Journal of Korean Biological Nursing Science
12
0
0
전체 글
(2)
(3)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
수치

관련 문서
Key Words: Ischemic stroke; Thrombectomy; Brain; Reperfusion injury 국문주요어: 허혈성 뇌졸중, 혈전제거술, 뇌재관류 손상.. Corresponding author:
Key Words: Chronic obstructive pulmonary disease; airflow obstruction; health status; COPD assessment test 국문주요어: 만성폐쇄성폐질환,
Factors Associated with Obstructive Sleep Apnea Risk in Patients with Metabolic Syndrome.. Jae Hee Kim 1 , Sang
Effects of Laughing and Music Therapy on Depression and Activities of the Autonomic Nervous System in the Elderly with Dementia..
The Effects of Relaxation on Stress and Blood Pressure Induced by Cognitive Distress Game among College Students.. Mi Ryeong Song 1 , Sung
T he fall prevention program (FPP), web- based instruction, nursing education, cardiopulmonary resuscitation, basic nursing sciences, exercise (2), exercise test,
Relation of the Blood Pressure, Lipids and Body Mass Index by Smoking Status Among Adolescents.. A Study on Health behavior in People with type
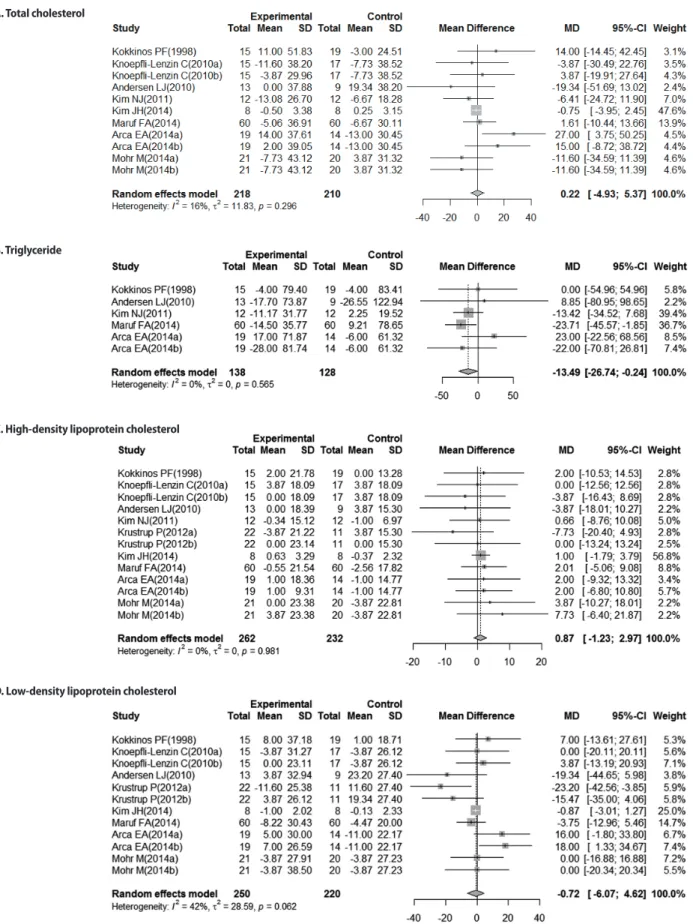
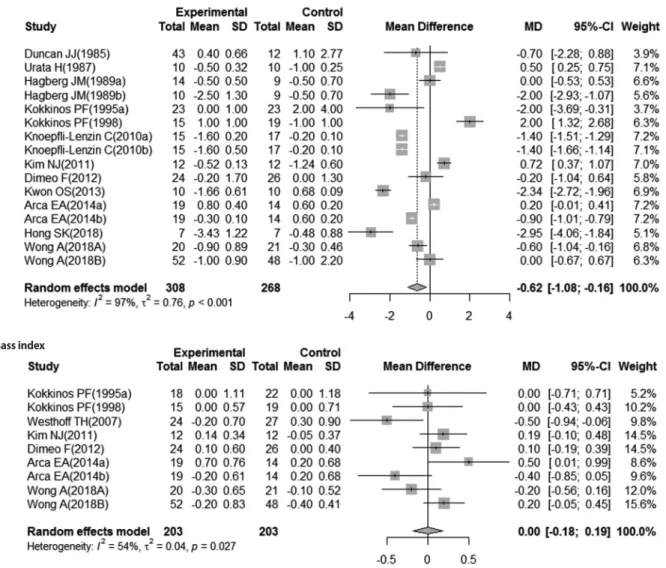
Purpose: This study was performed to identify the effects of dance sports programs on the parameters of health promotion (blood pressure, pulse, glucose, blood
