학 술 논 문
48
방사선촬영 보조기구를 이용한 어린이 흉부 엑스선 검사에 관한 연구
이도병 1 ·이소미 3 ·최현우 2 ·김종기 1 ·이종민 3
1대구가톨릭대학교 생체의료공학과, 2경북대학교대학원 의용생체공학과, 3경북대학교 의학전문대학원 영상의학교실
A Study on Chest X-ray Using Ancillary Device for Child Radiography
Do-byung Rhee 1 , Somi Lee 3 , Hyunwoo Choi 2 , Jong-ki Kim 1 and Jongmin Lee 3
1
Department of Biomedical Engineering, Daegu Catholic University
2
Department of Biomedical Engineering, Kyungpook National University
3
Department of Radiology, School of Medicine, Kyungpook National University
Abstract In this study, We developed a Ancillary device for child radiography for X-ray of children under 5 years old and verified its effectiveness. Chest X-rays of children younger than 5 years of age were performed by Supine method at the position of Table detector, Short - Source to Image Receptor Distance(SID). Existing Supine and Short -SID imaging methods cause many problems, such as errors in image reading and excessive radiation exposure dose to patients, but the use of an Ancillary device for child radiography(ADCR) solves these problems. A total of 160 children were divided into the Upright group using ADCR and Supine group without ADCR. The chest X-ray image was visually evaluated by two radiologists with reference to the European Commission's List of Quality Criteria for Diagnostic Radiographic Images in Pediatrics. The total score of the qualitative evaluation was 5.15% higher in the chest upright method using ADCR than in the chest supine method without ADCR, and the chest upright method score was higher than that of the chest supine method in items 1 to 7. whether infants have deep inspiration or not, 4.87% higher for item 1, whether infants rotate or not and the degree of tilting, 0% higher for the item 2, the repro- duction of image from just above apices of lungs to T12/L1, 0% for the item 3, reproduction of the vascular pattern in central 2/3 of the lungs, 6.92% higher for the item 4, reproduction of the trachea and the proximal bronchi, 12.9%
higher for the item 5, visually sharp reproduction of the diaphragm and costo-phrenic angles, 10% higher for the item 6, reproduction of the spine and paraspinal structures and visualisation of the retrocardiac lung and the mediastinum, and 3.65% higher for the item 7. Items 2 and 3 showed no statistically significant differences( P > 0.05), and items 1, 4, 5, 6, and 7 showed statistically significant differences( P < 0.05). In conclusion, Upright method using ADCR in pediatric chest X-ray is considered as a good alternative to existing Supine method.
Key words : Ancillary Device for Child Radiography, Kilovoltage Peak, Milliamperage Second, Half Value Layer, Automatic Exposure Control
I. 서 론
현대의학에서는 과학기술과 함께 의료영상을 이용하여 환
자의 질병을 진단하고 치료하는 기술이 크게 발전하였다. 그 중에서도 방사선을 이용한 검사는 비교적 간단한 방법으로 빠른 시간 안에 정확한 진단을 할 수 있어 그 사용빈도가 크게 증가하고 있다. 식품의약품안전처에서 조사한 결과에 의하면 2007년부터 2011년까지 의료기관에서 환자들에게 진단을 목적으로 실시한 방사선 검사는 5년간 약 35% 증 가하였고 피폭선량은 0.93 mSv에서 1.4 mSv로 약 51% 증 가하였다[1]. 최근 병원을 방문하는 어린이 환자의 수가 과 거에 비해 급격히 증가하고 있으며, 따라서 어린이 흉부 엑 Corresponding Author : Jongmin Lee
(700-721) 50, Sam-Duk 2 Ga, Jung-gu, Daegu, Republic of Korea
TEL: +82-53-420-5472 E-mail: [email protected]
방사선촬영 보조기구를 이용한 어린이 흉부 엑스선 검사에 관한 연구.
49 스선(Chest X-ray) 검사의 빈도도 크게 증가하였다. 일반
적으로 5세 미만 어린이의 Chest X-ray 검사는 짧은 선원 검출기간 거리(Short-source to image receptor distance, SID) 에서 전후 방향 바로 누운 자세(Anterior-posterior supine position) 로 시행되는데 그 이유는 어린이의 연령대 가 낮을수록 의사소통과 행동 통제가 매우 어려워 검사자와 보호자가 붙잡은 상태에서만 검사가 가능하기 때문이다. 그 럼에도 신체의 움직임으로 인한 자세의 뒤틀림은 고정하기 가 어려워 영상에서 장기의 구조물을 겹치게 하는 원인을 제공하기도 한다. 서울대학교 어린이병원에서 시행한 연구에 의하면 어린이 Chest X-ray 검사 중에서 Table Detector 위 치에 바로 누운 자세(Supine position)로 시행하는 검사는 전체 검사 중 61%의 비율로 영상에서는 머리 회전(Head rotation), 턱 선에 의한 기도 묘사 불충분(Insufficient expression of trachea by jaw line), 쇄골에 의한 폐야의 겹침(Overlapping of the lungs by the clavicle) 등이 주 로 나타났으며, 나이 분포로는 생후 24개월 이하가 가장 많 았다고 한다[2,3]. 일반적인 Chest X-ray 검사는 섬세한 폐 구조의 재현과 심장 확대의 최소화를 위하여 SID 180 cm 이상의 원거리(Long distance)에서 촬영하기를 권고하지만 [4], 일어서지 못하는 환자이거나 특히, 움직임이 많은 5세 미 만의 어린이와 같은 경우에는 Table Detector 위치에서 Supine 자세로 SID 100∼120 cm 정도의 선원(Source)으로 부터 짧은 거리에서 촬영을 시행한다. 기존의 바로 누운 Supine 방식의 Chest X-ray 검사는 횡격막 상승(Diaphragm rises), 심장 확대(Enlarged heart), 종격동 비대(Mediastinal
hypertrophy), 대동맥 확장(Aorta expansion), 견갑골과 폐야 의 겹침(Overlapping of the scapula and the lung) 등 을 일으켜 영상 판독에서 오류를 야기 시키며[5], 짧은 거 리(Short-SID)에서의 촬영은 환자에 대한 골수(Bone marrow) 에 방사선 피폭선량을 적게 할 수는 있으나 갑상 선(Thyroid)과 가슴(Chest)에 많은 방사선 피폭선량을 받 게 한다[6]. 본 연구는 어린이 Chest X-ray 검사에서 기존 의 바로 누운 Supine 자세로 촬영하는 방식의 단점을 해결 하기 위하여 방사선촬영 보조기구(Ancillary device for child radiography, ADCR) 를 이용하여 바로 직립한 자세 (Upright) 방식을 적용해 보았다. Upright 방식으로 촬영 된 영상과 Supine 방식으로 촬영된 영상을 비교, 분석하여 어린이 Chest X-ray 검사에 있어 가장 효율적이고 적합한 방법이 무엇인지 알아보고자 한다.
II. 대상 및 방법
1. 연구대상
본 연구에서는 Chest X-ray 검사를 위해 어린이병원 영 상의학과를 방문한 생후 6개월 이상 48개월 이하의 남녀 어 린이 160명 중에서 방사선촬영 보조기구(Ancillary device for child radiography, ADCR) 를 이용한 Upright 방식과 방사선촬영 보조기구(ADCR)를 이용하지 않은 기존의 Supine 방식을 구분하여 검사를 진행하였다. 검사를 하기 전 환자와 보호자에게 검사의 목적 및 절차, 방법에 대하여 충분한 사전 설명을 하였고 동의한 환자에 한하여 보호자가
그림 1. 방사선촬영 보조기구의 개발과 흉부 엑스선 직립 자세 촬영 방식[16]. (a) 보조기구 본체, (b) 흉부 수평 촬영용 평판, (c) 이동용 검 출기, (d) 복부 촬영용 쐐기모양 부재.
Fig. 1. Development of Ancillary Device for Child Radiography and Chest X-ray Upright Position Method[16]. (a) Device Main Body, (b) Flat Table for Chest Decubitus X-ray, (c) Portable Detector, (d) Wedge for Abdomen X-ray.
50
지켜보는 가운데 검사를 진행하였다. 환자의 신체적 특징은 남녀 성비(Male to female ratio), 키(Height), 몸무게 (Weight), 나이(Age), 체질량지수(Body mass index, BMI) 를 측정하였다.
2. 실험장비
본 연구에서는 방사선촬영 보조기구(ADCR)를 개발하여 어린이 Chest X-ray 검사에 이용하였다(그림 1). X-ray 장 비로는 Digital Radiography X-ray System(Innovision- SH 3D; DK healthcare company, korea) 으로 간접 전환 방식(Indirect conversion, Amorphous-silicon/cesium iodide type) 의 고정용 평면 패널 검출기(Flat-panel detector) 를 사용하였다. 크기는 17 × 17(43 × 43 cm) inch 이며 화소 수(Pixel number)는 3,072 × 3,072이다. X선관 의 고유여과(Inherent filtration)는 0.5 mm/Al이고, 초점 크 기(Focal spot size)는 0.6/1.2 mm이며 조사야 크기(Field of view, FOV) 는 12 × 12 inch로, 자동노출제어장치(Automatic exposure control, AEC) mode 를 설정하였다. 해상도 (Resolution) 는 4.0 Lp/mm, 화소 간격(Pixel pitch)은 140 µ(micron), 격자 비율(Grid ratio)은 12:1의 고정형 평행 격 자(Stationary parallel pattern grid)를 사용하였다. X-ray 장비의 출력의 측정하기 위해 Multi-function tester (Unfors- xi & R/F detector, billdal, sweden)를 사용하여 관전압(Tube voltage, Kilovoltage peak; kVp), 관전류 × 시간(Tube current × sec, Milliamperage second; mAs), 반가층(Half value layer, HVL) 그리고 Phantom의 흉부 면에 도달하는 입사면 공기선량(Incident air kerma, IAK)을 측정하였다.
III. 실험방법
1. Qualitative Visual Scoring
정성적인 시각적 평가는 무작위로 선별한 어린이 160명 을 대상으로 방사선촬영 보조기구(ADCR)를 이용한 바로 직 립한 자세 그룹(Upright group)과 ADCR을 이용하지 않은 바로 누운 자세 그룹(Supine group)으로 구분하여 시행하였 다(그림 2, 3). 촬영한 영상을 European Commission의
‘List of Quality Criteria for Diagnostic Radiographic Images in Pediatrics[7]’ 를 기준으로 폐(Lung), 심장(Heart), 횡격막(Diaphragm), 흉막 각(Costo-phrenic angles), 기도 및 근위 기관지(Trachea and the proximal bronchi)의 선 명도와 흉부(Chest)의 회전과 기울기 여부를 영상의학과 전 문의 2명(Radiologist with 20 years experienced, Pediatric radiologist with 8 years of experienced) 이 총 10 점 중에서 1, 2점은 좋지 않음(Poor), 9, 10점은 좋음 (Good), 6 점 이상은 수용 가능한 품질(Satisfaction)로 간주
하여 전반적인 영상에 점수를 부여하여 평가하였다(Table 1).
Radiologists 의 주관적인 판단의 오류를 최소화하기 위하여 영 상 평가는 모두 당일 처리 완료하였다.
2. Radiography Equipment
먼저 Supine 방식은 선원 검출기간 거리(Source to image receptor distance, SID) 120 cm 에서 Tube Voltage 70 kVp, Tube Current × Sec 3.56(±1.15) mAs 의 조건으로 촬영하였다. 방사선촬영 보조기구(ADCR)를 이 용한 Upright 방식은 SID 180 cm에서 Tube Voltage 110 kVp, Tube Current × Sec 2.04(±0.33) mAs 의 조건 으로 촬영하였다. ‘European Commission’에서 5세 어린 이 Chest X-ray 검사에서 AEC mode를 사용할 것과 Tube Voltage 를 60~80 kVp 및 Tube Voltage 100~120 High kVp 로 설정할 것을 권고하였으므로[7] 본 연구에서는 AEC 사용과 함께 Tube Voltage 중간(mean) 값인 70 kVp와 110 kVp 를 설정하여 각각 적용하였다.
3. Measurement of Radiography Equipment Output Table Detector 와 Stand Detector 간의 성능차이를 검
그림 3. 어린이 흉부 엑스선 검사에서 방사선촬영 보조기구를 이용 한 직립한 자세 방식.Fig. 3. Pediatric Chest X-ray-Upright Method using ADCR.
그림 2. 어린이 흉부 엑스선 검사에서 방사선촬영 보조기구를 이용 하지 않은 바로 누운 자세 방식.
Fig. 2. Pediatric Chest X-ray-Supine Method without ADCR.
51 증하기 위해 각 Detector에 Phantom(ATOM® dosimetry
phantom, model 705-D, CIRS, Norfolk, VA, US) 을 놓고 Multi-Function tester 를 이용하여 장비의 kVp, mAs, HVL, IAK 값을 측정하였다. 두 검출기(Detector)와 선원(Source) 과의 거리는 동일하게 120 cm로 설정하였고 AEC mode를 사용한 상태에서 Tube Voltage를 60 kVp 에서 130 kVp 까 지 10 kVp 단위씩 증가시켜서 각각의 값을 측정하였다.
4. Statistical Analysis
본 연구에서는 Statistical Package for Social Science (SPSS 20.0) 통계 프로그램을 이용하여 방사선촬영 보조기 구(ADCR)를 이용한 Upright Group과 ADCR을 이용하지 않은 Supine Group으로 구분한 어린이 160명의 신체 특 징에 관한 부분(Male to female ratio, Age, Height, Weight, BMI) 을 통계적 유의성 검증을 시행하였으며 Radiologists 2 명이 European Commission의 ‘List of Quality Criteria for Diagnostic Radiographic Images in Pediatrics[7]’ 를 참고하여 채점(Visual scoring) 한 결과 를 각 항목과 총점의 평균(mean) 값과 표준편차(Standard deviation) 를 산출하여 비교하였다. 두 그룹간의 유의한 차이 를 확인하기 위해 Independent-Sample T-test를 실시하 였고 통계적 유의 수준은 P < 0.05로 설정하였다.
IV. 연구 결과 및 고찰
1. Qualitative Visual Scoring & Statistical Analysis 방사선촬영 보조기구(Ancillary device for child radiography, ADCR) 를 이용한 Upright Group과 ADCR
을 이용하지 않은 Supine Group으로 구분한 어린이 160 명의 신체 특성에 관한 부분을 통계적 유의성 검증 결과 Male to female ratio, Age, Height, Weight, BMI 모두 통계적 유의한 차이가 없었다(P > 0.05, Table 2). 그리고 Radiologists 가 두 그룹에 대하여 채점(Visual scoring) 한 결과는 2, 3 문항에서 점수가 같았고 1, 4, 5, 6, 7 문항에 서 ADCR을 이용한 Upright 방식이 ADCR을 이용하지 않 은 Supine 방식 보다 높은 점수를 획득하였다. 특히 1. 심 흡기 여부(Performed at peak of inspiration)에서 4.87%, 4. 폐 중앙 2/3 지점에 혈관 모양의 재현성(Reproduction of
표 1. 유럽위원회의 소아에 대한 진단 방사선 영상의 품질 기준 목록.Table 1. The European Commission's List of Quality Criteria for Diagnostic Radiographic Images in Pediatrics.
DIAGNOSTIC REQUIREMENTS ← Score →
Poor Satisfactory Good
Image criteria 1 2 3 4 5 6 7 8 9 10
1. Performed at peak of inspiration, except for suspected foreign body aspiration
2. Reproduction of the thorax without rotation and tilting
3. Reproduction of the chest must extend from just above the apices of the lungs to T12/L1
4. Reproduction of the vascular pattern in central 2/3 of the lungs 5. Reproduction of the trachea and the proximal bronchi
6. Visually sharp reproduction of the diaphragm and costo-phrenic angles 7. Reproduction of the spine and paraspinal structures and visualisation
of the retrocardiac lung and the mediastinum
Total:
표 2. 방사선촬영 보조기구를 이용한 바로 직립한 자세 그룹과 방사 선촬영 보조기구를 이용하지 않은 바로 누운 자세 그룹으로 구분한 어린이 160명에 대한 신체적 특성을 독립표본 T-검정 시행 결과(성 비, 나이, 신장, 체중, 체질량지수).
Table 2. Independent-Sample T-test Results of Upright Group Using ADCR and Supine Group not Using ADCR(Male to female ratio Age, Height, Weight, Body mass index).
Variable ADCR used- Upright Group
ADCR none-
Supine Group P-Value No. of
patients 80 80
Male to
female ratio 44 : 36 53 : 27 0.147
Age(month) 21.0 ± 10.7 19.1 ± 11.2 0.442 Height(cm) 83.7 ± 9.7 80.7 ± 9.3 0.61 Weight(kg) 17.0 ± 2.8 16.2 ± 3.0 0.12 BMI(kg/m2) 12.1 ± 2.0 10.9 ± 11.2 0.36
52 the vascular pattern) 에서 6.9%, 5. 기도와 기관지 모양의 재현성(Reproduction of the trachea and the proximal bronchi) 에서 12.9%, 6. 횡격막과 흉막 각의 시각적 선명도 (Visually sharp reproduction of the diaphragm and costo-phrenic angles) 에서 10%, 7. 척추 주위 구조물과 심 장 후방과 종격동의 시각화(Reproduction of the spine and paraspinal structures and visualisation of the retrocardiac lung and the mediastinum) 에서 3.65%의 더 높은 비율을 보여 ADCR을 이용한 Upright 방식이 기 존의 Supine 방식 보다 시각적으로 주는 유익이 매우 크다 고 할 수 있다(그림 4). 반면에 2. 흉부의 회전과 기울기 여부 (Reproduction of the thorax without rotation and tilting) 와 3. 폐 첨부에서 허리뼈 1번까지의 재현성(Reproduction of the chest must extend from just above the apices of the lungs to T12/L1) 은 두 그룹의 점수가 같았는데, 그 이유 는 어린이를 Table Detector에 누워 고정시킨 Supine 자 세나 Stand Detector에서 ADCR을 이용하여 고정시킨 Upright 자세가 모두 공통적으로 Detector에 등을 맞대고 있는 자세이므로 2번 항목, 흉부의 회전과 기울기 여부에서 차이를 나타내지 않은 것으로 판단되며, Supine과 Upright 두 방식의 촬영은 Table / Stand 두 Detector size가 17
× 17 inch의 같은 크기에서 시행되기 때문에 3번 항목, 폐 첨부에서 허리뼈 1번까지의 전체 구조물에 대한 표현 여부 에서 차이가 없는 것으로 나타났다. Supine / Upright 두
방식에서 도출된 결과를 Independent Sample T-test 하 여 비교한 결과 2, 3 항목(P > 0.05, Table 3)을 제외한 Total Score, 1, 4, 5, 6, 7 항목에서는 모두 통계적으로 유 의한 차이를 나타냈다(P < 0.05, Table 3). Table Detector 와 Stand Detector 간의 성능차이 검증을 위해 AEC mode 를 사용한 동일한 조건으로 SID 120 cm에서 측정한 kVp, mAs, HVL, IAK 값을 Mann Whitney U-test 결과 kVp( P : 0.418), mAs(P : 0.980), HVL(P : 0.394), and IAK( P:0.758)로 모든 값은 통계적 유의한 차이가 없는 것 으로(P > 0.05) 나타나 Table / Stand 두 Detector 간의 성 능은 동일한 것으로 판단하였다. ‘ICRP Publication 16’에 의하면 선원과 환자 피부면과의 짧은 거리(Short Focus- skin distances)는 X-ray Beam에서 높은 비율로 연속으 로 발생되는 투과력이 약한 방사선 때문에 환자에게 입사하 는 방사선 피폭선량이 많아진다고 하였다[8]. X-ray 검사에 있어서 부적절한 선원 검출기간 거리(Source to image receptor distance, SID) 의 설정은 환자에게 피부면 입사 선량(Entrance surface dose, ESD)을 높이면서 방사선에 의한 결정적 영향(Deterministic effect)[9] 또는, 확률적 영 향(Stochastic effect)에 위험한 영향을 미친다[10,11]. 반 가층(HVL) 측정은 X-ray 조사 시 균일성의 지표를 평가할 때 사용하는데[12], Tube Voltage(kVp)가 일정하게 출력되 는 상태에서 SID를 증가하면 Tube Current × Sec(mAs)도 증가하여 환자의 피폭선량이 높아질 수 있으나 HVL도 함
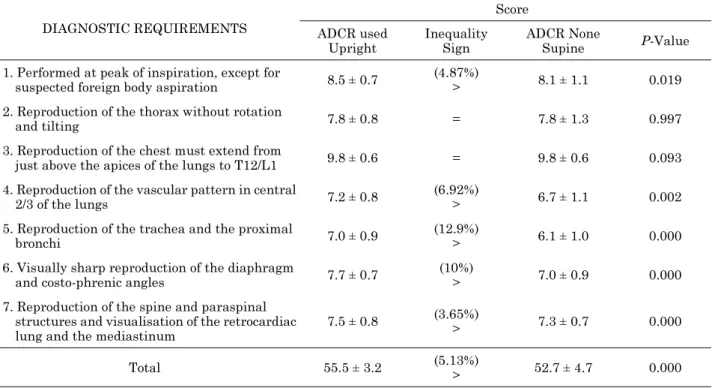
표 3. 시각적 채점 분석 결과에 대한 독립표본 t-검정 결과.Table 3. Independent-Sample T-test of Visual Grading Analysis Scores Result.
DIAGNOSTIC REQUIREMENTS
Score ADCR used
Upright
Inequality Sign
ADCR None
Supine P-Value
1. Performed at peak of inspiration, except for
suspected foreign body aspiration 8.5 ± 0.7 (4.87%)
> 8.1 ± 1.1 0.019
2. Reproduction of the thorax without rotation
and tilting 7.8 ± 0.8 = 7.8 ± 1.3 0.997
3. Reproduction of the chest must extend from
just above the apices of the lungs to T12/L1 9.8 ± 0.6 = 9.8 ± 0.6 0.093 4. Reproduction of the vascular pattern in central
2/3 of the lungs 7.2 ± 0.8 (6.92%)
> 6.7 ± 1.1 0.002
5. Reproduction of the trachea and the proximal
bronchi 7.0 ± 0.9 (12.9%)
> 6.1 ± 1.0 0.000
6. Visually sharp reproduction of the diaphragm
and costo-phrenic angles 7.7 ± 0.7 (10%)
> 7.0 ± 0.9 0.000
7. Reproduction of the spine and paraspinal structures and visualisation of the retrocardiac lung and the mediastinum
7.5 ± 0.8 (3.65%)
> 7.3 ± 0.7 0.000
Total 55.5 ± 3.2 (5.13%)
> 52.7 ± 4.7 0.000
53 께 증가하므로 공기 중 여과 효과(Air-filter effect)에 의한
공기 중 불필요한 Soft X-ray가 제거되면서 평균에너지가 상승된 Hard Beam X-ray만 남게 된다[13,14]. 그러므로 SID 의 증가는 환자에게 도달하는 방사선 피폭선량 (Radiation dose) 을 감소시킬 수 있는 중요한 요인이라고 할 수 있다[15]. Chest X-ray 검사에서 올바른 촬영 방법 과 적절한 SID 설정은 어린이의 방사선 노출 감소와 관련 하여 많은 이점을 제공하며 ADCR의 사용은 영상 판독에 있어서 시각적 우수성을 제공하며 Chest X-ray 검사 시 환 자의 방사선 피폭선량을 줄여줄 수 있는 좋은 방법으로 생 각된다.
IV. 결 론
5 세 미만 어린이의 Chest X-ray 검사는 주로 Table Detector 위치에서 바로 누운 Supine 자세로 선원(Source) 과 검출기(Detector) 간의 짧은 거리(Short-source to image receptor distance) 에서 시행되었다. 기존의 Supine 방식과 Short-SID 촬영방식은 영상 판독에서의 오류와 환자 가 불필요하게 받을 수 있는 방사선 피폭선량 노출에 대한 문제를 발생 시켜왔다. 방사선촬영 보조기구(ADCR)의 사 용은 이러한 문제들을 해결해 준다. ADCR은 움직임이 많 은 어린이를 안전하게 고정시켜 주어 흔들림 없는 정확한 영상을 구현할 수 있는 장점이 있다. 어린이 Chest X-ray 검사에서 기존의 Supine 방식은 고정된 SID로 짧은 거리 에서 시행할 수 밖에 없었지만 ADCR을 활용한 Upright 방식은 자유로운 SID 설정으로 선원으로부터 원거리(Long -source to image receptor distance) 촬영이 가능하여 환자
의 피폭선량 측면에서 유익이 있다. European Commission 의 ‘List of Quality Criteria for Diagnostic Radiographic Images in Pediatrics[7]’ 를 참고하여 Radiologists가 영상 평가한 결과에 의하면 ADCR을 사용한 Upright 방식이 기 존의 Supine 방식 보다 시각적 영상 평가에서 대부분 높은 평가를 받았다. 특히 기도(Trachea)와 기관지(Bronchus)의 재현성에서 12.9%, 횡격막(Diaphragm)과 흉막 각(Costo -phrenic angles) 의 선명도에서 10% 이상의 큰 비율 차이 를 보여 Chest X-ray 영상에서 Upright 방식은 해부학적 구조물을 표현하는 부분에서 큰 장점을 나타냈다고 할 수 있다. 따라서 어린이 Chest X-ray 검사에서 ADCR를 이용 한 Upright 방식의 적용은 기존의 Supine 방식에서 발생 하는 문제를 해결할 수 있는 좋은 대안으로 생각되며, 앞으 로 어린이 Chest X-ray 검사에 있어서 많은 유익을 끼칠 수 있을 것으로 보인다.
참고문헌
[1] Ministry of Food and Drug Safety, “Press Releases, Con- ducted national radiological records management program for CT patients,” Internet: http://www.mfds.go.kr/index.do?
mid= 675&seq=22654&cmd=v, accessed on Jan. 14, 2014.
[2] K.S Jung, C.W Song, and J.W Moon, “Image Analysis of Pediatric Chest Radiography,” in Proc. 2004 Spring Meeting of the Seoul Radiological Technologists Association, Seoul, Korea, April, 2004, vol. 10, no. 1, pp. 83-88.
[3] C.W Song, S.H Baek, and S.S Bae, “Child and Infant Chest AP examination’s usefulness which use assistance tool,” in Proc. 2005 Spring Meeting of the Seoul Radiological Technol- ogists Association, Seoul, Korea, March. 2005, vol. 11, no. 1, pp. 39-46.
그림 4. 바로 직립한 자세 방식과 바로 누운 자세 방식을 비교한 정성적인 시각적 채점 그래프 결과.
Fig. 4. Qualitative visual scoring graph result of Upright method and Supine method.
54
[4] E.D Frank, B.W Long, B.J Smith, and V. Merrill, Merrill's atlas of radiographic positioning & procedures, 2012, pp.
496-498.
[5] N. Raby, L. Berman, S. Morley and G. De Lacey, Accident and Emergency Radiology: A Survival Guide E-Book. Else- vier Health Sciences, 2014, pp. 307-328.
[6] H.J Lee, “Interpretation of Plain Chest Radiography-Focused on Findings of Normal and Pneumonia,” Korean Journal of Pediatrics, vol. 45, no. 11, pp. 1311-1316, 2002.
[7] European Commission, European guidelines on quality crite- ria for diagnostic radiographic images in paediatrics, Lux- embourg: Office for Official Publications of the European Communities, EUR. 16261, 1996.
[8] International Commission on Radiological Protection, Protec- tion of the patient in x-ray diagnosis, Oxford: ICRP, Publica- tion 16, 1970. pp. 18-20.
[9] Wagner, Louis K., Patricia J. Eifel, and Richard A. Geise.
“Potential biological effects following high X-ray dose inter- ventional procedures,” Journal of Vascular and Interven- tional Radiology, vol. 5, no. 1, pp. 71-84, 1994.
[10] Kebart, R. C. and C. D. James. “Benefits of increasing focal film distance,” Radiologic technology, vol. 62, no. 6, pp.
434-442, 1991.
[11] Brennan, P. C. and M. Nash. “Increasing FFD: an effective dose-reducing tool for lateral lumbar spine investigations,”
Radiography, vol. 4, no. 4, pp. 251-259, 1998.
[12] S.J Kim, “The great encyclopedia of nursing science,” Seoul, Korea: Korea Dictionary Research, 1997.
[13] Jones, A. Kyle, and Alexander S. Pasciak. “Calculating the peak skin dose resulting from fluoroscopically guided inter- ventions. Part I: Methods,” Journal of Applied Clinical Med- ical Physics, vol. 12, no. 4, pp. 231-244, 2011.
[14] Valentin, Jack. “Radiation and your patient: A guide for med- ical practitioners: ICRP Supporting Guidance 2Approved by ICRP Committee 3 in September 2001,” Annals of the ICRP, vol. 31, no. 4, pp. 1-52, 2001.
[15] Robinson, J, and D. McLean. “Extended focal-film distance technique: an analysis of the factors in dose reduction for the AP knee radiograph,” Radiography, vol. 7, no. 3, pp. 165- 170, 2001.
[16] J.M Lee, D.B Rhee and G.S Yoon, Radiation Imaging Auxil- iary Device and Radiation Imaging Apparatus, Korean. Pat- ent 10-1625057, May 23, 2016.
![Fig. 1. Development of Ancillary Device for Child Radiography and Chest X-ray Upright Position Method[16]](https://thumb-ap.123doks.com/thumbv2/123dokinfo/5335650.392579/2.892.171.724.774.1058/development-ancillary-device-child-radiography-upright-position-method.webp)