Received: October 1, 2013, Revised: November 8, 2013, Accepted: November 21, 2013 ISSN 1598-4478 (Print) / ISSN 2233-7679 (Online)
†
Correspondence to: Seong-Hwa Jeong
Faculty of Health Science, Daegu Haany University, 1, Haanydaero, Gyeongsan 712-715, Korea Tel: +82-53-819-1477, Fax: +82-53-819-1412, E-mail: [email protected]
Copyright © 2013 by the Korean Society of Dental Hygiene Science
Association of Oral Health Condition between Mothers and Their Preschool Children in Korea
Sae-Hee Cheon, Seong-Hwa Jeong 1†
Department of Dental Hygiene, Masan University, Changwon 630-729, 1 Faculty of Health Science, Daegu Haany University, Gyeongsan 712-715, Korea
어머니의 구강건강상태가 미취학 자녀의 구강건강상태에 미치는 영향
천세희ㆍ정성화
1†
마산대학교 치위생과,
1대구한의대학교 보건학부
The objective of this study was to examine whether there is an association of oral health conditions between mothers and their preschool children in Korea. A sample of 823 preschool children and their mothers were selected for this study from the database of the fourth Korean National Health and Nutrition examination Survey. Preschool children were defined as children aged 4, 5, and 6 years old. The subjects were clinically examined for the presence of caries lesions (dft index) and their mother was checked for the presence of dental caries (DMFT index) and periodontal status (CPI). The socio-demographic characteristics and mother’s oral health behaviours were considered covariates in this study. Univariate and multivariate analysis was adapted to assess the association of oral health condition between mothers and their preschool children. In univariate analysis, there were significant differences between preschool children’s dft index and their mother’s age (p=0.005), dental treatment demand for the past one year (p=0.034), and DMFT index (p=0.016). In multivariate analysis, only mother’s DMFT index was significantly associated with their children’s dft index after adjusting for covariates. In conclusion, the mother’s oral health was partly associated with their preschool children’s oral health in Korea.
Key Words: DMF index, Oral health, Preschool child
Introduction
Dental caries is a common oral disease, which is known as tooth decay. It affects a remarkable amount of preschool children
1)
. According to the Korea National Oral Health Survey, dental caries has shown to be a serious public oral health problem for preschool children in Korea2)
. The caries prevalence and decayed or filled teeth for deciduous teeth index (dft index) in 5-year- olds in 2010 were 61.5% and 2.99%, respectively. Althoughthe rates of dental caries have been decreasing in Korea, it is still high numerically when compared to other OECD countries, even in developed countries
3,4)
.Mothers who have poor oral health status may also have children that will have poor oral health when they grow up
5)
. Carter and Hill6)
showed that children’s likelihood of dental caries was determined by the amount of germs and bacteria in their mother’s mouth. Okada et al.7)
reported most mothers caring for their family at home are in an important and special position, while she has respon-sibility and the most central role for the maintenance and promotion of oral health. Nelson et al.
8)
investigated maternal factors such as their stress, coping, and social supports are significant predictors for adolescent caries.Borges et al.
9)
studied the influence of socio-behavioral factors on the prevalence and severity of dental caries in preschool children. In their conclusions, the dental caries in preschoolers was highly associated with factors related to the children’s parents. Saied- Moallemi et al.10)
reported the knowledge of the mother’s oral health affects posi- tively on their children cavities prevention. Goettems et al.11)
showed children’s oral conditions were related to their mothers dental anxiety, socioeconomic characteris- tics and maternal perception of their children’s oral health.Dye et al.
12)
investigated children’s oral health status is strongly related to their mother’s oral health status.There are numerous studies showing there is an associa- tion between mother’s oral health conditions and their children’s oral health status in other countries. Moreover, mother’s oral health behaviors, knowledge, and socio- demographic characteristics could be considered quite important predictor factors for children’s oral health.
However, there are still insufficient studies to verify the association of oral health condition between mothers and their children in Korea. Jeong et al.
13)
showed mother's education level have an effect on the prevalence of dental caries among preschool children using the Korea National Oral Health Survey 2006. Thus, it is meaningful to assess the association of oral health conditions between mothers and their children the using a national representative data.The aim of this study is to investigate the association of oral health condition between mothers and their preschool children in Korea.
Materials and Methods
1. Subjects
The data of this study was a subset of the fourth Korean National Health and Nutrition Examination Survey (KNHANES IV) which was conducted from 2007 to 2009 by the Korea Center for Disease Control and Prevention.
Preschool children were defined as children aged 4, 5, and 6 years old. The sample of preschool children were first
extracted from database of KNHANES IV. After then, their mothers information was matched independently using family identification variable in the database.
Finally, a total of 823 matched subjects were analyzed in this study.
2. Study variables
The preschool children’s and their mother’s oral health condition were evaluated dft index and decayed, missing, or filled teeth for permanent teeth index (DMFT index), res- pectively, which were based on the Korean National Oral Health Survey screening criteria. Periodontal status was also evaluated mother’s oral health condition using community periodontal index (CPI). The criterion for periodontal status was assessed by World Health Orga- nization CPI based on bleeding presence of calculus and, pocket depth at sextant of mouth
14)
. The CPI score was rated into 5 categories at each sextant: sound (CPI 0), gingival bleeding (CPI 1), calculus (CPI 2), shallow peri- odontal pocket of 3.5 to 5.5 mm (CPI 3), and deep peri- odontal pocket of 5.5 mm or more (CPI 4). Then the subject’s CPI score was considered the highest score of the sextant. According to the subject’s CPI score, periodontal status was classified the two groups: non- periodontitis (the highest CPI score of sextant ≤2) and periodontitis (the highest CPI score of sextant ≥3)15)
.The mother’s socio-demographic characteristics and oral health behaviors were considered covariates in this study.
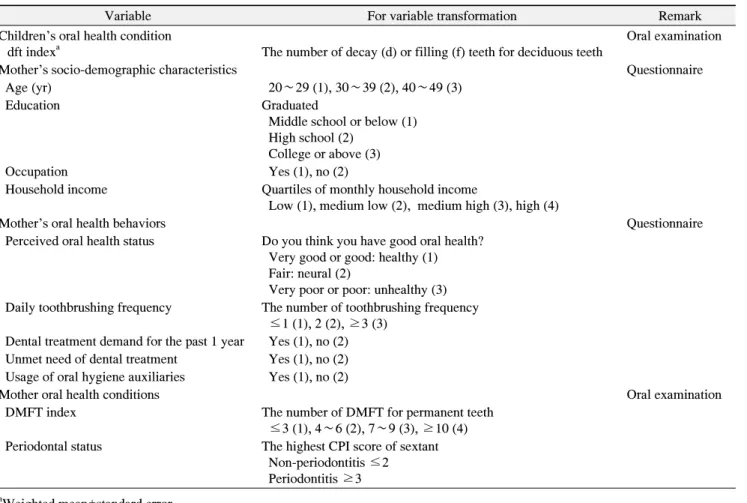
The mother’s socio-demographic characteristics included age, education, occupation, and household income. The mother’s oral health behaviors consisted of perceived oral health status, daily toothbrushing frequency, dental treat- ment demand for the past one year, unmet need of dental treatment, and usage of oral hygiene auxiliaries. Table 1 is summarized the classification of the variables in this study.
3. Statistical analysis
The children’s dft index according to the mother’s socio-demographic characteristics, and oral health be- haviors and conditions were summarized by mean and standard error, and then tested the mean differences by t-test or one-way ANOVA procedure. If there was a
Variable For variable transformation Remark Children’s oral health condition
dft index
aThe number of decay (d) or filling (f) teeth for deciduous teeth
Oral examination
Mother’s socio-demographic characteristics Questionnaire
Age (yr) 20∼29 (1), 30∼39 (2), 40∼49 (3)
Education Graduated
Middle school or below (1) High school (2)
College or above (3)
Occupation Yes (1), no (2)
Household income Quartiles of monthly household income
Low (1), medium low (2), medium high (3), high (4)
Mother’s oral health behaviors Questionnaire
Perceived oral health status Do you think you have good oral health?
Very good or good: healthy (1) Fair: neural (2)
Very poor or poor: unhealthy (3) Daily toothbrushing frequency The number of toothbrushing frequency
≤1 (1), 2 (2), ≥3 (3) Dental treatment demand for the past 1 year Yes (1), no (2) Unmet need of dental treatment Yes (1), no (2) Usage of oral hygiene auxiliaries Yes (1), no (2)
Mother oral health conditions Oral examination
DMFT index The number of DMFT for permanent teeth
≤3 (1), 4∼6 (2), 7∼9 (3), ≥10 (4) Periodontal status The highest CPI score of sextant
Non-periodontitis ≤2 Periodontitis ≥3
a
Weighted mean±standard error.
CPI: community periodontal index, dft: decayed or filled teeth for deciduous teeth, DMFT: decayed, missing, or filled teeth for permanent teeth.
Table 1. The Classification of the Study Variable
significant difference in one-way ANOVA, a subsequent post-hoc comparison was conducted using Scheffe’s method. Multiple regression analysis was adapted to assess the association of oral health condition between mothers and their preschool children after adjusting for covariates.
All analyses accounted a complex sampling design using SAS for Windows version 9.2 (SAS Institute Inc., Cary, NC, USA), and considered statistically significant as a p-value of <0.05.
Results
Table 2 showed mean differences of children’s dft index according to their mother’s socio-demographic character- istics, and oral health behaviors and conditions. The mean difference of dft index according to mother’s socio-demo-
graphic characteristics was statistically significant only in age (p=0.005). The mean dft index according to mother’s age was rated as 3.47, 2.43, and 3.91 in those 20 to 29, 30 to 39, and 40 to 49 years old, respectively. In subsequent post-hoc comparison, there was significant difference between the 30 to 39 years old group and the 40 to 49 years old group.
Among of mother’s oral health behaviors, the mean difference of children’s dft index was statistically signifi- cant with dental treatment demand for the past one year, but not in perceived oral health status, daily toothbrushing frequency, unmet need of dental treatment, and usage of oral hygiene auxiliaries. Mothers with dental treatment demand for the past one year (3.15) had statistically higher dft index of their children than that of the other group (2.49) (p=0.034).
Characteristic Number dft index
ap-value
bSocio-demographic
Age (yr) 0.005
20∼29 64 3.47±0.60
c,d30∼39 667 2.43±0.15
c40∼49 92 3.91±0.48
dEducation 0.684
Middle school or below 41 3.18±0.72
High school 426 2.72±0.18
College or above 356 2.58±0.21
Occupation 0.110
Yes 299 2.97±0.24
No 527 2.54±0.15
Household income 0.126
Low 43 3.56±0.59
Medium low 238 2.76±0.27
Medium high 324 2.41±0.20
High 218 2.87±0.22
Oral health behaviors
Perceived oral health status 0.565
Healthy 72 2.27±0.46
Neural 345 2.67±0.21
Unhealthy 406 2.78±0.20
Daily toothbrushing frequency 0.565
≤1 47 3.50±0.77
2 335 2.60±0.20
≥3 441 2.67±0.19
Dental treatment demand for the past 1 year 0.034
Yes 253 3.15±0.28
No 570 2.49±0.15
Unmet need of dental treatment 0.344
Yes 431 2.57±0.18
No 392 2.82±0.21
Usage of oral hygiene auxiliaries 0.902
Yes 375 2.67±0.20
No 448 2.71±0.20
Oral health condition
DMFT index 0.016
≤3 250 2.16±0.20
c4∼6 186 2.53±0.28
c,d7∼9 215 3.16±0.28
d≥10 172 3.05±0.31
dPeriodontal status 0.625
Periodontitis 125 2.86±0.39
Non-periodontitis 698 2.66±0.15
a
Weighted mean±standard error.
b
p-values were determined by t-test or one-way ANOVA.
c,d
The differentletter means that there are significant difference between two groups by Scheffe’s post-hoc test (p<0.05).
dft: decayed or filled teeth for deciduous teeth, DMFT: decayed, missing, or filled teeth for permanent teeth.
Table 2. Children’s dft Index according to Their Mother’s Socio-Demographic Characteristics, and Oral Health Behaviors and Conditions
Estimated coefficients (b) Standard error p-value Age (yr)
20∼29 Reference
30∼39 −1.136 0.609 0.063
40∼49 0.325 0.774 0.675
Education
Middle school or below Reference
High school 0.349 0.808 0.666
College or above 0.228 0.809 0.778
Occupation
Yes Reference
No 0.366 0.274 0.182
Household income
Low Reference
Medium low −0.613 0.606 0.312
Medium high −0.758 0.554 0.172
High −0.476 0.581 0.413
Perceived oral health status
Healthy Reference
Neural 0.321 0.503 0.524
Unhealthy 0.333 0.506 0.511
Daily toothbrushing frequency
≤1 Reference
2 −0.742 0.740 0.317
≥3 −0.754 0.749 0.315
Dental treatment demand for the past 1 year
No Reference
Yes 0.610 0.316 0.055
Unmet need of dental treatment
No Reference
Yes −0.252 0.261 0.334
Usage of oral hygiene auxiliaries
No Reference
Yes −0.136 0.282 0.629
DTMF index
≤3 Reference
4∼6 0.304 0.344 0.378
7∼9 0.894 0.341 0.009
≥10 0.727 0.368 0.049
Periodontal status
Non-periodontitis Reference
Periodontitis 0.064 0.409 0.877
DMFT: decayed, missing, and filled teeth.
Table 3. Association between Children’s Oral Health Conditions and Mother’s Socio-Demographic Characteristics, and Oral Health Behaviors and Conditions
In the mother’s oral health conditions, the mean dft index according to mother’s DMFT index were rated as 2.16, 2.53, 3.16, and 3.05 in those 3 or less, 4 to 6, 7 to 9 and 10 or more respectively, and there was a significant difference (p=0.016). In subsequent post-hoc comparison, the differences between the 3 or less group and the 7 to 9
group, and the 10 or more group were statistically signifi- cant respectively. On the other hand, the mean difference of children’s dft index was not statistically significant according to mother’s periodontal status.
Table 3 demonstrated an adjusted association between children’s oral health conditions and mother’s socio-
demographic characteristics, and oral health behaviors and conditions. After adjusted for other covariates, mother’s DMFT index was positively associated with their child- ren’s dft index. Mothers with 7 to 9 DMFT index were at increased dft index by 41.7% (b=0.894, p=0.009), and mothers with 10 or more DMFT index were at increased dft index by 33.7% (b=0.727, p=0.049), contrary to mothers with 3 or less DMFT index, respectively.
Discussion
General health status is determined by several factors rather than being determined by one variable. There are the individual’s life style, occupation, education, family structure, community, social, culture and environmental conditions in health determinants
16)
. Recently, numerical studies have proven that oral health affects ones general health, so that there is also the importance of maintaining health, teeth and gum conditions17,18)
. Parent’s environ- mental factors have a strong effect on their children’s oral health including dental diseases and oral health behaviors.In addition, patents with poor oral health condition might have their children that will suffer poor oral hygiene when they are adults, also could lead to the development of systemic problems such as hypertension, cardiovascular, diabetes and respiratory diseases
19)
.Chen
20)
showed the relationship between the mother’s oral health status, behaviors, knowledge and socio-demo- graphic factors, and dental caries status of their children.Specifically, they suggested the more mothers’ DMFT index have had, the more children’s dft index have as well.
Our findings as well showed the mother’s DMFT index was associated with their children’s oral health status after adjusting for all covariates.
Mattila et al.
21)
studied the prevalence of dental caries and its predictor in children, assessing children’s oral behaviors and their parents’ oral health conditions. The study reported parents should be promoted to develop their children’s oral health attitude and behaviors, moreover, parents’ oral health attitude and behaviors are incredibly important for their children. Poor oral health conditions in parents might turn over to their children. In particular, both genetic and environmental factors relatedto their oral health conditions may play a role in the onset of adult oral health conditions. Sankeshwari and Ankola
22)
investigated there was association of socio-demographic factors with children’s dental caries experience. In their suggestion, the findings could be valued to oral health education program for their parents. In our study, mother’s age was partly associated with childern’s dental caries.Wierzbicka et al.
23)
also reported children’s oral health habits are influenced by and the education level of their mother and the oral health care habits and Sayegh et al.24)
as well explained that social class and income level of parents are inversely proportional to their children caries experience. On the other hand, our study showed that the mother’s education level and household income was not persuaded by any of their children’s oral health status, but there were decreasing tendency as more education and higher income.There were a few limitations even this study demon- strated that children’s dental caries experience was signifi- cantly associated with the mother’s dental caries using national representative data. Firstly, our study is designed to the cross-sectional study, which is impossible to verify the causality between children’s oral health status and their mother’s oral health conditions. Secondly, our study did not reflect all confounded variables between mother’s and children’s oral health conditions, because we con- ducted the secondary data analysis using database of KNHANES IV.
Summary
This study was to examine whether there is an association of oral health conditions between preschool children and their mothers using the KNHANES IV in Korea. A sample of 823 preschool children and their mothers were selected for this study using the family identification variable in the database of the KNHANES.
Statistical analysis was carried out considering the weights to reflect the complex sampling design. The mean differences of children’s dft index according to the mother’s socio-demographic characteristics, mother’s oral health behaviors and conditions were performed, multiple regression analysis was conducted to assess the associ-
ation of oral health condition between mothers and their preschool children. In the results, the mean difference of dft index according to mother’s socio-demographic cha- racteristics was statistically significant in age (p=0.005), the mean difference of children’s dft index among of mother’s oral health behaviors was statistically significant with dental treatment demand for the past one year (p=0.034). In addition, the mean difference of the mother’s DMFT index according to children’s dft index was statistically significant (p=0.016). Meanwhile, after adjusted for the mother’s socio-demographic charac- teristics and oral health behaviors, the mother’s DMFT index positively associated with their children’s dft index.
Therefore this study found the better mother’s oral health condition improves their children’s oral health condition.
These findings of this study suggest mother’s oral health condition may have an effect on their children’s oral health, and oral health education program to improve mother’s oral health condition should be developed.
요 약
본 연구는 국민건강영양조사 제4기 자료를 이용하여 미 취학 아동의 치아우식상태와 어머니 구강건강상태와의 관 련성을 파악하고자 하였다. 원시자료에서 가족 아이디 변수 를 이용해 아동과 어머니를 짝짓기하여 최종 823명의 자료 를 추출하였다. 통계분석은 복합표본설계를 반영하기 위하 여 가중치를 고려한 분석을 실시하였으며, 어머니의 인구사 회학적 특성과 구강건강행태 및 구강건강상태에 따른 자녀 의 우식경험유치지수의 차이를 분석하고, 이들 간의 관련성 을 알아보기 위해 다중회귀분석을 시행하였다. 분석결과, 미취학 아동의 우식경험유치지수는 어머니의 사회인구학 적 특성 중 나이에 따른 차이가 통계적으로 유의하였으며 (p=0.005), 어머니의 구강건강행태 중 지난 1년 동안 치과 검진 유무에 따른 차이가 통계적으로 유의하였다(p=0.034).
또한 어머니의 우식경험영구치지수에 따른 자녀의 우식경 험유치지수의 차이도 통계적으로 유의하였다(p=0.016). 한 편 어머니의 인구사회학적 특성과 구강건강행태를 보정한 후, 어머니와 자녀의 구강건강상태 관련성을 분석한 결과 어머니의 우식경험영구치지수는 자녀의 우식경험유치지수 와 유의한 관련성이 있는 것으로 나타났다. 따라서 어머니 의 구강건강상태가 양호할수록 자녀의 구강건강상태 또한 양호함을 알 수 있었다. 이러한 연구 결과는 어머니의 구강
건강상태가 자녀들에게 영향을 미칠 수 있음을 보여주므로 어머니들의 구강건강상태를 향상시킬 수 있는 효과적인 구 강보건교육 프로그램이 개발되어야 한다고 생각된다.