Small Bowel Obstruction with Strangulation Caused by Patent Omphalomesenteric Duct
4
0
0
전체 글
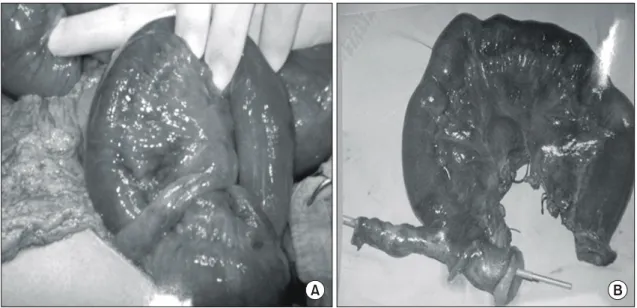
(2) 남소현 외:소장 교액을 유발한 개방성 배꼽창자간막관. 331. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. 증가되어 있는 것 이외에 특이 소견 없었다. 복부 단순 촬영 에서 팽만된 여러 개의 소장고리와 공기-액체층을 보여 기 계적 장폐색증을 의심하였다(Fig. 1). 복부 전산화 단층 촬 영에서는 위와 소장이 심하게 팽만되어 있으며 내부에 공 기-액체층을 관찰할 수 있었으며 원위부 회장이 끝이 뾰족 해지면서 골반강내에 뭉쳐 장벽의 부종을 보이고 있었으며 장간막내부의 혈관이 돌아가 있는 소견을 보였다(Fig. 2). 이상의 소견으로 기계적 장폐색에 의한 소장 교액을 의심 하여 응급 개복술을 시행하였다. 수술 소견상 혈성복수가. 약 1,000 ml 정도 고여 있었으며, 회맹판으로부터 대략 30 cm 상방의 회장과 배꼽 사이에 개방성 배꼽창자간막관으 로 추정되는 관형의 구조물을 발견하였다. 개방성 배꼽창 자간막관이 밴드 역할을 하면서 그 공간 사이로 소장이 탈 장되어 장 폐색을 일으키고 탈장된 장은 교액 상태로 되어 있었다(Fig. 3). 수술은 탈장된 장을 복원하고 교액된 소장 과 개방성 배꼽창자간막관을 절단 후 단단 소장문합술을 시행하였다. 이외 복강내 다른 장기에 특이소견은 없었다. 수술 후 조직검사상 장간막 반대편에 5 cm×1 cm 길이의. A. B. Fig. 2. Abdominal & pelvic CT shows the distal small bowel obstruction with internal herniation(arrow: r/o Meckel`s diverticulum).. A. B. Fig. 3. Grossly, on antemesenteric border shows an elongated tubular structure, measuring 5×1 cm. The serosa is purplish brown and hemorrhagic. On opening, the tubular structure opens into small intestine. The inner surface of the tubular structure shows hemorrhagic mucosal folds. The mucosa of the small intestine is unremarkable. The wall is hemorrhagic. The mesentery is hemorrhagic..
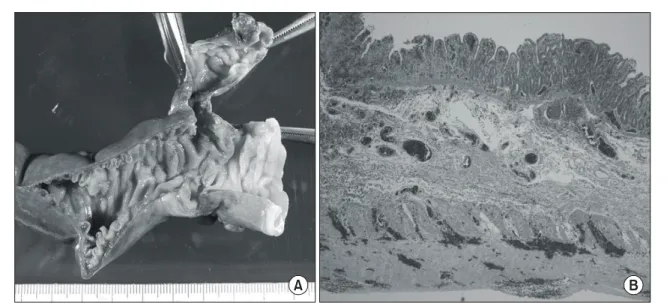
(3) 332. 대한외과학회지:제 67 권 제 4 호 2004. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. A. B. Fig. 4. Pathologic finding shows that the patent omphalomesenteric duct consists of full thickness of intestinal wall lined by small intestinal type mucosa with focal ischemic necrosis and hemorrhage.. 긴 관형 구조물이 있었으며 이는 소장의 점막과 같은 장벽 으로 구성된 개방성 배꼽창자간막관으로 진단되었다(Fig. 4). 환자는 수술 후 특별한 합병증 없이 퇴원하였다.. 고. 찰. 난황낭은 태생 2∼3주경까지 자궁태반순환이 완성될 때 까지 영양분을 공급하는 통로로써 중요한 역할을 담당하며 9주경에는 배모양의 잔여물로 5 mm 정도로 작아져 중장관 과는 난황자루(yolk stalk)의 형태로 연결되다가 10주경에는 퇴화된다.(1,4) 제대부기형은 제대부의 폐쇄가 이루어지지 않거나 배꼽창자간막관이 계속 남아있어 형성되며,(5) 그 형태로는 배꼽창자간막관이 열려 있어 회장과 배꼽사이의 누관을 형성하는 경우, 배꼽 용종, 배꼽 물혹, Meckel 게실, 배꼽탈장, 섬유화 밴드 등을 볼 수 있다.(1,3) 그 중 가장 흔 한 것은 Meckel 게실로 유병율은 2∼4%에 이르며 이는 회 맹판으로부터 60 cm 이내에 회장의 장간막 반대편에 생기 며 장관의 전 층을 포함하는 특징이 있다. 제대부기형의 대 부분은 증상을 일으키지 않으나 증상이 생기게 되면 위장 관 출혈 및 장폐색, 소장의 감돈 등의 급성 복증으로 나타날 수 있다.(6-9) 배꼽창자간막관이 회장과 지속적으로 연결되 어 있는 경우 장 내용물의 배출이 이루어질 수 있고, 이곳을 통해 회장의 탈출, 장중첩증 등을 일으킬 수 있으며,(3) 회 장의 탈출 혹은 장관 폐색이 생긴 경우 이환율 및 사망률이 높아지므로 개방성 배꼽창자간막관을 수술적으로 절제해 야만 한다.(10,11) Meckel 게실은 대부분 증상이 없으나 합 병증이 생긴 경우 25∼50%에서 위장관 출혈의 형태로 나타 나며 10∼20%에서는 장관 폐색, 장관 염전, 게실염 등의 형 태로 나타날 수 있다. 드물게는 양성 신생물, 악성 신생물. 등의 형태로도 나타날 수 있다. 합병증이 생겼을 경우 치료 로는 게실의 절제 혹은 게실을 포함한 소장 부분절제를 시 행하여야 한다.(1,6,10,12) 배꼽창자간막관에 의해 장폐색증 이 일어날 수 있는 상황은 첫째, 함입된 Meckel 게실이 선두 점으로 작용하여 장중첩이 일어난 경우, 둘째 배꼽에 붙어 있는 개방성 배꼽창자간막관을 축으로 장관 염전이 생기거 나 이 밴드가 소장고리에 압력을 가하게 되는 경우, 셋째 게실 밴드(mesodiverticular band)에 의해 내탈장되어 밀폐성 장폐쇄증이 되는 경우, 넷째 Meckel 게실의 염증에 이차적 으로 소장 유착이 생긴 경우, 다섯째 Littre's 탈장이 감돈된 경우, 여섯째 Meckel 게실이 저부에서 꼬인 경우, 일곱째 식 물위석 혹은 석(stone)이 Meckel 게실 내에 생겨 내강의 협 착을 일으킨 경우, 여덟째 열려 있는 배꼽창자간막관을 통 해 회장이 탈출되거나 장중첩이 생긴 경우로 분류해 볼 수 있다.(13) 본 증례는 이전의 수술 과거력 없는 33세 남자 환자가 배 꼽에 붙어 있는 개방성 배꼽창자간막관을 축으로 장관 염 전이 생기면서 소장 폐색 및 교액을 일으킨 경우에 해당한 다. 이상에서 살펴본 바 제대부 기형, 개방성 배꼽창자간막 관에 의한 합병증은 극히 드물지만 위장관 출혈, 소장 폐색 및 교액의 원인이 될 수 있다. 그러므로 정확한 원인이 규명 되지 않은 급성 복증, 특히 수술의 과거력이 없는 기계적 장폐색 및 소장 감돈의 유발원인으로 고려해보아야 할 것 이다.. REFERENCES 1) Konvolinka CW. Patent omphalomesenteric duct. Surgery 2002;131:689-90..
(4) 남소현 외:소장 교액을 유발한 개방성 배꼽창자간막관. 333. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 2) Hasegawa T, Sakurai T, Monta O, Tazuke Y, Ueda S, Iwasaki Y, et al. Transumbilical resection and umbilical plasty for patent omphalomesenteric duct. Pediatr Surg Int 1998;13: 180-1. 3) Disorders of the umbilicus in infants and children: A consensus statement of the Canadian Association of Paediatric Surgeons Paediatrics & Child health. Paediatr Child Health 2001;6: 312-3. 4) Moore TC. Omphalomesenteric duct malformations. Semin Pediatr Surg 1996;5:116-23. 5) Yoo SY, Lee CI, Kang SJ, Rhoe BS. Umbilical anomalies associated with omphalocele. J Korean Surg Soc 1990;39: 703-7. 6) Bueno Lledo J, Serralta Serra A, Planeeis Roig M, Dobon Gimenez F, Ibanez Palacin F, Rodero R. Intestinal obstruction caused by omphalomesenteric duct remnant: usefulness of laparoscopy. Rev Esp Enferm Dig 2003;95:736-8. 7) Filip F, Gotia DG, Aprodu SG, Vlad A, Savu A, Savu B, et al. Intestinal occlusion by persistence of the omphalo- enteric conduct in a 10-year old child. Rev Med Chir Soc Med Nat Iasi 2000;104:119-22. 8) Gaisie G, Curnes JT, Scatliff JH, Croom RD, Vanderzalm T.. 9). 10). 11). 12). 13). Neonatal intestinal obstruction from omphalomesenteric duct remnants. Am J Roentgenol 1985;144:109-12. Prabhu-Khanolkar S, Azmy AA, Raine PA. Closed loop intestinal obstruction due to vitello-intestinal remnants. Z Kinderchir 1985;40:188-9. Yamada T, Seiki Y, Ueda M, Yoshikawa T, Sempuku S, Kurokawa A, et al. Patent omphalomesenteric duct: a case report and review of Japanese literature. Asia Oceania J Obstet Gynaecol 1989;15:229-36. Lin HC, Lin JT, Deng HH, Lee HC, Lin ST. Intestinal volvulus caused by a persistent omphalomesenteric band: report of one case. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi 1995;36:58-60. Amendolara M, Pasquale S, Perri S, Carpentieri L, Errante D, Biasiato R. Intestinal occlusion caused by persistent omphalomesenteric duct and Meckel's diverticulum: report of 2 cases Chir Ital 2003;55:591-5. McClenathan JH, Dabadghav N. Unusual presentation of omphalomesenteric duct remnant: A variant of mesodiverticular band causing intestinal obstruction. J Pediatr Surg 2002; 37:267-8..
(5)
수치

관련 문서
