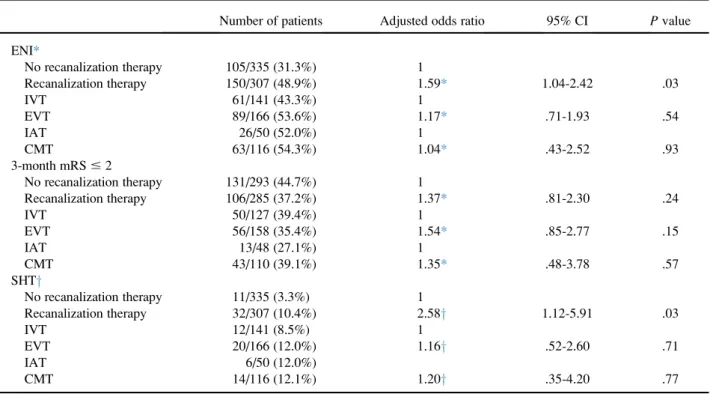
Table 2. Clinical outcomes according to methods of recanalization therapy
Number of patients Adjusted odds ratio 95% CI P value ENI*
No recanalization therapy 105/335 (31.3%) 1
Recanalization therapy 150/307 (48.9%) 1.59* 1.04-2.42 .03
IVT 61/141 (43.3%) 1
EVT 89/166 (53.6%) 1.17* .71-1.93 .54
IAT 26/50 (52.0%) 1
CMT 63/116 (54.3%) 1.04* .43-2.52 .93
3-month mRS# 2
No recanalization therapy 131/293 (44.7%) 1
Recanalization therapy 106/285 (37.2%) 1.37* .81-2.30 .24
IVT 50/127 (39.4%) 1
EVT 56/158 (35.4%) 1.54* .85-2.77 .15
IAT 13/48 (27.1%) 1
CMT 43/110 (39.1%) 1.35* .48-3.78 .57
SHTy
No recanalization therapy 11/335 (3.3%) 1
Recanalization therapy 32/307 (10.4%) 2.58y 1.12-5.91 .03
IVT 12/141 (8.5%) 1
EVT 20/166 (12.0%) 1.16y .52-2.60 .71
IAT 6/50 (12.0%)
CMT 14/116 (12.1%) 1.20y .35-4.20 .77
Abbreviations: A-fib, atrial fibrillation; CI, confidence interval; CMT, combined thrombolysis; DM, diabetes mellitus; ENI, early neurologic improvement; EVT, endovascular therapy; IAT, intra-arterial thrombolysis only; IVT, intravenous thrombolysis only; mRS, modified Rankin scale; NIHHS, National Institutes of Health Stroke Scale; SHT, symptomatic hemorrhagic transformation.
Values are number of patients (%) if not indicated.
*Adjusted for sex, onset to arrival, initial NIHSS, prestroke mRS, A-fib, and DM.
yAdjusted for onset to arrival, initial NIHSS, A-fib, and DM.
developed more frequently in patients treated with recan- alization therapy (P values,.001), and the proportion of 3-month mRS score of 2 or less was slightly higher in un- treated patients (P5.16) (Table 2). Multivariable analyses demonstrated that recanalization therapy increased the odds of ENI and SHT significantly, but not the odds of 3-month mRS score of 2 or less.
IVT versus EVT
Of the 307 patients who underwent recanalization ther- apy, 46% were treated with IVT and 54% with EVT.
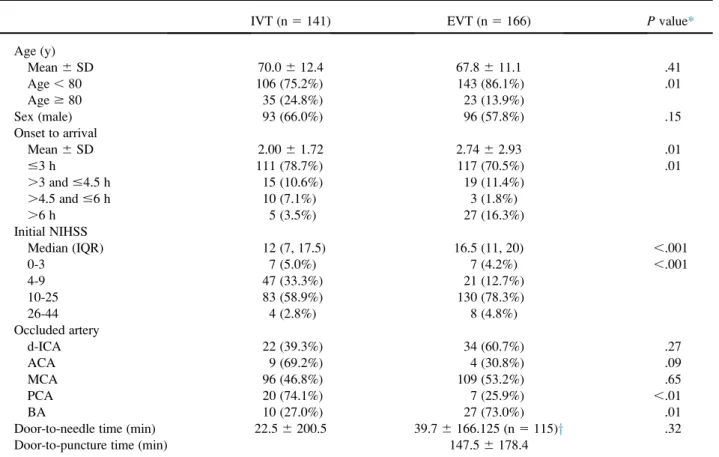
Compared with the IVT group, the EVT group was more likely to be less than 80-years old, arrive late at hos- pitals, and had higher initial NIHSS scores (Table 3). EVT was preferred in BA occlusion, and IVT was preferred in PCA occlusion. ENI tended to develop more frequently in the EVT group than in the IVT group (P5 .07); however, the proportion who had SHT and 3-month mRS score of 2 or less was not different between the 2 groups (Table 2).
Multivariable analyses revealed no significant association between EVT and the clinical outcomes.
IAT versus CMT
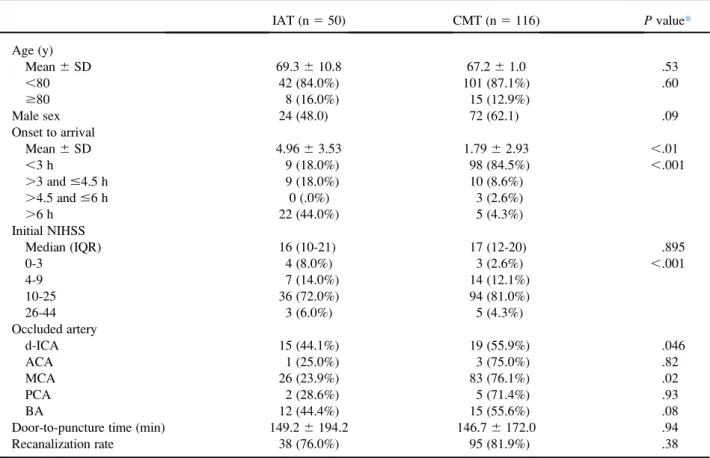
Of the 166 patients in the EVT group, 30% received IAT and 70% received CMT. The CMT group was more likely to arrive at hospitals earlier and had higher initial NIHSS scores than the IAT group (Table 4). CMT was preferred in d-ICA and MCA occlusions. The ENI and SHT rates and the proportion of mRS score of 2 or less were not significantly different between the 2 groups (Table 2). The recanalization rate was not different too (P5 .38).
Methods of EVT and Comparisons According to Endovascular Devices
Chemical thrombolytics were used in 74% of the patients in the EVT group, and urokinase was the most commonly used thrombolytic agent (91%) (Supplementary Table 1). En- dovascular devices were applied in 95% of the patients in the EVT group and the microcatheter/microwire was used most frequently. The new generation thrombectomy de- vices, such as the Penumbra system and the Solitaire, were used in 58% of the patients in the EVT group. Comparisons
Table 3. Comparisons of baseline characteristics between IVT and EVT groups
IVT (n5 141) EVT (n5 166) P value*
Age (y)
Mean6 SD 70.06 12.4 67.86 11.1 .41
Age, 80 106 (75.2%) 143 (86.1%) .01
Age$ 80 35 (24.8%) 23 (13.9%)
Sex (male) 93 (66.0%) 96 (57.8%) .15
Onset to arrival
Mean6 SD 2.006 1.72 2.746 2.93 .01
#3 h 111 (78.7%) 117 (70.5%) .01
.3 and #4.5 h 15 (10.6%) 19 (11.4%)
.4.5 and #6 h 10 (7.1%) 3 (1.8%)
.6 h 5 (3.5%) 27 (16.3%)
Initial NIHSS
Median (IQR) 12 (7, 17.5) 16.5 (11, 20) ,.001
0-3 7 (5.0%) 7 (4.2%) ,.001
4-9 47 (33.3%) 21 (12.7%)
10-25 83 (58.9%) 130 (78.3%)
26-44 4 (2.8%) 8 (4.8%)
Occluded artery
d-ICA 22 (39.3%) 34 (60.7%) .27
ACA 9 (69.2%) 4 (30.8%) .09
MCA 96 (46.8%) 109 (53.2%) .65
PCA 20 (74.1%) 7 (25.9%) ,.01
BA 10 (27.0%) 27 (73.0%) .01
Door-to-needle time (min) 22.56 200.5 39.76 166.125 (n 5 115)y .32
Door-to-puncture time (min) 147.56 178.4
Abbreviations: ACA, anterior cerebral artery; BA, basilar artery; CMT, combined thrombolysis; d-ICA, distal portion of the internal carotid artery; EVT, endovascular therapy; IQR, interquartile range; IVT, intravenous thrombolysis only; MCA, middle cerebral artery; NIHHS, Na- tional Institutes of Health Stroke Scale; PCA, posterior cerebral artery; SD, standard deviation.
Values are number of patients (%) if not indicated.
*P values are calculated by the Student t test, Pearson chi-square test, and Mann–Whitney U test, whichever appropriate.
yValues were obtained from patients receiving IVT in the CMT group.
of baseline characteristics and clinical outcomes according to the EVT devices are presented inSupplementary Table 1.
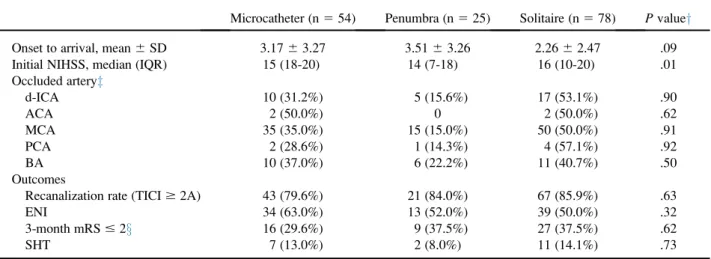
Recanalization rates ranged from 80%-86% and were com- parable among the EVT devices. The proportions of 3- month mRS score of 2 or less and the ENI and SHT rates were not different among the 3 groups.
Discussion
The proportion of patients treated with recanalization therapy within the first 3 hours was 74%. This proportion decreased to 25% beyond this time window (79 of 311 pa- tients: IVT in 30, IAT in 31, and CMT in 18 patients;
Tables 1, 3, and 4), but was still high. In a recent Japanese study, less than 10% of patients were treated with recanalization therapy, mostly by IAT.12
The proportion of EVT to recanalization therapy in this study was 56%, which is higher than 34% in the Japanese study3and 8% in a Swiss study.20The differences may be explained partly by the more aggressive application of EVT beyond the 3-hour window (62%) compared with within the 3-hour window (51%) in this study (Table 3).
More than 10% of patients with the NIHSS score less than 4 and almost half of those with NIHSS score of 4 or more but less than 10 received recanalization therapy.
These findings represent that physicians in real practice do not always withhold recanalization therapy in mild stroke patients. The present guidelines recommend avoiding recanalization therapy in patients who have mi- nor and isolated symptoms.21
Recanalization therapy increased the odds of ENI and SHT significantly. The increase of ENI by recanalization therapy was reported in the Safe Implementation of Treat- ment in Stroke–International Stroke Thrombolysis Regis- ter18and the National Institute of Neurological Disorders and Stroke (NINDS) trial,1 although these 2 studies enrolled subjects without any knowledge of vascular sta- tus. No difference between the IVT and EVT groups is compatible with the failures seen in recent EVT trials.22-24 Comparison of the IAT and CMT groups also showed no improvement in clinical outcomes by precedent IVT.
However, the imbalance of baseline characteristics and possibilities of residual and unmeasured confounders prevent generalization of these results.
Table 4. Comparisons of baseline characteristics between IAT and CMT groups
IAT (n5 50) CMT (n5 116) P value*
Age (y)
Mean6 SD 69.36 10.8 67.26 1.0 .53
,80 42 (84.0%) 101 (87.1%) .60
$80 8 (16.0%) 15 (12.9%)
Male sex 24 (48.0) 72 (62.1) .09
Onset to arrival
Mean6 SD 4.966 3.53 1.796 2.93 ,.01
,3 h 9 (18.0%) 98 (84.5%) ,.001
.3 and #4.5 h 9 (18.0%) 10 (8.6%)
.4.5 and #6 h 0 (.0%) 3 (2.6%)
.6 h 22 (44.0%) 5 (4.3%)
Initial NIHSS
Median (IQR) 16 (10-21) 17 (12-20) .895
0-3 4 (8.0%) 3 (2.6%) ,.001
4-9 7 (14.0%) 14 (12.1%)
10-25 36 (72.0%) 94 (81.0%)
26-44 3 (6.0%) 5 (4.3%)
Occluded artery
d-ICA 15 (44.1%) 19 (55.9%) .046
ACA 1 (25.0%) 3 (75.0%) .82
MCA 26 (23.9%) 83 (76.1%) .02
PCA 2 (28.6%) 5 (71.4%) .93
BA 12 (44.4%) 15 (55.6%) .08
Door-to-puncture time (min) 149.26 194.2 146.76 172.0 .94
Recanalization rate 38 (76.0%) 95 (81.9%) .38
Abbreviations: ACA, anterior cerebral artery; BA, basilar artery; CMT, combined thrombolysis; d-ICA, distal portion of the internal carotid artery; IAT, intra-arterial thrombolysis only; MCA, middle cerebral artery; NIHHS, National Institutes of Health Stroke Scale; PCA, posterior cerebral artery; SD, standard deviation.
Values are number of patients (%) if not indicated.
*P values are calculated by the Student t test, Pearson chi-square test, whichever appropriate.
With respect to the methods of mechanical EVT, the traditional microcatheter/microwire method16 was still used most commonly; however, a large proportion used new generation devices. The recanalization rates of those new generation devices were quite high, although the proportions of 3-month mRS score of 2 or less and the ENI and SHT rates were not different among these 3 commonly used EVT methods (Table 5).
Among the EVT group, the proportion of those treated by CMT was more than 2 times of those treated by IAT (Table 4). The recanalization rates of the CMT and IAT groups (82% and 76%, respectively) were higher than that of the prourokinase trial (66%)25and slightly lower than those observed in recent new generation device trials (83%
and 86%).3,4 The negligible difference in recanalization rates between the CMT and IAT groups may explain the difference in the clinical outcomes (Table 2).
Significant increase of SHT and nonsignificant im- provement of the 3-month functional outcome despite in- crease in the odds of ENI can be interpreted as that the recanalization strategies for symptomatic intracranial oc- clusion in this study do not improve the clinical outcome overall. However, high recanalization rates in the EVT group especially with new generation devices and com- bined methods and without increase of SHT suggest that the recent technical advances can bring about improvement of clinical outcomes in this population.26
This study has limitations. First, it was a retrospective observational study, although a prospectively collected database was used. Second, the hospitals participating
in this study were mostly classified as comprehensive stroke centers, which may raise concerns about the repre- sentativeness of this study at a national level. Third, because catheter-guided angiography was performed only in the EVT group, we could not directly compare the IVT group with the EVT group with respect to the recanalization rate. Fourth, it should be noted that 3- month clinical outcomes were unavailable in 10% of patients.
In conclusion, this study demonstrated the current sit- uation of recanalization strategies for acute symptomatic occlusion of intracranial cerebral arteries in Korea. The variety and active use of endovascular approaches were quite noticeable. Exploration of newer endovascular stra- tegies in the clinical trial setting is warranted.
Supplementary Data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.jstrokecerebrovasdis.2013.12.
027.
References
1.Brown DL, Johnston KC, Wagner DP, et al. Predicting ma- jor neurological improvement with intravenous recombi- nant tissue plasminogen activator treatment of stroke.
Stroke 2004;35:147-150.
2.Smith WS, Tsao JW, Billings ME, et al. Prognostic signifi- cance of angiographically confirmed large vessel intra- cranial occlusion in patients presenting with acute brain ischemia. Neurocrit Care 2006;4:14-17.
Table 5. Comparisons according to EVT devices*
Microcatheter (n5 54) Penumbra (n5 25) Solitaire (n5 78) P valuey
Onset to arrival, mean6 SD 3.176 3.27 3.516 3.26 2.266 2.47 .09
Initial NIHSS, median (IQR) 15 (18-20) 14 (7-18) 16 (10-20) .01
Occluded arteryz
d-ICA 10 (31.2%) 5 (15.6%) 17 (53.1%) .90
ACA 2 (50.0%) 0 2 (50.0%) .62
MCA 35 (35.0%) 15 (15.0%) 50 (50.0%) .91
PCA 2 (28.6%) 1 (14.3%) 4 (57.1%) .92
BA 10 (37.0%) 6 (22.2%) 11 (40.7%) .50
Outcomes
Recanalization rate (TICI$ 2A) 43 (79.6%) 21 (84.0%) 67 (85.9%) .63
ENI 34 (63.0%) 13 (52.0%) 39 (50.0%) .32
3-month mRS# 2x 16 (29.6%) 9 (37.5%) 27 (37.5%) .62
SHT 7 (13.0%) 2 (8.0%) 11 (14.1%) .73
Abbreviations: ACA, anterior cerebral artery; BA, basilar artery; d-ICA, distal portion of the internal carotid artery; ENI, early neurologic improvement; EVT, endovascular therapy; MCA, middle cerebral artery; NIHHS, National Institutes of Health Stroke Scale; PCA, posterior cerebral artery; SD, standard deviation; SHT, symptomatic hemorrhagic transformation; TICI, thrombolysis in cerebral infarction.
Values are the number of patients (%) if not indicated.
*Analysis was made on the basis of the final device used in the cases in which multiple devices were used, and 9 patients in whom the Wing- span stent was the final device were excluded from the analysis.
yP values are calculated by a 1-way analysis of variance, Kruskal–Wallis test, and Pearson chi-square test, whichever appropriate.
zValues are the number of the occluded vessels, which can be overlapped in patients who have multiple occlusions.
xPatients whose 3-month mRS scores were unavailable (n 5 7) were excluded from the analysis.
3.Saver JL, Jahan R, Levy EI, et al. Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel- group, non-inferiority trial. Lancet 2012;380:1241-1249.
4.Nogueira RG, Lutsep HL, Gupta R, et al. Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke (TREVO 2): a randomised trial. Lancet 2012;380:1231-1240.
5.Mazighi M, Serfaty JM, Labreuche J, et al. Comparison of intravenous alteplase with a combined intravenous- endovascular approach in patients with stroke and confirmed arterial occlusion (RECANALISE study): a prospective cohort study. Lancet Neurol 2009;8:802-809.
6.Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359:1317-1329.
7.Bhatia R, Hill MD, Shobha N, et al. Low rates of acute recanalization with intravenous recombinant tissue plas- minogen activator in ischemic stroke: real-world experi- ence and a call for action. Stroke 2010;41:2254-2258.
8.Smith WS, Sung G, Saver J, et al. Mechanical thrombec- tomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke 2008;39:1205-1212.
9.Grunwald IQ, Wakhloo AK, Walter S, et al. Endovascular stroke treatment today. AJNR Am J Neuroradiol 2011;
32:238-243.
10.Hassan AE, Chaudhry SA, Grigoryan M, et al. National trends in utilization and outcomes of endovascular treat- ment of acute ischemic stroke patients in the mechanical thrombectomy era. Stroke 2012;43:3012-3017.
11.Hennerici MG, Kern R, Szabo K. Non-pharmacological strategies for the treatment of acute ischaemic stroke.
Lancet Neurol 2013;12:572-584.
12.Yoshimura S, Egashira Y, Sakai N, et al. Recovery by Endovascular Salvage for Cerebral Ultra-acute Embolism- Japan retrospective survey group. Retrospective nation- wide survey of acute stroke due to large vessel occlusion in Japan: a review of 1,963 patients and the impact of endo- vascular treatment. Cerebrovasc Dis 2011;32:219-226.
13.Chao AC, Hsu HY, Chung CP, et al. Outcomes of thrombolytic therapy for acute ischemic stroke in Chinese patients: the Taiwan Thrombolytic Therapy for Acute Ischemic Stroke (TTT-AIS) Study. Stroke 2010;41:885-890.
14.Kim BJ, Han MK, Park TH, et al. Current status of acute stroke management in Korea: a report on a multicenter,
comprehensive acute stroke registry. Int J Stroke 2013.
Nov 21 [Epub ahead of print.].
15. Hong K-S, Bang OY, Kang D-W, et al. Stroke statistics in Korea: part I. Epidemiology and risk factors: a report from the Korean Stroke Society and Clinical Research Center for stroke. J Stroke 2013;15:2-20.
16. Noser EA, Shaltoni HM, Hall CE, et al. Aggressive me- chanical clot disruption: a safe adjunct to thrombolytic therapy in acute stroke? Stroke 2005;36:292-296.
17. Higashida RT, Furlan AJ, Roberts H, et al. Trial design and reporting standards for intra-arterial cerebral thromboly- sis for acute ischemic stroke. Stroke 2003;34:e109-e137.
18. Kharitonova T, Mikulik R, Roine RO, et al. Association of early national institutes of health stroke scale improve- ment with vessel recanalization and functional outcome after intravenous thrombolysis in ischemic stroke. Stroke 2011;42:1638-1643.
19. Larrue V, von Kummer RR, Muller A, et al. Risk factors for severe hemorrhagic transformation in ischemic stroke pa- tients treated with recombinant tissue plasminogen acti- vator: a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II). Stroke 2001;32:438-441.
20. Michel P, Odier C, Rutgers M, et al. The Acute STroke Reg- istry and Analysis of Lausanne (ASTRAL): design and baseline analysis of an ischemic stroke registry including acute multimodal imaging. Stroke 2010;41:2491-2498.
21. Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke:
a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947.
22. Kidwell CS, Jahan R, Gornbein J, et al. A trial of imaging selection and endovascular treatment for ischemic stroke.
N Engl J Med 2013;368:914-923.
23. Ciccone A, Valvassori L, Nichelatti M, et al. Endovascular treatment for acute ischemic stroke. N Engl J Med 2013;
368:904-913.
24. Broderick JP, Palesch YY, Demchuk AM, et al. Endovas- cular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med 2013;368:893-903.
25. Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in acute cere- bral thromboembolism. JAMA 1999;282:2003-2011.
26. Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke 2007;38:967-973.