*This work was supported by Korea Institute of Planning and Evaluation for Technology in Food, Agriculture, Forestry(IPET) through Agri-Bio industry Technology Development Program, funded by Ministry of Agriculture, Food and Rural Affairs(MAFRA) from 2016 to 2017(316086-2).
*Corrensponding Author : Jeong-Yi Kwon (jeongyi.kwon@samsung,com) Received January 24, 2018
Accepted May 20, 2018
Revised April 30, 2018 Published May 28, 2018
소아청소년을 대상으로 한 재활승마 선별도구 : 델파이 방법을 통한 융합연구
황영섭1, 장현정2, 홍보영3, 이지영4, 권정이1*
1
삼성서울병원 재활의학과,
2삼성창원병원 재활의학과,
3
가톨릭대학교 성빈센트병원 재활의학과,
4삼성전자 승마단
The Screening Tool for Equine Assisted Activities and Therapies in Children and Adolescents : A Convergence Study with the Delphi Method
Young Sub Hwang 1 , Hyun Jung Chang 2 , Bo Young Hong 3 , Ji Young Lee 4 , Jeong-Yi Kwon 1*
1
Dept. of Physical and Rehabilitation Medicine, Sungkyunkwan University School of Medicine, Samsung Medical Center,
2
Dept. of Physical and Rehabilitation Medicine, Sungkyunkwan University School of Medicine, Samsung Changwon Hospital,
3
Dept. of Rehabilitation Medicine, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea,
4
Samsung Equestrian Team
요 약 본 연구의 목적은 국내 소아청소년을 대상으로 한 재활승마 선별도구를 개발하는 것으로, 승마장에서 재활승마지도사 들이 참가자를 직접 선별 가능하도록 하기 위함이다. 예비 선별도구는 6명의 전문가가 기존 국외의 지침서들을 참조하여 개발 하였으며 해당 인원이 포함된 총 23명의 전문가들을 대상으로 두 차례의 델파이 연구를 진행하였다. 선별도구 각 항목의 적절 성에 대한 의견을 0점(비동의)~10점(동의)으로 총 11점 척도로 표시하도록 하였다. 항목의 적절성이 8점 이상인 경우를 합의 된 항목으로 간주하였으며 8점 이상인 항목은 48개의 항목 중 39개의 항목이었다. 39 항목의 켄달의 일치계수에서 유의미한 결과값이 나타나(p<.001) 평가자간 의견일치가 되었음을 확인하였으며 따라서 최종 선별도구는 총 39개의 항목으로 구성되었 다. 재활승마 선별도구는 참가자에게 보다 더 안전한 재활승마를 제공할 것이며 향후 성인을 대상으로 한 추가적인 연구가 필요할 것으로 보인다.
주제어 : 재활승마, 소아청소년, 재활승마지도사, 선별도구, 델파이연구
Abstract
The aim of this study was to develop the Equine Assisted Activities and Therapies(EAAT) screening tool for children and adolescents, which can be available for the EAAT instructors to screen potential participants in the riding center. The preliminary screening tool was developed by six experts and several international guidelines were used for the references. A two-round Delphi study was performed with 23 experts. Panel members were asked to rate their (dis)agreement with each tool’s item on an 11-point scale. The consensus was considered to be reached when the item was scored more than 8. The consensus was reached on 39 items out of 48, resulting the final screening tool’s items are to be 39. The resulting screening tool could contribute to make safer EAAT settings for participants and the future investigations in adult subjects will be needed.Key Words :
EAAT, Adolescents, Screening tool, EAAT instructor, Delphi study1. 서론
재활승마(Equine Assisted Activities and Therapies;
EAAT)란 신체적 정신적 장애를 가진 사람이 승마를 통 하여 치료적 성과를 도모하는 말을 이용한 재활프로그램 이다. 재활승마의 목표로는 균형감각 및 자세조절의 향 상, 대근육 및 소근육 운동기술 발달, 집중력 향상, 의사 소통 능력의 향상 등이 있다[1-3].
하지만 재활승마를 시행하기에 앞서 해당 활동의 위 험요소 또한 존재한다는 점을 간과 할 수 없다. 승마활동 중 부상으로 인한 입원시간 비율이 모터사이클로 인한 입원시간 비율보다 3배 이상 많았다는 연구 결과가 있으 며[4], 약 500kg정도의 무게로 시속 65km로 달릴 수 있는 말의 특성을 고려한다면[5] 위험성이 존재하는 것은 당 연하다. 아동이 승마활동 중 발생하는 사고의 종류로는 낙상이 52%로 가장 빈번하게 일어났으며 낙상 후 이차 적으로 말굽에 치이거나 밟히고 깔리는 상황으로 이어질 가능성 또한 크다[6]. 승마활동으로 인한 부상의 종류로 는 골절, 두부손상, 열상, 연조직 손상 등이 있으며[7] 부 상 빈도가 가장 많은 신체부위는 머리이다[6]. 머리의 부 상은 어떤 신체부위의 부상보다도 오랜 기간 동안의 장 애를 남기는 부위로, 승마활동 중 부상으로 외상성 뇌손 상을 진단받은 생존자 106명 중 63%가 의식이 떨어짐을 경험하였고 46%가 외상후 기억상실증을 겪었으며 13%
가 퇴원 후에도 지속적인 신경학적 후유증을 겪었을 정 도로[8] 부상의 심각성 큰 편이다. 따라서 재활승마지도 사는 안전한 재활승마를 시행하기 위하여 승마 참가자의 금기증, 건강상태와 같은 제한점들을 명확하게 알고 있 어야 한다.
그러나 불행하게도 비의료인인 재활승마지도사들이 이러한 결정을 내리기에는 정보가 부족하여 위험을 감수 하고 기승활동에 참여시키거나 의료진의 소견서를 첨부 하도록 요구한다. 기승 활동 전에 미주에서와 같이 모든 참가자들이 의사의 전문 진료를 받는 것은 바람직하나, 진료를 의뢰받은 의사들이 재활승마에 대한 지식이 부족 하다면 기승을 허락하지 않을 가능성이 높다. 그 결과 참 가자들은 재활승마에 참여할 기회가 오히려 박탈된다.
지도사들이 안전하게 재활승마를 실시 할 수 있도록 국제 재활승마협회(Professional Association of Therapeutic Horsemanship International; PATH Intl.)의 기준 매뉴얼 (standard manual)에서[9] 재활승마의 금기증을 정하고
있다. 하지만 이는 성인기의 모든 질환까지 포함하고 있 어 소아청소년을 주 대상으로 하는 국내의 대부분의 승 마장에서 적용하기에는 부적합한 측면이 있다. 또한 비 의료인인 재활승마지도사들이 50여 페이지의 의학용어 가 포함된 영문 매뉴얼의 내용을 모두 숙지하여 적용하 기에는 어려움이 있다.
앞선 요인들로 현재 국내 승마장에서 재활승마를 시 행 시, 특별한 선별 절차 없이 지도사가 강습을 진행하고 있는 경우가 대부분이다. 따라서 효율적이고 안전한 재 활승마 체계의 발전을 위하여, 국내 현실에 적합한 ‘소아 청소년을 대상으로 한 재활승마 선별도구’를 개발하고자 한다.
2. 재료 및 방법
2.1 연구방법
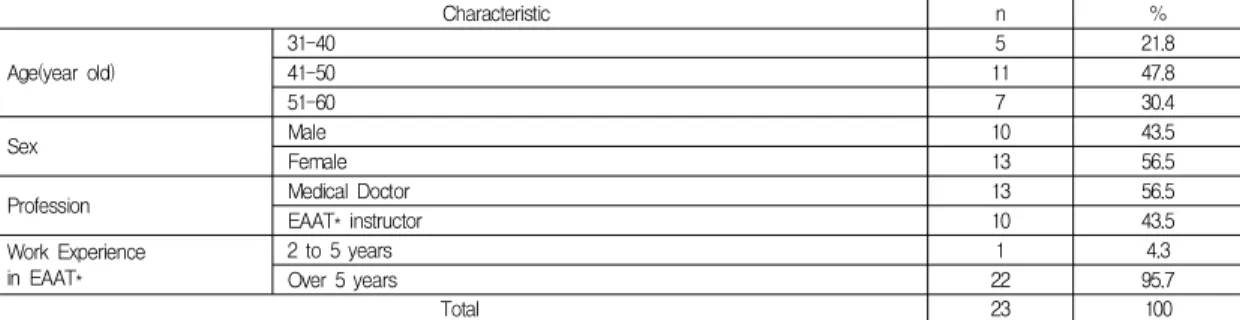
본 연구는 정확한 지식이 없는 문제에 대해 여러 전 문가 인원들로부터 의견을 종합하는 델파이 기법(Delphi study)을 적용하였다[10]. 전문가 모집 기준은 목적적 표 집을 이용하여 재활승마지도사 자격증이 있으며 재활승 마 경력이 5년 이상인 자, 혹은 전문의 자격증을 소지한 의사의 경우 재활승마 경력이 2년 이상인 자로 설정하였 다. 앞선 참여자 선정 기준을 충족시키는 인원을 각 분야 로부터 추천을 받아 참여 의사를 이메일 혹은 전화로 사 전에 확인하고 동의를 얻어 전문가 총 23명을 선정하였 다. Table 1
연구진은 대상 소아청소년의 선별에 필요한 항목들을 전문가들과의 합의 하에 도출하여 설문 항목을 구성하였 으며, 해당 1차 설문지를 대면방식 혹은 이메일을 통해 전문가들에게 전달 후 회신 받아 항목들의 적절성 및 설 문지에 대한 의견를 확인 하였다. 이후 해당 결과를 바탕 으로 설문지 구성 및 항목의 내용들을 수정하여 2차 설문 지를 작성하였다. 완성된 설문지 또한 대면방식 혹은 이 메일을 통해 전문가들에게 전달한 후 회신 받아 항목들 의 적절성을 다시 한 번 재평가 받았으며 연구진은 해당 설문지 결과를 바탕으로 최종 재활승마 선별도구를 작성 하였다.
2.2 델파이 조사 설문지
본 연구는 개방형 질문형식을 생략하고, 1차 델파이
Characteristic n %
Age(year old)
31-40 5 21.8
41-50 11 47.8
51-60 7 30.4
Sex Male 10 43.5
Female 13 56.5
Profession Medical Doctor 13 56.5
EAAT* instructor 10 43.5
Work Experience in EAAT*
2 to 5 years 1 4.3
Over 5 years 22 95.7
Total 23 100
EAAT*: Equine Assisted Activities and Therapies
Table 1. Backgrounds of participants in the delphi study(n=23)
조사 이전에 연구진 (전문의 3명, 재활승마지도사 3명) 이 국제재활승마협회의 기준 매뉴얼과 영국 장애인 승마 협회(The Riding For The Disabled Association;RDA)의 영국 장애인 승마협회 강사/코치를 위한 지도서: 승마에 있어서의 금기증(Guidance for RDA Groups and Instructors/Coaches: Contra-indications for riding)을 [11]<Appendix 2> 기초로 소아청소년을 대상으로 재활 승마를 시행하기 전 선별에 필요한 항목들을 합의 하에 도출하여 설문 항목을 구성하였다. 전문가들의 합의에 의해 도출 되어 만들어진 1차 설문지의 구성은 세 영역 1) 재활승마를 시행 할 수 있는 기본 조건, 2) 주의 사항 (기승 전 의사로부터 전문 소견을 필요로 하는 경우), 3) 금기 사항으로 이루어졌다. 설문지는 응답 항목의 각각 의 중요도를 0점에서 10점까지의 11점 척도 (전혀 중요 하지 않다=0, 매우 중요하다=10)에 표시하도록 구성이 되었다. 2차 설문지는 1차 조사 결과의 항목별 평균, 표준 편차, 사분위수 범위가 포함되어 패널들의 각 항목에 대 한 합의도를 반영하여 작성 할 수 있도록 구성 되었다. 2 차 델파이 조사에서는 전문가 의견의 우선순위와 항목별 중요도에 대한 델파이 전문가들의 의견 일치도를 확인하 기 위하여 켄달의 일치계수 (Kendall's Coefficient of Concor-dance; W)를 사용하였으며 통계적으로 유의한 경우 평가자들의 의견이 상호간에 일치된 것으로 해석 할 수 있다.
2.3 자료 분석
수집된 자료는 SPSS Win 20.0 프로그램을 통해 분석 하였으며, 1차 전문가 델파이 조사 응답 분석에서는 세 가지 영역의 각 항목별 평균, 최소값, 최대값, 표준편차, 사분범위를 제시하기 위해 기술 통계 분석을 실시하였다.
2차 델파이 조사 응답 분석에서는 전문가 의견의 우선순
위와 항목별 중요도에 대한 델파이 전문가들의 의견 일 치도를 확인하기 위하여 켄달의 일치계수(Kendall's Coefficient of Concordance;W)를 사용하였으며 통계적 으로 유의한 경우 평가자들의 의견이 상호간에 일치된 것으로 해석 된다. 또한 2차 델파이 조사에서도 기술 통 계를 사용하여 선정된 각 항목의 적절성을 재평가하기 위하여 해당 값의 평균과 표준편차를 분석하였다.
3. 결과
3.1 연구 대상자의 특성
델파이 패널 23인 중 남성은 10명(43.5%), 여성은 13 명(56.5%)이었다. 연령별 분포는 30대가 5명(21.8%), 40 대가 11명(47.8%), 50대가 7명(30.4%)이었다, 직종에서는 의사가 13명(56.5%)으로 재활의학과 의사 10명과 정신건 강의학과 의사 3명으로 구성 되었으며 재활승마지도사는 총 10명(43.5%) 으로 재활승마지도사 중 물리치료사 자 격 동시 소지자는 3명, 작업치료사 자격 동시 소지자는 1 명 이었다. 재활승마경력은 대부분 5년 이상(95.7%) 이었 다. Table 1
3.2 전문가 델파이 조사결과
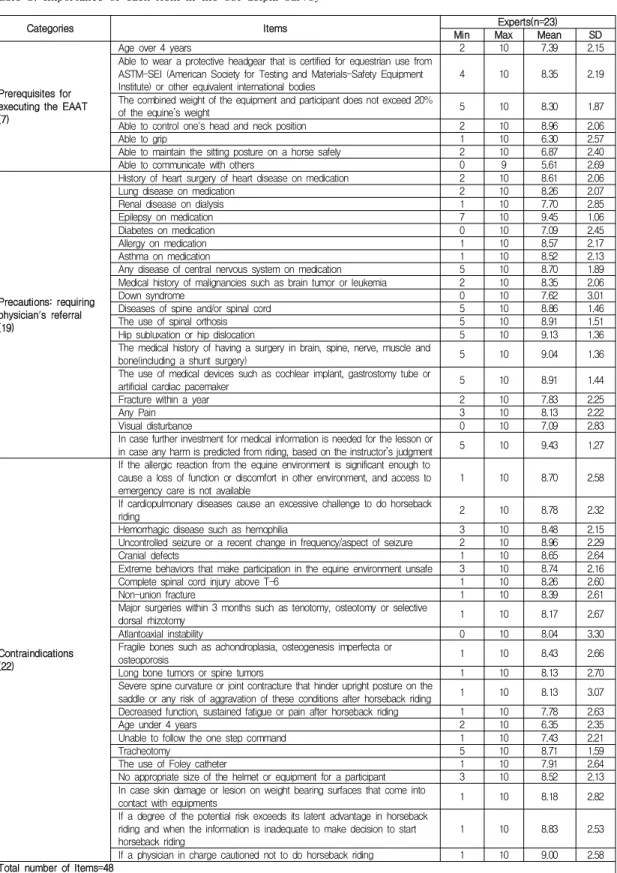
3.2.1 1차 델파이 조사결과 Table 2
1차 델파이 조사결과에서 각 항목들에 대한 평균, 표 준편차, 사분위수 범위가 구해졌으며 설문지 구성 및 내 용에 대한 의견들을 수렴하였다. 의견 내용들 중 타당한 근거가 있다고 판단되는 의견들을 선별하여 그에 따라 설문지 내용을 수정하였다. 재활승마를 시행 할 수 있는 기본 조건에 대한 영역에서 ‘쥐기 가능’ 항목과 ‘의사소통 가능’항목은 설명이 구체적이지 못하다는 의견에 따라
Categories Items Experts(n=23)
Min Max Mean SD
Prerequisites for executing the EAAT (7)
Age over 4 years 2 10 7.39 2.15
Able to wear a protective headgear that is certified for equestrian use from ASTM-SEI (American Society for Testing and Materials-Safety Equipment Institute) or other equivalent international bodies
4 10 8.35 2.19
The combined weight of the equipment and participant does not exceed 20%
of the equine’s weight 5 10 8.30 1.87
Able to control one's head and neck position 2 10 8.96 2.06
Able to grip 1 10 6.30 2.57
Able to maintain the sitting posture on a horse safely 2 10 6.87 2.40
Able to communicate with others 0 9 5.61 2.69
Precautions: requiring physician's referral (19)
History of heart surgery of heart disease on medication 2 10 8.61 2.06
Lung disease on medication 2 10 8.26 2.07
Renal disease on dialysis 1 10 7.70 2.85
Epilepsy on medication 7 10 9.45 1.06
Diabetes on medication 0 10 7.09 2.45
Allergy on medication 1 10 8.57 2.17
Asthma on medication 1 10 8.52 2.13
Any disease of central nervous system on medication 5 10 8.70 1.89
Medical history of malignancies such as brain tumor or leukemia 2 10 8.35 2.06
Down syndrome 0 10 7.62 3.01
Diseases of spine and/or spinal cord 5 10 8.86 1.46
The use of spinal orthosis 5 10 8.91 1.51
Hip subluxation or hip dislocation 5 10 9.13 1.36
The medical history of having a surgery in brain, spine, nerve, muscle and
bone(including a shunt surgery) 5 10 9.04 1.36
The use of medical devices such as cochlear implant, gastrostomy tube or
artificial cardiac pacemaker 5 10 8.91 1.44
Fracture within a year 2 10 7.83 2.25
Any Pain 3 10 8.13 2.22
Visual disturbance 0 10 7.09 2.83
In case further investment for medical information is needed for the lesson or
in case any harm is predicted from riding, based on the instructor’s judgment 5 10 9.43 1.27
Contraindications (22)
If the allergic reaction from the equine environment is significant enough to cause a loss of function or discomfort in other environment, and access to emergency care is not available
1 10 8.70 2.58
If cardiopulmonary diseases cause an excessive challenge to do horseback
riding 2 10 8.78 2.32
Hemorrhagic disease such as hemophilia 3 10 8.48 2.15
Uncontrolled seizure or a recent change in frequency/aspect of seizure 2 10 8.96 2.29
Cranial defects 1 10 8.65 2.64
Extreme behaviors that make participation in the equine environment unsafe 3 10 8.74 2.16
Complete spinal cord injury above T-6 1 10 8.26 2.60
Non-union fracture 1 10 8.39 2.61
Major surgeries within 3 months such as tenotomy, osteotomy or selective
dorsal rhizotomy 1 10 8.17 2.67
Atlantoaxial instability 0 10 8.04 3.30
Fragile bones such as achondroplasia, osteogenesis imperfecta or
osteoporosis 1 10 8.43 2.66
Long bone tumors or spine tumors 1 10 8.13 2.70
Severe spine curvature or joint contracture that hinder upright posture on the
saddle or any risk of aggravation of these conditions after horseback riding 1 10 8.13 3.07 Decreased function, sustained fatigue or pain after horseback riding 1 10 7.78 2.63
Age under 4 years 2 10 6.35 2.35
Unable to follow the one step command 1 10 7.43 2.21
Tracheotomy 5 10 8.71 1.59
The use of Foley catheter 1 10 7.91 2.64
No appropriate size of the helmet or equipment for a participant 3 10 8.52 2.13 In case skin damage or lesion on weight bearing surfaces that come into
contact with equipments 1 10 8.18 2.82
If a degree of the potential risk exceeds its latent advantage in horseback riding and when the information is inadequate to make decision to start horseback riding
1 10 8.83 2.53
If a physician in charge cautioned not to do horseback riding 1 10 9.00 2.58 Total number of Items=48
Table 2. Importance of each item in the 1st delphi survey
Categories Items Experts(n=23)
Min Max Mean SD Kendall’s W
Prerequisites for executing the EAAT (7)
Age over 4 years 5 10 7.87 1.42
W= 0.46 χ2 = 63.50
d.f. = 6 p<.001 Able to wear a protective headgear that is certified for
equestrian use from ASTM-SEI (American Society for Testing and Materials-Safety Equipment Institute) or other equivalent international bodies
6 10 8.78 1.31
The combined weight of the equipment and participant does
not exceed 20% of the equine’s weight 5 10 8.17 1.59
Able to control one's head and neck position 6 10 9.17 1.15 Able to grip(※It is usual for participants to grip rein or saddle in THR) 0 10 6.26 2.60 Able to maintain the sitting posture on a horse safely 2 10 7.00 2.00 Able to communicate with others(※possible to follow the one
step command) 0 9 5.74 2.63
Precautions: requiring physician's referral (19)
History of heart surgery or heart disease on medication or 7 10 8.96 1.11
W= 0.25 χ2 = 105.91
d.f. = 18 p<.001
Lung disease on medication 7 10 8.74 1.10
Renal disease on dialysis 3 10 8.17 1.99
Epilepsy on medication 8 10 9.57 0.79
Diabetes on medication 0 10 7.30 2.25
Allergy on medication 5 10 8.78 1.45
Asthma on medication 5 10 8.91 1.44
Any disease of central nervous system on medication 5 10 8.96 1.46 Medical history of malignancies such as brain tumor or leukemia 0 10 8.35 2.10
Down syndrome 3 10 8.43 1.78
Diseases of spine and/or spinal cord 8 10 9.00 0.91
The use of spinal orthosis 7 10 9.30 1.02
Hip subluxation or hip dislocation 7 10 9.48 0.85
The medical history of having a surgery in brain, spine,
nerve, muscle and bone(including a shunt surgery) 7 10 9.39 0.89 The use of medical devices such as cochlear implant,
gastrostomy tube or artificial cardiac pacemaker 8 10 9.26 0.81
Fracture within a year 0 10 8.09 2.17
Any Pain 0 10 8.00 2.47
Visual disturbance 0 10 7.35 2.84
In case further investment for medical information is needed for the lesson or in case any harm is predicted from riding, based on the instructor’s judgment
8 10 9.78 0.60
Contraindications (22)
If the allergic reaction from the equine environment is significant enough to cause a loss of function or discomfort in other environment, and access to emergency care is not available
1 10 8.70 2.58
W= 0.26 χ2 = 126.24
d.f. = 21 p<.001 If cardiopulmonary diseases cause an excessive challenge to
do horseback riding 8 10 9.52 0.79
Hemorrhagic disease such as hemophilia 8 10 9.17 0.94
Uncontrolled seizure or a recent change in frequency/aspect
of seizure 8 10 9.61 0.66
Cranial defects 8 10 9.43 0.73
Extreme behaviors that make participation in the equine
environment unsafe 6 10 9.35 1.11
Complete spinal cord injury above T-6 8 10 9.13 0.92
Non-union fracture 7 10 9.22 1.00
Major surgeries within 3 months such as tenotomy,
osteotomy or selective dorsal rhizotomy 6 10 9.00 1.21
Atlantoaxial instability 7 10 9.26 1.10
Fragile bones such as achondroplasia, osteogenesis
imperfecta or osteoporosis 8 10 9.22 0.90
Long bone tumors or spine tumors 5 10 8.96 1.30
Severe spine curvature or joint contracture that hinder upright posture on the saddle or any risk of aggravation of these conditions after horseback riding
1 10 8.96 2.01
Decreased function, sustained fatigue or pain after horseback riding 5 10 8.35 1.67
Age under 4 years 2 10 7.00 2.07
Unable to follow the one step command 0 9 6.96 2.40
The use of T-cannula 6 10 8.83 1.30
The use of Foley catheter 6 10 8.74 1.21
No appropriate size of the helmet or equipment for a participant 7 10 9.26 0.96 In case skin damage or lesion on weight bearing surfaces
that come into contact with equipments 6 10 9.17 1.15
If a degree of the potential risk exceeds its latent advantage in horseback riding and when the information is inadequate to make decision to start horseback riding
8 10 9.57 0.59
If a physician in charge cautioned not to do horseback riding 8 10 9.74 0.54 Total number of Items=48
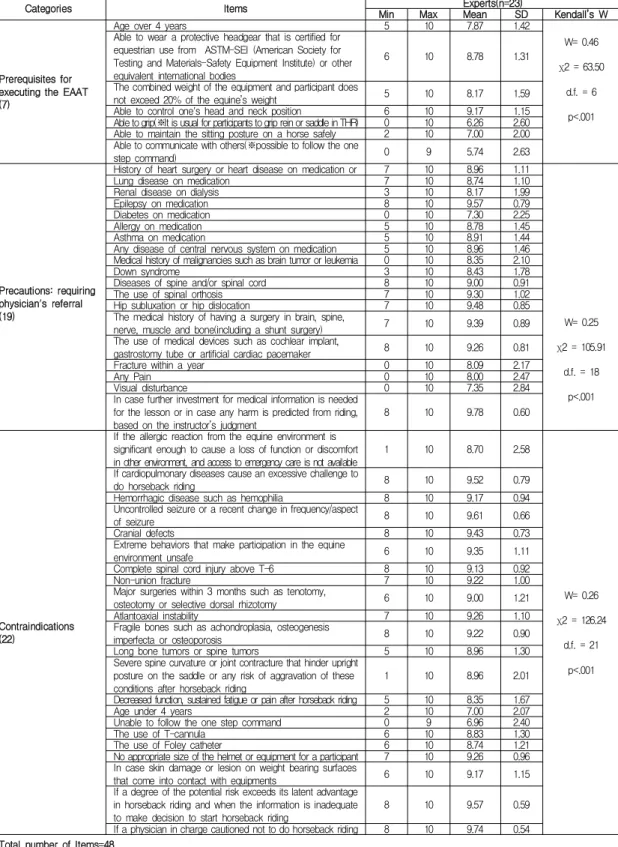
Table 3. Importance of each item in the 2nd delphi survey
Categories Items Prerequisites for
executing the EAAT (3)
Able to wear a protective headgear that is certified for equestrian use from ASTM-SEI (American Society for Testing and Materials-Safety Equipment Institute) or other equivalent international bodies
The combined weight of the equipment and participant does not exceed 20% of the equine’s weight Able to control one's head and neck position
Precautions: requiring physician's referral (16)
History of heart surgery of heart disease on medication Lung disease on medication
Renal disease on dialysis Epilepsy on medication Allergy on medication Asthma on medication
Any disease of central nervous system on medication Medical history of malignancies such as brain tumor or leukemia Down syndrome
Diseases of spine and/or spinal cord The use of spinal orthosis Hip subluxation or hip dislocation
The medical history of having a surgery in brain, spine, nerve, muscle and bone(including a shunt surgery) Fracture within a year
The use of medical devices such as cochlear implant, gastrostomy tube or artificial cardiac pacemaker
In case further investment for medical information is needed for the lesson or in case any harm is predicted from riding, based on the instructor’s judgment
Contraindications (20)
If cardiopulmonary diseases cause an excessive challenge to do horseback riding Hemorrhagic disease such as hemophilia
Uncontrolled seizure or a recent change in frequency/aspect of seizure Cranial defects
Extreme behaviors that make participation in the equine environment unsafe Non-union fracture
Major surgeries within 3 months such as tenotomy, osteotomy or selective dorsal rhizotomy Atlantoaxial instability
Fragile bones such as achondroplasia, osteogenesis imperfecta or osteoporosis Long bone tumors or spine tumors
Complete spinal cord injury above T-6
Severe spine curvature or joint contracture that hinder upright posture on the saddle or any risk of aggravation of these conditions after horseback riding
If the allergic reaction from the equine environment is significant enough to cause a loss of function or discomfort in other environment, and access to emergency care is not available
Decreased function, sustained fatigue or pain after horseback riding The use of T-cannula
The use of Foley catheter
No appropriate size of the helmet or equipment for a participant
In case skin damage or lesion on weight bearing surfaces that come into contact with equipments
If a degree of the potential risk exceeds its latent advantage in horseback riding and when the information is inadequate to make decision to start horseback riding
If a physician in charge cautioned not to do horseback riding Total number of Items=39
Table 4. EAAT screening tool for children and adolescents 각각‘재활승마는 고삐 쥐기, 말 안장 쥐기 등의 활동이 많 이 포함됨’과 ‘한 단계 이상 지시 따라 하기 가능’ 이라는 부연 설명을 항목 옆에 추가하였다. 금기증에서 ‘뼈에 발 생한 종양’ 항목을‘장골(long bone), 척추에 발생한 종양’
으로 수정하였고 ‘기관 삽입’ 항목 또한 구체적인 설명이 필요하다는 의견에 따라 ‘T-cannula를 하고 있는 경우’
로 수정하였다.
3.2.2 2차 델파이 조사결과 Table 3
2차 델파이 조사결과는 1차 설문지의 평균, 표준편차, 사분위수 범위를 옆에 표기하여 1차 조사결과를 반영하 여 작성하도록 하였다. 또한 2차 델파이 조사에서는 전문 가 의견의 우선순위와 항목별 중요도에 대한 델파이 전 문가들의 의견 일치도를 확인하기 위하여 켄달의 일치계 수(Kendall's Coefficient of Concordance;W)를 사용하였 으며 사용 결과, 모든 영역에서 통계적으로 유의하다는 p
값이 산출되어 평가자들의 의견이 상호간에 일치 된 것 으로 나타났다. 2차 델파이 조사에 대한 자료 분석을 통 해 전체 문항에 대한 적절성이 평균 8점 이상으로 나타났 고 이에 따라 적절성 8점 이하인 항목은 최종 선별도구 항목에서 제외하였다. 제외된 항목은 재활승마를 시행 할 수 있는 기본 조건 영역에서 ‘만 4세 이상’, ‘쥐기 가능’,
‘말에 앉는 자세를 안전하게 유지 할 수 있는 경우’와 ‘의 사소통 가능’ 4 항목, 주의 사항에서 ‘당뇨병으로 약물 치 료 중, ‘시각장애’와 ‘통증이 있는 경우’ 3 항목, 그리고 금 기 사항에서‘만 4세 이하’와 ‘한 단계 지시 수행이 어려운 경우’ 2 항목으로 총 9 항목이다. 따라서 39개의 항목이 최종적으로 선정되었다. Table 4, <Appendix 1>
4. 고찰
재활승마의 효과는 다양한 측면에서 보고되고 있는데, 머리와 몸통의 조절 능력[12] 및 보행 기능의 향상[13]과 같은 신체적인 효과가 있다. 참가자가 말의 움직임에 적 응하기 위해 사용하는 근육과 관절의 움직임은 관절가동 범위를 향상 시키며[14], 정교하면서 부드럽고 리드미컬 한 말의 걸음걸이는 인간의 보행과 흡사하여, 골반의 움 직임을 정상화 시킨다[13]. 권[2]등은 뇌성마비 아동을 대 상으로 주 2회, 30분씩, 8주간의 치료승마를 제공한 결과, 보속과 보폭의 향상, 골반의 움직임의 정상화를 보고하 였다. 치료승마는 다양한 운동수준을 보이는 뇌성마비 아동에서 대운동기능(Gross motor function)과 균형 (Balance)을 향상시켰다[1]. 또한 주의력결핍과잉행동장 애와 자폐스펙트럼장애와 같은 정신질환에서도 재활승 마의 효과들이 보고되었다[3,15]. 이와 같이 재활승마는 다양한 질환군에서 적용되고 있으며, 국내에서도 말산업 육성법의 시행과 함께 재활승마지도사들이 배출되면서 재활승마 프로그램을 시행하는 승마장이 점점 증가하는 추세이다.
현재 전 세계적으로 보급된 재활승마 가이드라인은 존재하지 않으며, 북미에서는 국제재활승마협회의 기준 매뉴얼을[9], 영국과 호주 뉴질랜드 등 영연방 국가에서 는 영국을 기반으로 하는 영국 장애인 승마협회의 ‘영국 장애인 승마협회 강사/코치를 위한 지도서: 승마에 있어 서의 금기증’을[11]<Appendix 2> 선택하여 사용하고 있 다. 이 중 더 까다로운 규정을 가지고 있는 것은 국제재
활승마협회의 기준 매뉴얼로 50여 페이지에 이르는 주의 사항을 제시하고 있다. 치료사들이 프로그램을 운영하는 미국 치료승마협회는 국제재활승마협회의 기준 매뉴얼 보다 더 유연한 규정을 적용하고 있다[16]<Appendix 3>.
앞선 외국 가이드라인들이 금기로 정하고 있는 요소 들은 크게 세 가지로 볼 수 있다. 첫 번째로 승마 활동이 기존 질환을 악화시킬 우려가 있는 경우, 두 번째로 낙상 의 우려가 큰 경우, 마지막 세 번째로 낙상할 경우 손상 의 위험도가 정상인보다 경우이다. 승마 활동이 기존 질 환을 악화시킬 우려가 있는 경우는 척추 및 척수의 질환, 관절의 불안정성, 두개골 결손, 골절, 뼈를 약하게 하는 질환, 고관절 탈구 등이다. 낙상의 우려가 큰 경우는 위험 한 돌출 행동을 보이는 경우, 관절 구축, 척추 및 척수의 질환으로 말 위에서 안전하게 자세를 유지하지 못하는 경우, 조절되지 않는 경기 등이 해당된다. 낙상할 경우 손 상의 위험도가 정상인보다 큰 경우는 혈우병과 같은 출 혈성 질환, 두개골 결손, 뼈를 약하게 하는 질환, 장골 (long bone) 및 척추에 발생한 종양 등이 해당된다.
국제재활승마협회의 기준 매뉴얼은 2세 미만 참가자 에게 기승을 금지하고 있다. 2세 미만의 어린이는 신체적 신경학적 발달이 미숙하여 말에서부터 오는 감각이나 움 직임을 조직화하기에 불충분하며, 천문이 아직 열려 있 는 경우 두개골 결손과 동일한 위험성을 가질 수 있기 때 문이다. 또한 미성숙한 척추에 반복되는 스트레스가 가 해지거나, 머리를 잘 가누지 못하는 상태에서 말의 움직 임으로 경추에 반복되는 미세한 손상이 가해질 위험이 있으며 말의 급작스런 움직임은 머리조절 능력이 성숙하 지 않은 참가자에게 경추부염좌(whiplash-type)와 같은 손상을 일으킬 수 있다. 한편 발달지연이 없는 아동이라 할지라도 만 3세경까지 보행의 패턴이 성숙되지 않으므 로, 이보다 어린 연령에서는 아동의 보행과 고관절에 미 치는 영향을 고려하여야 한다. 전반적 발달지연을 보이 는 아동의 경우에는 더 높은 생활 연령에서 2세 수준의 신체적 정신적 나이에 도달하므로 이를 충분히 고려하여 야 한다. 이런 논의 끝에 최근 국제재활승마협회 기준 매 뉴얼의 연령 기준을 4세 이상으로 수정하려는 움직임이 있으며, 이미 많은 승마장에서 연령 기준을 4세 이상으로 운영하고 있고 국내의 삼성전자승마단에서도 4세의 연령 기준을 사용하고 있다. 하지만 본 연구에서 ‘4세 미만’ 항 목은 합의에 이르지 못하여 해당 항목은 기타 고려사항 에 추가 되었다.
환축추 불안정성(atlantoaxial instability)은 의학용어 임에도 불구하고 모든 가이드라인에서 금기증으로 정하 고 있을 정도로 중요하기 때문에 해당 용어를 그대로 사 용하였다. 환축추 불안정성이 있으면 척수에 압력이 전 달되어 신경학적 손상을 일으킬 수 있기 때문이다. 다운 증후군, 류마티스 관절염 등과 같이 환축추 불안정성을 동반하는 질환에서는 머리 조절(head control)의 정도가 기승을 시킬 것인지 여부를 결정하는 중요한 요소이며, 해마다 전문의가 신경학적 검사와 단순촬영을 시행하여 진행 여부를 확인하는 과정이 필요하다. 그 밖에 척추에 압력이 가해질 경우 신경학적 손상을 일으킬 수 있는 질 환들로는 척추전방전위증(spondylolisthesis), 수척수증 (hydromyelia), 2형 키아리 병변(arnold-chiari malformation type II), 척수견인증후군(tethered cord) 등이 있으며 외 국의 금기 사항에도 포함되어 있다. 이러한 질환들은 모 두 척수이분증(spina bifida)과 연관되므로 어려운 의학 용어를 최대한 줄인다는 원칙에 따라‘척추, 척수의 질환’
이라는 용어 내에 포함하여 의사의 소견서를 받도록 하 였다. 여기서 2형 키아리 변형은 척수이분증 환자들이 사 망에 이르는 주요 원인으로 미국 치료승마협회와 국제재 활승마협회에서는 증상을 동반한 2형 키아리 변형 환자 에서 기승을 금지하고 있다.
외국의 가이드라인에 포함된 류마티스 관절염 (rhematoid arthritis), 척추간판탈출증(herniated nucleus pulposus), 다발성 경화증(multiple sclerosis), 당뇨병 (diabetes)과 같은 급성기 질환들은 소아청소년기에 흔하 지 않고, 질환의 범위가 광범위하며 급성기라는 정의가 모호한 문제점이 있어 본 연구에는 포함하지 않았다. 그 대신 이러한 질환들은 승마 활동 후 통증이 증가하거나 악화를 보일 가능성이 높으므로 ‘승마 활동 후 지속되는 피로, 통증, 기능의 저하’ 나 ‘기타 승마의 위험이 잠재적 이점을 초과하고 기승자가 활동을 지속하기 위해 정보에 근거한 결정을 내릴 수 없는 경우’ 로 재활승마지도사의 판단에 따라 기승 여부를 결정하도록 하였다. 당뇨병이 심한 경우 조절이 잘 안 되는 상태에서 혼수상태에 빠질 수 있으며[17] 감각의 저하로 피부 손상의 위험이 있으므 로 조절되지 않는 당뇨를 영국 장애인 승마협회, 국제재 활승마협회, 미국 치료승마협회 모두에서 금기 사항에 넣고 있다. 본 연구에서 ‘당뇨로 약물치료 중’ 항목을 주 의 항목에 넣어 의사의 소견서를 받도록 제시하였으나 합의에 이르지 못하였다. 국내 소아청소년들에서 당뇨의
낮은 유병율을 고려하였을 때, 당뇨의 심한 합병증을 보 이는 참가자는 거의 없을 것으로 예상되지만 ‘지도사의 판단에 근거, 기승 시 위험이 예상되거나, 레슨에 필요한 의학적 정보가 필요한 경우’항목에 근거하여 전문의의 진료를 요청하는 것이 권장된다.
영국 장애인 승마협회의 금기증은 국제재활승마협회 의 기준 매뉴얼보다 더 관대한 규정을 가지고 있으며, 금 기증에 해당 할 경우 의사에게 의뢰하지 않고, 승마활동 을 바로 규제한다. 연령 규정이 없는 대신 저하된 머리 조절 기능(poor head control), 저하된 몸통 조절 기능 (poor trunk control) 그리고 앉기 균형(sitting balance), 항목이 들어있다는 점, 척추의 변형에 대한 규정을 각도 로 명확히 하였다는 점이 주된 차이점이다. 본 연구에서 영국 장애인 승마협회의 금기증인 다발성 경화증, 망막 박리(Detached retina), 척추고정술(Spinal rodding)은 소 아청소년기에 매우 드물기 때문에 선별도구에 포함시키 지 않았다. 한편 척추 질환인 척추전방전위, 척추측만증 (scoliosis), 척추후만증(kyphosis)는 어려운 의학 용어이 고, 해당 질환은 x-ray를 통해서 측정할 수 있기 때문에 금기보다는 주의 항목에‘척추, 척수의 질환’으로 반영하 여 의사의 소견서를 받도록 하였다. 영국 장애인 승마협 회에서는 말에 앉기가 독립적으로 되는 경우에 한해서 프로그램을 진행하는 것을 원칙으로 하고 있으며, 재활 승마 사이드 워커(Side-Walker)는 어깨높이 이상으로 기 승자를 지지하지는 않도록 하고 있다. 본 연구에서 재활 승마를 시행하기 위한 기본 요건에서 ‘말에 앉는 자세를 안전하게 유지할 수 있는 경우’ 항목이 합의에 이르지 못 하였는데, 몸통의 균형을 향상시키는 것이 재활승마의 주요 목표이므로 몸통의 균형이 종지 않은 환아들이 재 활승마의 적응증이라는 패널의 의견이 있었다. 몸통의 균형이 좋지 않은 경우 재활승마 사이드 워커들이 환아 를 지지하며 프로그램을 진행할 수는 있다. 하지만 지지 가 과도할 경우에는 말의 움직임이 전달되는 것을 방해 하므로 결국 재활승마가 효과적으로 진행되기 어렵다는 점을 고려하여야 한다.
본 선별도구에서 외국의 가이드라인과 특별히 다른 점은 ‘수술 3개월 이내’를 금기 사항으로 정하였다는 것 이다. 소아청소년기에 중요 수술은 뇌성마비 환아들에서 시행하는 건절제술, 골절단술, 후근절제술 등이 가장 흔 하다. 이러한 환아들에서 언제부터 승마활동이 가능할 것인 지에 대한 규정은 없으나 일반적으로 3개월간은 회
복기로 볼 수 있으므로 절대 금기 기간을 설정하였다. 3 개월이 지난 경우라도 ‘뇌, 척추, 신경, 근육, 뼈의 수술 병 력’에 해당하여 의사의 소견서가 필요하며, 의사가 허락 하는 경우에 기승하도록 하였다. 그러나 수술마다 회복 을 요하는 기간은 다를 것이므로 일괄적으로 3개월의 규 정을 정하는 것은 한계가 있다. 피부, 눈, 귀의 간단한 수 술은 수 주 만에 회복되어 별 문제 없이 기승을 할 수 있 을 것으로 판단된다. 그러나 비의료인이 1차 선별을 한다 는 부담감, 각 수술마다 재활승마가 가능한 적절한 회복 기간을 판정할 수 있는 과학적 근거의 부족, 대체로 소아 청소년기에 수술을 받는 경우는 중대한 사항이라는 점을 고려 시, 참가자의 안전을 최대한 보호 하여야 한다는 차 원에서 수술의 명칭은 다소 모호한 표현으로 남겨 두었다.
국내에서 재활승마를 가장 오랜 기간 동안 시행한 삼 성전자 승마단은 재활승마 선정 기준에, 최소한 안장을 잡을 수 있는 쥐기 능력, 한 단계 지시를 수행할 수 있는 의사소통 능력을 적용하고 있다. 시각장애의 경우도 참 가자의 안전을 고려하여 배제하고 있는데, 본 연구에서 이들 항목은 합의에 도달하지 못하였고 이는 외국의 가 이드라인과 동일하다.
5. 결론
본 선별도구는 국내 재활승마 전문가들의 합의를 거 쳐 도출된 것으로, 재활승마지도사들이 승마장에서 기승 전 선별검사로 사용하여 안전한 재활승마 프로세스 구축 에 기여할 것이다. 본 선별도구의 사용으로 참가자들의 불필요한 의료기관 방문 절차를 줄일 수 있으며, 의사들 로부터 참여에 대한 허락을 받는 과정에서 승마 활동 참 여를 과도하게 제한 받지 않을 뿐 아니라, 반대로 참가자 들의 무리한 요구로부터 의사와 지도사들을 보호할 수 있을 것으로 기대된다. 또한 참가자들의 의학적 평가를 의뢰받은 의사들에게도 본 연구 결과는 참고자료로 활용 될 수 있을 것이다. 비록 국내 전문가들에 의해 합의되지 않은 항목들이라 할지라도 참가자의 안전을 위해 고려하 는 것이 권장된다. 그러나 본 선별도구는 소아청소년기 의 특성을 반영하여 도출된 것으로 향후 성인 환자들을 대상으로 한 추가적인 연구가 필요하다.
REFERENCES
[1] Kwon, J. Y., Chang, H. J., Yi, S. H., Lee, J. Y., Shin, H.
Y., & Kim, Y. H. (2015). Effect of hippotherapy on gross motor function in children with cerebral palsy: a randomized controlled trial. The Journal of Alternative
and Complementary Medicine, 21(1), 15-21.
[2] Kwon, J. Y., Chang, H. J., Lee, J. Y., Ha, Y., Lee, P. K.,
& Kim, Y. H. (2011). Effects of hippotherapy on gait parameters in children with bilateral spastic cerebral palsy. Archives of physical medicine and rehabilitation,
92(5), 774-779.
[3] Jang, B., Song, J., Kim, J., Kim, S., Lee, J., Shin, H. Y., Kwon, J. Y., Kim, Y. H., & Joung, Y. S. (2015).
Equine-assisted activities and therapy for treating children with attention-deficit/hyperactivity disorder.
The Journal of Alternative and Complementary Medicine, 21(9), 546-553.
[4] Bixby-Hammett, D. M., & Brooks, W. H. (1989).
Neurologic injuries in equestrian sports. Sports neurology, 229-234.
[5] Ball, C. G., Ball, J. E., Kirkpatrick, A. W., & Mulloy, R.
H. (2007). Equestrian injuries: incidence, injury patterns, and risk factors for 10 years of major traumatic injuries.
The American Journal of Surgery, 193(5), 636-640.
[6] Ghosh, A., DiScala, C., Drew, C., Lessin, M., & Feins, N.
(2000). Horse-related injuries in pediatric patients.
Journal of pediatric surgery, 35(12), 1766-1770.
[7] Hobbs, G. D., Yealy, D. M., & Rivas, J. (1994).
Equestrian injuries: a five-year review. The Journal of
emergency medicine, 12(2), 143-145.
[8] Centers for Disease Control and Prevention. (1996).
Horseback-riding-associated traumatic brain injuries--Oklahoma, 1992-1994. MMWR: Morbidity and
mortality weekly report, 45(10), 209-211.
[9] Path intl. (2016). Professional Association of Therapeutic Horsemanship International PRECAUTIONS AND CONTRAINDICATIONS INDEX. www.pathintl.org/
images/pdf/standards-manual/2016/2016-PATH-Intl-Se ction-L-Precautions-and-Contraindications.pdf [10] Dalkey, N., & Helmer, O. (1963). An experimental
application of the Delphi method to the use of experts.
Management science, 9(3), 458-467.
[11] Riding for the Disabled Association. (2015). Chartered Physiotherapists in Therapeutic Riding and Hippotherapy:
Guidance for RDA Groups and Instructors/Coaches:
Contra-indications for riding. www.rda.org.uk/assets/
Contra-indication-guidance-revd-1115.pdf
[12] Shurtleff, T. L., Standeven, J. W., & Engsberg, J. R.
(2009). Changes in dynamic trunk/head stability and functional reach after hippotherapy. Archives of physical
medicine and rehabilitation, 90(7), 1185-1195.
[13] McGee, M. C., & Reese, N. B. (2009). Immediate effects of a hippotherapy session on gait parameters in children with spastic cerebral palsy. Pediatric Physical Therapy,
21(2), 212-218.
[14] McGibbon, N. H., Benda, W., Duncan, B. R., &
Silkwood-Sherer, D. (2009). Immediate and long-term effects of hippotherapy on symmetry of adductor muscle activity and functional ability in children with spastic cerebral palsy. Archives of physical medicine and
rehabilitation, 90(6), 966-974.
[15] Yoo, J. H., Oh, Y., Jang, B., Song, J., Kim, J., Kim, S., Lee, J., Shin, H. Y., Kwon, J. Y., Kim, Y. H., Jeong, B.,
& Joung, Y. S. (2016). The Effects of Equine-assisted Activities and Therapy on Resting-state Brain Function in Attention-deficit/Hyperactivity Disorder: A Pilot Study. Clinical Psychopharmacology and Neuroscience,
14(4), 357.
[16] American Hippotherapy Association. (2014). Best Practice Statements for the Use of Hippotherapy by Occupational Therapy, Physical Therapy, and Speech- Language Pathology Professionals.
www.americanhippotherapyassociation.org/wp-content/
uploads/2015/02/FINAL_ver_Best-Practice_12_30_15.pdf [17] Wolfsdorf, J., Glaser, N., & Sperling, M. A. (2006).
Diabetic ketoacidosis in infants, children, and adolescents. Diabetes care, 29(5), 1150-1159.
황 영 섭(Hwang, Young Sub) [학생회원]
▪2016년 2월 : 연세대학교 원주캠 퍼스 작업치료학과(이학사)
▪2016년 3월 ∼ 2017년 2월 : 분당 서울대학교병원 작업치료사
▪2016년 9월 ∼ 현재 : 강원대학교 삼척캠퍼스 응급의료재활학과(이 학석사)
▪2017년 8월 ∼ 현재 : 삼성서울병원 재활의학과 연구원
▪관심분야 : 작업치료, 소아재활, 뇌성마비
▪E-Mail : [email protected]
장 현 정(Chang, Hyun Jung) [정회원]
▪1999년 2월 : 이화여자대학교 의 학과 학사
▪2006년2월 : 연세대학교 의과대학 재활의학 석사
▪2012년2월 : 부산대학교 의과대학 재활의학 박사
▪1999년 3월 ∼ 2000년 2월 : 이대부속병원 수련의
▪2001년 3월 ∼ 2005년 2월 : 세브란스병원 재활의학과 전공의
▪2005년 3월 ∼ 2009년 2월 : 삼성서울병원 재활의학과 임상강사 및 임상조교수
▪2009년 3월 ∼ 현재 : 성균관대 삼성창원병원 재활의학 과 임상부교수
▪관심분야 : 소아재활, 암재활
▪E-Mail : [email protected]
홍 보 영(Hong, Bo Young) [정회원]
▪2011년 2월 : 가톨릭대학교 의과 대학 재활의학 박사
▪2009년 3월 ∼ 2011년 2월 : 서울 성모병원 재활의학과 임상강사
▪2011년 3월 ∼ 2014년 2월 : 성빈 센트병원 재활의학과 임상조교수
▪2014년 3월 ~ 2018년 3월 : 성빈센트 재활의학과 조교수
▪2018년 4월 ~ 현재 : 성빈센트병원 재활의학과 부교수
▪관심분야 : 재활의학, 소아재활, 뇌성마비
▪E-Mail : [email protected]
이 지 영(Lee, Ji Young) [정회원]
▪2012년 2월 : 삼육대학교 대학원 물리치료학과 이학석사
▪2000년 8월 ∼ 2003년 3월 : 삼성 서울병원 재활의학과 물리치료사
▪2003년 4월 ∼ 현재 : 삼성전자승 마단 재활승마센터 물리치료사, 재활승마지도사
▪관심분야 : 물리치료, 재활승마, 치료승마
▪E-Mail : [email protected]
권 정 이(Kwon, Jeong-Yi) [정회원]
▪1993년 2월 : 서울대학교 의학과 학사
▪2000년 2월 : 서울대학교 의과대 학 재활의학 석사
▪2007년 2월 : 서울대학교 의과대 학 재활의학 박사
▪2004년 9월 ∼ 2005년 3월 : 가톨릭의대 성빈센트병원 재활의학과 전임강사
▪2005년 4월 ∼ 2008년 9월 : 가톨릭의대 성빈센트병원 재활의학과 조교수
▪2008년 10월 ∼ 2009년 2월 : 삼성서울병원 재활의학과 임상부교수
▪2009년 3월 ∼ 2015년 3월 : 삼성서울병원 재활의학과 부교수
▪2015년 4월 ∼ 현재 : 삼성서울병원 재활의학과 교수
▪관심분야 : 재활의학, 소아재활, 뇌성마비
▪E-Mail : [email protected]
영역 항목 재활승마를 시행 할 수
있는 기본 조건
국제 안전 기준 (ASTM 등)을 통과한 헬맷에 머리가 맞는 경우 사람과 마구의 몸무게 합이 말 체중의 20% 이내
머리와 목의 조절이 가능
주의 사항 기승 전 의사로부터 전문
소견을 필요
심장수술의 병력, 심장질환으로 약물 치료 중 폐질환으로 약물 치료 중
신장질환으로 투석 중 경기약 복용 중 알레르기로 약물 치료 중 천식으로 약물 치료 중
중추신경계 질환으로 약물 치료 중 뇌종양, 백혈병과 같은 소아암 병력 다운증후군
척추, 척수의 질환 척추보조기를 착용한 경우 고관절 아탈구 혹은 탈구
뇌, 척추, 신경, 근육, 뼈의 수술 병력 (션트 수술 포함) 1년 이내 골절
인공와우, 위루관, 인공심박기와 같은 의료장치를 가지고 있는 경우
지도사의 판단에 근거, 기승 시 위험이 예상되거나, 레슨에 필요한 의학적 정보가 필요한 경우
금기증
말을 타기 어려운 정도의 심폐 질환 혈우병과 같은 출혈성 질환
조절되지 않는 경기 혹은 빈도 및 양상의 변화를 최근 보이는 경우 두개골 결손
위험한 돌출 행동을 보이는 경우
골절 치료중이거나 골절 후 완전 유합이 되지 않은 경우 건절제술, 골절단술, 후근절제술과 같은 수술 3개월 이내 환축추 불안전성
연골무형성증, 불완전 골형성증, 골다공증과 같은 뼈를 약하게 하는 질환 장골(long bone), 척추에 발생한 종양
흉추6번 상부의 완전한 척수손상
관절 구축, 척추의 변형, 뼈의 변형으로 말 위에서 안전하게 자세를 잡지 못하거나, 상기 변형이 진행될 우려가 큰 경우
알레르기 반응이 기능 소실이나 불편함을 일으키나 즉각적 조치가 어려운 경우 (응급실과의 거리가 먼 경우) 승마 활동 후 지속되는 피로, 통증, 기능의 저하
T-cannula를 하고 있는 경우 요관 삽입
기승자의 체형에 맞는 마구나 헬맷이 없는 경우 안장이나 마구가 닿는 부위의 피부 질환, 손상이 있는 경우
기타 승마의 위험이 잠재적 이점을 초과하고 기승자가 활동을 지속하기 위해 정보에 근거한 결정을 내릴 수 없는 경우
담당 의사가 기승하지 말도록 지시한 경우
※ 기타 고려 사항 1. 만 4세 미만
2. 한 단계 지시를 수행할 수 없는 경우 3. 시각 장애
4. 안장이나 고삐를 쥘 수 없는 경우
5. 말에 앉는 자세를 안전하게 유지 할 수 없는 경우 6. 통증이 있는 경우
7. 당뇨병으로 약물 치료 중
<Appendix 1>. 소아청소년을 대상으로 한 재활승마 선별도구
<Appendix 2>. Guidance for RDA(Riding For The Disabled Association) Groups and Instructors/Coaches:
Contra-indications for riding
Poor Head Control: It is necessary that a rider can control the position of their head so that it does not flop or rest forward or behind the upright position. So, if there is no head control, riding is not undertaken. Hippotherapy may be used as a means of gaining more head control.
Hip dislocation: Many children with CP will have a degree of Dysplasia of one or both hips. Where there is no pain associated with it, riding can be good, encouraging the hips into a position where they may settle into the joints. Pain may not be vocalised but can be recognised by increased spasm or the rider’s unwillingness to tolerate certain positions. Advice should be sought from a physiotherapist.
Osteoporosis/osteogenesis: Weakness of the bones, either from birth or acquired. When serious even the act of positioning the feet in the stirrups could cause fractures. It can be the result of long term use of certain drugs. Falls could be very dangerous. Riding is not advised.
Diabetes: Many diabetics have their disease under control, are unlikely to lose
consciousness and would be safe to ride. It is necessary to know if they are likely to become unwell and what action must be taken.
If this is a frequent occurrence riding is not advised. One of the side effects of diabetes is loss of sensation and poor circulation (see Circulatory and sensation problems)
Haemophilia: In this condition, the control of bleeding is a problem. There can be bleeding into joints if they are strained. This is a serious problem and riding is not advised if the condition is severe.
Acute inflammatory condition: This is a generalised illness and riding is not advised while the body is working to respond to the inflammatory process. It may be in joints, muscles and soft tissue or internal organs. Rheumatoid arthritis is an inflammatory disease and may have acute flair ups during which time riding should be stopped.
Spondylolisthesis: This is a condition where one bone in the spine has moved forward on the one below, carrying the upper body with it. This creates an unstable spine and the potential for nerve damage and paralysis. Riding is not advised.
Uncontrolled epilepsy: Uncontrolled epilepsy means that a fit can occur at any time and any place. This is not a safe scenario with horses. An RDA coach will consider applications from participants with epilepsy on a case by case basis guided by the RDA policy on epilepsy. Ultimately the decision to accept or reject an application for riding rests with the coach in charge of the ride.
Circulatory/pressure problems and problems with sensation: It is useful if riders are able to feel if any parts of the body are being rubbed by equipment. With poor circulation or nerve damage this sensation may be reduced. Riders should be on sheepskin or similar pressure reducing pads and all leathers need to be without edges in contact. Ask carers to check skin carefully after each ride. Poor circulation can lead to very cold hands and feet, so consideration should be given to appropriate riding venues and times of year.
Scoliosis>40 degrees: Scoliosis is unnatural complex three dimensional deformity curving the spine most distinctly sideways. If the curves are gentle, normal activities are encouraged. When the angle of the curve is 40 degrees or more, the downward pressure of gravity is pushing it to go further. The action of the horse can increase the pressure through the spine and increase the curve, so medical advice is essential to confirm the degree of curve. A physiotherapist should be consulted.
Acute phase MS: People with MS can suffer relapses when there can be some
deterioration in their condition, ranging from sensory symptoms such as numbness, loss of power and severe fatigue. It is not advisable to ride during this acute phase. It usually passes but may leave the rider less able and lacking confidence, so it is important to reassess and be alert to any changes from previous level of riding. Care should be given to increase the ride time gradually.
Atlanto/occipital instability: This can occur in people with Down’s syndrome. It is weakness at the joint at the top of the neck; injury to that area can cause paralysis. A judgement has to be made on the amount of head control the potential rider has and advice sought from a physiotherapist with experience of using hippotherapy.
Kyphosis>40 degrees (severe): Kyphosis is the medical term for a forward bend of the spine. It occurs naturally in the mid spine but to a minimal degree. Where the forward bend is more pronounced, the same effect will be happening with gravity as in scoliosis. Riding could increase the problem.
Spinal rodding (depending on level): When the bones of the spine are fixed together by means of a rod inserted down the length, the effect is to block the movement from the horse in this area but cause excess elsewhere. In this case riding is not advised. Sometimes this rodding is done to small segments, in which case riding can still be beneficial to mobilise and strengthen the rest of the body. If there has been ANY spinal surgery to insert rods guidance must be sought from the Consultant and Physiotherapist.
Detached retina: This is an acute problem of the eye and no sudden movements should occur while it is being treated. Riding is not advised.
Poor trunk control and sitting balance: If a rider can only remain on the horse be being held up by side walkers then some of the value of the movement of the horse is being blocked. The rider should be able to maintain independent sitting on the horse for the duration of the ride. Any support from side walkers should not be given above their own shoulder height (for their safety). Rides may have to be shortened to work with the rider’s tolerance and stamina.
Shunt: This is a length of tubing taking excess liquid from the brain into the stomach. A tube may be visible under the skin around the ear. Great care should be taken in fitting hats. Any complaint of headache should be taken seriously as shunts can become blocked.
If this occurs during a ride, the ride should cease and the carers be informed. Riding should not recommence until the problem is resolved.
Febrile illness: If a rider has an elevated temperature they must not ride as they may have an infection which could be made worse by physical exertion or could be transmitted to others.
<Appendix 3>. American Hippotherapy Association, Inc.: PRECAUTIONS AND CONTRAINDICATIONS TO HIPPOTHERAPY
Essential considerations for continued use of equine movement
Hippotherapy inherently involves movement. If the movement will cause a decrease in the patient’s function, an increase in pain, or generally aggravate the medical condition, hippotherapy may not be an appropriate choice.
Hippotherapy establishes a human-animal interaction. If this interaction is detrimental to the patient or the horse, hippotherapy may be contraindicated.
Hippotherapy requires the use of certain equipment in a prescribed environment, and is, by definition, interaction with a horse.
The outdoor environment for hippotherapy is much less controlled than that of an indoor clinic. If the therapist cannot accommodate the patient’s equipment needs, or the environment will aggravate his or her condition, hippotherapy may not be appropriate.
There is always potential risk for a fall in hippotherapy. In most instances, the fall would be from four or six feet above the ground.
Such a fall may cause a greater functional impairment than the patient originally had. The possibility of a fall should be given careful consideration, and may lead to the informed decision that hippotherapy is not appropriate for that patient.
Participating in activities around a horse involves risk. Even the well -trained horse is sometimes unpredictable, subject to its instinctive fight or flight responses. Horses are large, move quickly and can be dangerous to the patient who is unable to respond appropriately.
Hippotherapy requires intervention by a team. The treatment team most often
involves the therapist, horse handler, therapy horse, and side walker/therapy aides. If any members of the team are not qualified or trained in appropriate hippotherapy procedures, including safety; or, if an essential member of the team is absent, then hippotherapy is contraindicated.
Medications - As with all therapy sessions, consideration must be given to the
medications, prescription and over the counter, the patient is taking. Of special concern is that hippotherapy takes place in the outdoor environment, with considerations such as weather (heat/cold/sunlight/wind) and allergens. Be familiar with all of the patient’s medications, dosages, time of administration, recent changes, and side effects. Your best resource regarding medications is the patient’s physician and/or pharmacist.
ABSOLUTE CONTRAINDICATIONS FOR HIPPOTHERAPY