□Case Report□
217 Disruption of the urinary collecting system can produce internalized urine leaks that can form an encapsulated collection of urine, which is known as a urinoma.1 Urinomas are an uncommon condition and are usually the result of renal trauma, but may be the result of obstructive uropathy from a urteral stone or a pelvic mass or even a urological procedure. Phy- siologic dilatation of the urinary tract by hormonal influences and of course, mechanical effects are universally associated with pregnancy. However, a rupture of the urinary collection system is rare. This report describes a case of extremely large urinomas of both retroperitoneal spaces that was detected during the postpartum period.
CASE REPORT
A 31-year-old woman presented with the chief complaint of bilateral flank pain. The patient gave birth one month before by Cesarean section because of dystocia. There was no history of prior trauma or stones and no documented urinary tract infection during her pregnancy. The postpartum physical examination was unremarkable except for mild tenderness in both flanks. There was no history of lower urinary tract symptom. Urinalysis yielded normal results and the urine
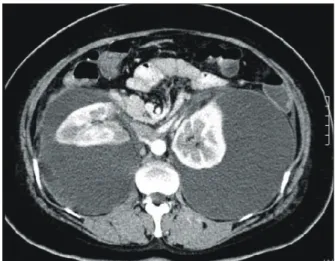
culture results were also negative. Serum creatinine level was 1.2mg/dl. Abdominal ultrasonography revealed huge echo-poor collections around both kidneys. Abdominal CT scan showed poor attenuation with a large amount of fluid collection around both shrunken kidneys and no extravasation of contrast media (Fig. 1). However, there was no evidence of hydronephro- ureterosis. Percutaneous drainage was immediately performed.
Huge Perirenal Urinomas in a Woman during the Postpartum Period
Se Jung Jang, Dong Il Kang
From the Department of Urology, Inje University College of Medicine, Busan, Korea
Urinary tract dilation is one of the most common side effects during pregnancy. This is primarily a physiologic phenomenon that is typically more prominent on the right side, and it is caused by hormonal changes and mechanical obstruction. Occasionally, urinary tract dilation leads to more serious urinary tract problems such as infection, obstructive renal failure and urinomas. Urinomas are also known as pararenal pseudocysts, and they generally occur as a result of urinary system disruption, but they only rarely occur with pregnancy. We report here on an unusual case of extremely large bilateral perirenal urinomas that were detected during the postpartum period. This was successfully resolved by percutaneous drain- age and ureteral stents. (Korean J Urol 2006;47:217-219)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Hydronephrosis, Pregnancy, Postpartum period
대한비뇨기과학회지 제 47 권 제 2 호 2006
인제대학교 의과대학 비뇨기과학교실 장세정․강동일
접수일자:2005년 10월 7일 채택일자:2005년 11월 24일 교신저자: 강동일
인제대학교 의과대학 부산백병원 비뇨기과 부산시 부산진구 개금동 633-165번지
ꂕ 614-735 TEL: 051-890-6384 FAX: 051-892-9887 E-mail: urokang@
lycos.co.kr
Fig. 1. Abdominal computed tomography (CT) scan shows a large fluid collection around both kidneys. The kidneys are shrunken.
218
대한비뇨기과학회지:제 47 권 제 2 호 2006
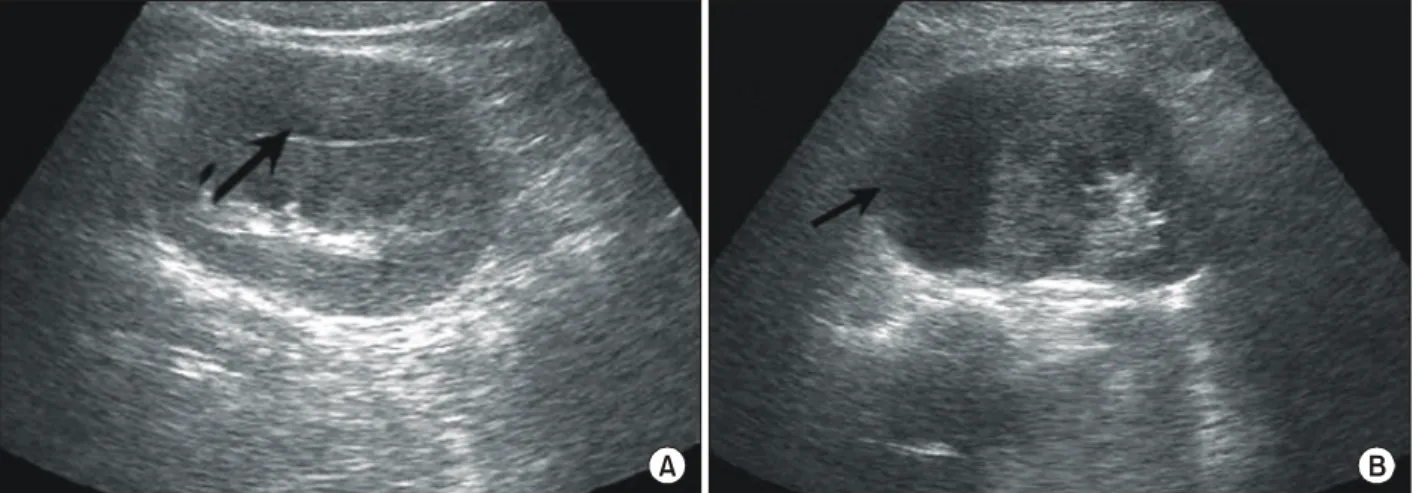
Approximately 1,200ml and 800ml of amber-colored fluid was drained from the right and left side, respectively. After four days, ultrasonography indicated that the urinomas had resolved, and there was no longer any urine leakage via the drainage catheters, which were consequently removed. However, six weeks later, bilateral flank pain and the urinomas redeveloped (Fig. 2). Once again, percutaneous drainage catheters and ureteral stents were established, but left in place for one month.
Complete reabsorption of the perinephric urinomas was ob- served by using ultrasonography and the percutaneous drainage catheters and ureteral stents were removed. Five months later, we concluded, with the use of ultrasonography, no relapse of bilateral perinephric urinoma (Fig. 3).
DISCUSSION
Hydronephrosis during pregnancy is quite common and is often associated with mechanical obstruction of the ureters at the pelvic brim.2 Although this is present in over 80 percent of pregnant woman, the normal ureter and bladder anatomy is usually restored to normal within several weeks postpartum.3 Usually, the right ureter is much more affected than the left ureter, which is somewhat protected by the sigmoid colon and its mesentery.3
Clinical presentations of hydronephrosis are flank pain and tenderness associated with gastointestinal distress. These symptoms are similar to those of other obstetric and surgical emergencies such as acute appendicitis, cholecystitis, nephroli- Fig. 2. Ultrasound indicates anechoic areas (black arrows) that are newly developed around both kidneys (A: right kidney, B: left kidney).
A B
Fig. 3. Ultrasonography shows complete reabsorption of perinephric urinomas after 5 months (A: right kidney, B: left kidney).
A B
Se Jung Jang, et al:Huge Perirenal Urinoma in Women during the Postpartum Period
219thiasis and/or acute hydramnios.4 Occasionally, increasing hy- dronephrosis can proceed to retroperitoneal urinary extravasa- tion and urinoma formation. Such complications may lead to a perinephric abscess, peripelvic urinary granuloma, or retrop- eritoneal fibrosis.5,6 Reports of bilateral perinephric urinomas in connection with pregnancy are very rare in the literature.
Prompt diagnosis and management of urinary extravasation is very important and urgently requires measures to prevent such complications. Ultrasonography is indispensable for diagnosis, and CT scanning may also aid in the diagnosis.7,8
A perinephric urinoma appears on sonography as a homo- geneous collection of anechoic fluid. The treatment of a urinoma depends on the urinary extravasation cause and the degree to which the functioning of the kidney is affected. The treatment goals are to preserve renal function, relieve pain, and allow the site of rupture to heal.9 In most cases, small urinomas will reabsorb without intervention. If urinomas are large or persist for several days, drainage of the urinoma should be considered. If a urinoma does not diminish despite an ade- quately positioned percutaneous drainage catheter, decom- pression of the pelvocaliceal system must be taken in order to prevent a continuous urinoma enlargement.8
In conclusion, urinomas should be a consideration for women with postpartum flank pain, and it is necessary to diagnose
quickly and treat appropriately in order to preserve renal function.
REFERENCES
1. Arnold EP. Pararenal pseudocyst. Br J Urol 1972;44:40-6 2. Roberts JA. Hydronephrosis of pregnancy. Urology 1976;8:1-4 3. Dhabuwala CB, Riehle RA Jr. Spontaneous rupture of a hy- dronephrotic kidney during pregnancy. Urology 1984;24:591-4 4. Anteby SD, Ron M, Diamant YZ. Hydroureter and hydro- nephrosis of pregnancy presenting as acute obstetric or surgical emergencies. Int Surg 1975;60:93-5
5. Kinn AC. Complicated hydronephrosis of pregnancy. Acta Obstet Gynecol Scand 1981;60:91-5
6. Hamperl H, Dallenbach FD. The extravasation and precipi- tation of urine in the hilus of the kidneys. J Mt Sinai Hosp N Y 1957;24:929-34
7. Hamoud K, Kaneti J, Smailowitz Z, Kroll D, Barki Y. Spon- taneous perinephric urinoma in pregnancy. Int Urol Nephrol 1994;26:643-6
8. Titton RL, Gervais DA, Hahn PF, Harisinghani MG, Arellano RS, Mueller PR. Urine leaks and urinomas: diagnosis and imaging-guided intervention. Radiographics 2003;23:1133-47 9. Royburt M, Peled Y, Kaplan B, Hod M, Friedman S, Ovadia
J. Non-traumatic rupture of kidney in pregnancy - case report and review. Acta Obstet Gynecol Scand 1994;73:663-5