VOLUME 14, NUMBER 4, December 2009
Operative Treatment of the Fracture and Dislocation of the Fourth and Fifth Carpometacarpal Joints Simultaneously - Two Cases Report -
Hyun-Soo Park, MD, Jong Won Kim, MD
1, Min-Sok Shin, MD, Jae-Wook Jung, MD, Jin Phil, Yang, MD
Department of Orthopedic Surgery Hanil General Hospital, Seoul, Korea Hyundai General Hospital, Namyangjoo, Korea1
Simultaneoulsy carpometacarpal fracture and disloca- tion is known to be uncommon past days. But Fisher1 reported that it is quite common injury of hand in 1984.
Also high energy injury causes carpometacarpal joint fracture and dislocation, the result of treatment has wide spectrum of prognosis, so early diagnosis and treatment is essential. We reported 2 patients who had the fourth and fifth carpometacarpal fracture and dislocation.
(J Korean Soc Hand Surg 2009;14:255-9)
Key Words: Carpometacarpal joint, Fracture and dislo- cation, Closed pinning
서 론
수근 중수 관절의 골절 및 동시탈구는 심한 외력에
의해 발생하는 손상으로 과거에는 수부 손상에 있어 드문 손상으로 알려져 있었으나 최근에서는 이 손상 및 치료에 있어서 인식이 확대되고 있어 1984년 Fisher는1 수근 중수 관절의 골절 및 탈구의 손상이 드물지 않다고 문헌으로 보고한 바 있다. 또한 심한 외력으로 손상이 발생하는 만큼, 예후의 차이가 커서 손상에 대한 조기진단 및 적절한 치료가 중요시되고 있다. 이에 저자들은 수근 중수골 관절의 손상 중에서 동시에 발생하는 제 4, 5 수근 중수 관절의 골절 및 탈구에 대해 2예의 치험례를 바탕으로 수상기전, 진단 방법, 치료방법 그리고 예후 에 대해 문헌 고찰과 더 불어 보고하고자 한다.
증례 보고
증례 1
우측 손잡이인 27세 남성이 우측 주먹을 쥔 상태로 벽을 세게 친 후 발생한 우측 수부의 종창 및 동통을 주소로 응급실로 내원한 자로 내원 당시 이학적 진찰 상, 우측 수배부의 종창 및 동통, 그리고 척측 수근관 절 부위의 특징적인 압통이 관찰되었다. 피부에는 종 창외의 상처는 관찰되지 않았고, 원위부 감각 및 혈행 상태의 이상은 관찰되지 않았다. 수부의 전후면, 측 면, 그리고 사면의 단순 방사선 촬영상 제 4, 5 수지 중수골 기저부의 골절 및 배측 으로의 동시탈구가 관 찰되었고, 바로 촬영한 컴퓨터 단층 촬영상, 유구골의 견열골절 소견 으로 Cain 등2의 분류상 II형에 해당되 었다(Fig. 1A, B, C). 수지의 종축 견인을 통한 도 수정복을 시도하였고, 정복 후 척측 gutter 석고붕대 로 수부의 기능적 위치로 고정하였으나, 정복상태가 불안정하여 수술을 시행하게 되었다. 영상 증폭 장치 하에서 전완부의 회내전 상태에서 제 4, 5 수지의 종 축 견인 후 배측에서 수근 중수 관절에 압박력을 가하 여 정복시킨 상태를 유지하면서 K-강선을 제 4 중수 골 기저부에서 유두골로 삽입하여 고정하였고, 또 다
제
제 4 4,, 5 5 수 수근 근 중 중수 수골 골 관 관절 절의 의 골 골절 절 및 및 동 동시 시탈 탈구 구의 의 수 수술 술적 적 치 치료 료 -
- 2 2예 예 보 보고 고 - -
한일병원 정형외과학교실, 현대병원 정형외과학교실1 박현수∙김종원1∙신민석∙정재욱∙양진필
Address reprint requests to: JJoonngg WWoonn KKiimm,, MMDD
Department of Orthopaedic Surgery, Hyundai General Hospital, Janghyeon-ri 663, Jinjeop-eup, Namyangju-si, Gyeonggi-do, Korea
TEL: 031-574-9118, FAX: 031-572-1194 E-mail: osjongwon@hanmail.net
– 256 –
Fig. 3. (A, B, C) Six months follow-up after surgery, anteroposterior, oblique and lateral roentgenogram demonstrat- ing restoration of normal configuration of the carpometacarpal joint but it shows sclerosis of the car- pometacarpal joint.
Fig. 1. (A) Initial anteroposterior roentgenogram of the right hand, demonstrating overlapping of the fourth car- pometacarpal joint and small fragmentation of the fourth metacarpal base. (B) Lateral roentgenogram demon- strating dorsal dislocation of the fourth metacarpal bone with comminuted hamate fracture. (C) Initial com- puted tomography demonstrating dorsal dislocation of the fourth metacarpal bone and fragmentation of impacted hamate body.
Fig. 2. (A, B, C) Postoperative anteroposterior, oblique and lateral roentgenogram shows restoration of the normal anatomical configuration of the carpometacapal joint after closed reduction and pinning.
른 K-강선을 제 5 중수골 기저부에서 유구골을 향하 여 삽입하여 고정하였다(Fig. 2A, B, C). 수술 후 수부의 내재근 양성 위치에서 단 상지 석고고정을 시행 하였고, 6주 후, 외래 방문 시 단순 방사선 촬영을 통해
안정된 유지 상태를 확인하고, K-강선을 제거하였으며, 수술 후 6개월 후 추적 진료에서도 통증 없이 파악력의 회복을 건측의 80%이상 얻었다(Fig. 3A, B, C).
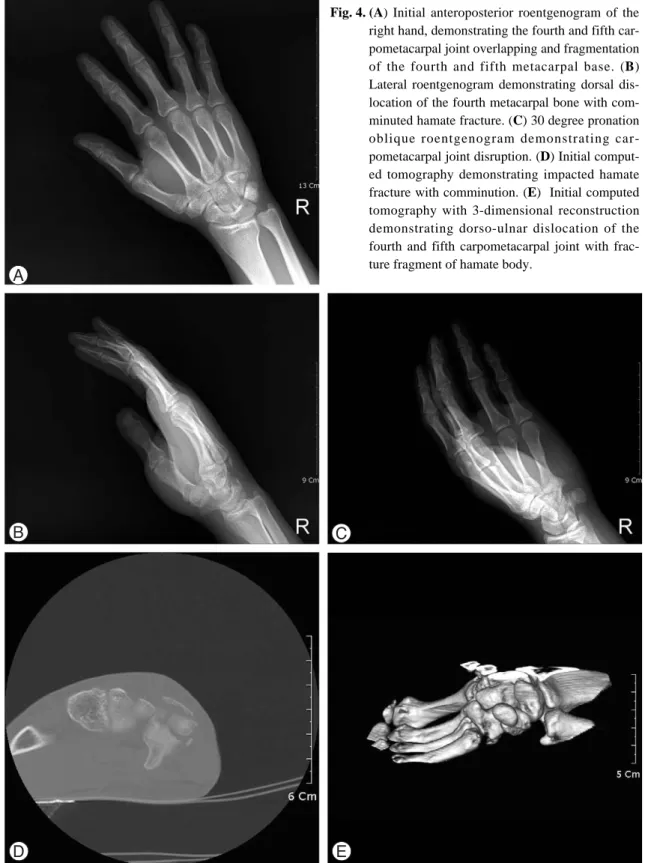
Fig. 4. (A) Initial anteroposterior roentgenogram of the right hand, demonstrating the fourth and fifth car- pometacarpal joint overlapping and fragmentation of the fourth and fifth metacarpal base. (B) Lateral roentgenogram demonstrating dorsal dis- location of the fourth metacarpal bone with com- minuted hamate fracture. (C) 30 degree pronation oblique roentgenogram demonstrating car- pometacarpal joint disruption. (D) Initial comput- ed tomography demonstrating impacted hamate fracture with comminution. (E) Initial computed tomography with 3-dimensional reconstruction demonstrating dorso-ulnar dislocation of the fourth and fifth carpometacarpal joint with frac- ture fragment of hamate body.
증례 2
우측 손잡이인 27세 남성이 계단에서 주먹을 쥔 상 태에서 넘어진 후 발생한 우측 수배부의 심한 동통 및 종창을 주소로 외래 진료 후 입원한 자로, 진찰상 우 측 수배부의 동통 및 종창 소견이 관찰되었고, 피부의 상처는 관찰되지 않았다. 수지 원위부의 감각이상이나 혈행 이상은 관찰되지 않았으나, 척측 수근관절부위의 심한 압통이 관찰되었다. 전후면, 사면, 측면, 30도 내회전 사면의 단순 방사선 상 제 4, 5 중수골 기저부 의 분쇄골절이 관찰되었고, 수근 중수 관절의 배측 탈 구가 측면상에서 명확히 관찰되었다. 이후 촬영한 컴 퓨터 단층 촬영상, 유구골 체부 배측의 견열 골절 소 견이 관찰되었고(Fig. 4A, B, C, D, E), Cain 등2 의 분류상 II형에 해당하였다. 내원 직후, 종축견인을 통한 도수정복을 시도하여 정복하였지만, 견인하지 않 으면 수근 중수관절의 탈구가 일어나는 불안정 골절로 판단되어 수술적 치료를 시행하였다. 영상 증폭 장치 하에 전완부의 회내전 상태에서 제 4, 5 수지에 종축 으로 견인력을 가하고, 수근 중수간 관절부위에 압박 을 가해 정복하고 유지한 상태에서, 제 4, 5 중수골 기저부에서 각각 유두골, 유구골로 K-강선을 삽입하 여 고정하였고, 수술후 수부의 내재근 양성 위치에서 단상지 석고고정을 시행하였다(Fig. 5A, B, C). 수 술 후 6주가 경과한 후 K-강선을 제거하였고, 술후 6 개월 후 통증 및 파악력의 회복을 만족할 만큼 얻을 수 있었다.
고 찰
수근 중수골 관절의 골절 및 동시 탈구는 수부의 손 상에 있어서 드물다고 알려져 있었으나, 최근의 연구 에서는 드물지 않은 손상으로1 적절한 시기의 진단 및 치료가 이루어지지 않는다면, 수상 후 동통 및 운동제 한을 야기할 수 있는 손상이다. 대부분 손상자체가 주
먹을 쥔 상태에서 직접가격에 의한 타격손상에 의하여 발생하며3, 외력의 방향에 따라 수장측 혹은 배측으로 의 탈구가 결정되며, 이는 강한 외력에 의해 손상 초 기 수부의 부종 및 동반 연부조직 손상이 있어 단순 타박상 및 염좌로 진단 되는 경우도 있고, 단순 방사 선 사진상으로 진단되지 못하여 진단 자체가 늦어지는 경우가 많다4. 이는 초기 진료에 있어서 진찰자의 세심 한 문진 및 진찰 그리고 방사선 검사에 대한 면밀한 판단이 필요할 것으로 사료된다.
방사선학적으로 본 증례에서 사용되었듯이, 수부의 전후면, 측면, 사면 등 3가지의 촬영이 기본적으로 필 수적이며, 특히 Bora와 Didizian은5 제 4,5 수근 중 수골의 기저부 및 수근관절부위의 경우 전완부를 전후 방 사진보다 30도 내회전하여 촬영할 경우 보다 정확 한 진단을 할 수 있다고 하였다. 방사선 사진상에서 Henderson 등은4 수근관절의 중첩 여부, 중수골의 단축, 그리고 관절면의 평행여부를 면밀히 관찰하면 진단에 도움이 된다고 밝힌 바 있다. 또한 중수골 기 저부의 분쇄 및 탈구에 대한 정확한 평가를 위해서 컴 퓨터 단층촬영이 도움이 되며 Hindman 등6은 컴퓨터 단층촬영의 유용성을 지적하였고 특히 중수골 기저부 의 골절을 평가하는데 관상면과 종축면상이 좋다고 한 바 있다.
수근 중수관절은 해부학적 위치에 따라 관절의 운동 성이 다양한데, 제 2, 3 수근 중수관절은 거의 운동성 이 없는데 반하여 제 4, 5 수근 중수관절은 Gunther 등7에 의해 각각 8도, 15도의 운동성을 가지는 것으로 밝혀진 바 있다. 또한 중수골 기저부의 관절면의 모양 역시 해부학적 위치에 따라 다양한데, 척측에서 요측 으로 갈수록 관절면이 오목한 모양을 이루고있다. 이 두 가지의 관절면의 해부학적 특징으로 인하여 외력이 가해졌을 때, 제 4, 5 수근 중수 관절이 다른 관절보 다 쉽게 손상이 가능하다고 사료되며, 순간적으로 강 한 외력이 작용하였을 때 동시에 탈구가 가능하리라 사료된다.
– 258 –
Fig. 5. (A, B, C) Postoperative anteroposterior, oblique and lateral roentgenogram shows restoration of the normal anatomical configuration of the carpometacapal joint after closed reduction and pinning.
수근 중수 관절의 골절 및 탈구의 치료에 대해서 Lawlis 등8은 관혈적 정복술이 비 관혈적 정복술보다 해부학적 정복이 가능하고, 조기에 관절운동이 가능하 다고 하였던 반면, Petrie와 Lamb은9 연부조직 손상 가능성이 있는 관혈적 정복술이 해부학적으로 미세 골 편을 정복하는 점에 대해 부정적인 견해를 피력한 바 있다. 결국 도수정복 후 불안정한 상태나 다발성 골절 혹은 골절 및 탈구, 그리고 개방성 손상과 같은 경우 에 관혈적 정복술이 타당할 것이라고 사료된다. 또한 Hartwig 등은10 연부조직의 심한 종창 및 골편이나 인대, 건 등의 관절면 내측으로의 감입 등 비관혈적 정복술이 불가능할 때 역시 관혈적 정복술을 고려해 볼 수 있다고 주장한 바 있다.
참고문헌
01) Fisher MR, Rogers LF, Hendrix RW. Carpometacarpal dislocations. CRC Crit Rev Diagn Imaging. 1994;22:95- 126.
02) Cain JE, Shelper TR, Wilson MR. Hamatometacarpal frac- ture-dislocation: Classification and treatment. J Bone Joint Surg Am. 1987;12:762-7.
03) Nalebuff, EA. Isolated anterior carpometacarpal disloca- tion of the fifth finger. Classification and case report. J Trauma. 1968;8:1119-23.
04) Henderson JJ, Arafa MAM. Carpometacarpal dislocation.
An easily missed diagnosis. J Bone Joint Surg Am.
1987;69:212-4.
05) Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am. 1974;56:1459-63.
06) Hindman BW, Kulik WJ, Lee G, Avoio RE. Occult frac- tures of the carpals and metacarpals: Demonstration by CT. Am J Rad. 1989;153:529-32.
07) Gunther SF. The carpometacarpal joints. Orthop Clin Am.1984; 15:259-77.
08) Lawlis JF. III, Gunther SF. Carpometacarpal dislocations:
Long-term follow-up. J Bone Joint Surg Am. 1991;73:52-9.
09) Petrie PWR, Lamb DW. Fracture-subluxation of base of fifth metacarpal. Hand. 1974;6:82-6.
10) Hartwig RH, Louis DS. Multiple carpometacarpal disloca- tions. A review of four cases. J Bone Joint Surg Am.
1979;61:906-8.