신증후군 환자에서 혈전에 의한 급성 심근경색증의 성공적인 Abciximab 치료
5
0
0
전체 글
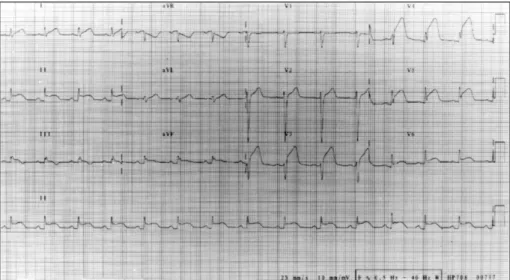
(2) 1). 이었다.. 표는 거의 없다.. 혈소판 당단백 IIb/IIIa 수용체 차단제인 Abciximab ®. 일반 화학검사는 정상 범위였고, 심근 효소 검사에서. (ReoPro )는 급성 관동맥 증후군에 효과적으로 사용되. troponin I 4.8 ng/mL, troponin T 5.27 ng/mL, creatine. 고 있으며 특히, 당뇨병이나 고위험군에서 경피적 관동맥. kinase(CK), CK-MB 481/97 U/L, myoglobn 207. 중재술(PCI:percutaneous coronary intervention) 결. ng/mL, aspartate aminotrnsferase 16 U/L, LDH 1820. 과를 향상시키고, 단기 및 장기간에서 심근경색증 및. mg/dL이었고, 혈청지질검사에서 total cholesterol 524. 사망률 감소에 효과적인 것으로 여러 대규모 연구를 통. mg/dL, high density lipoprotein-cholesterol 58 mg/dL,. 3-8). triglyceride 507 mg/dL, low density lipoprotein-. 해 밝혀지고 있다.. 저자 등은 MCNS으로 면역억제 요법을 받던 29세. cholesterol 366 mg/dL, apolipoprotein A1 166 mg/dL,. 남자 환자에서 좌전하행지의 다발성 혈전에 의한 급성. apolipoprotein B 247 mg/dL, lipoprotein(a) 61.9. 심근경색증이 발생하였음을 진단하고 구제적 풍선 성. mg/dL 이었으며, 혈중 albumin 1.4 g/dL, urine protein. 형술을 시행하던 중 Abciximab(ReoPro®)으로 관동맥. 11.8 g/day 였다. 혈액 응고 검사에서 prothrombin. 내 혈전을 성공적으로 치료한 경험을 보고하고자 한다.. time(INR) 1.07, activated partial thromboplastin time 39.5 sec 이었다. 그밖에 homocysteine 10.0 μmol/L,. 증. 례. erythrocyte sedimentation rate 12 mm/hr, C-reactive protein 0.564 mg/dL, fibrinogen 382.7 mg/dL. 28세 남자환자가 2시간동안 지속되는 흉통을 주소로. 이었고, rheumatoid arthritis factor 음성, antinuclear. 내원하였다. 10 갑년의 흡연자이었고 2년 전부터 미세 변. antibody titer 음성, anti-double strand DNA 2.8 IU/mL,. 화형 신증후군으로 cyclorosporin 150 mg과 atrovas-. anti-SM 항체 음성이었다. 감염 지표로서 Helicobacter. tatin 10 mg을 복용 중이었다. 생명징후는 혈압 110/70. pylori IgG 양성, Anti-cytomegalovirus(CMV) IgG. mmHg, 맥박수 분당 76회, 호흡수 분당 20회, 체온은. 195.1 AU/mL, Anti-CMV IgM 음성, Mycoplasma. 36℃이었다. 신체검사에서 급성 병색을 보였고 전신부. antibody 음성이었다.. 종은 없었다. 경정맥압은 정상이었고 양측 경동맥 및. 심전도에서 V3-6, Ⅰ, Ⅱ, Ⅲ, aVF lead에 저명한 ST. 복부 대동맥 등에서 잡음은 청진되지 않았으며, 심잡음. 분절 상승이 있었다(Fig. 1). 응급실에서 aspirin 300 mg,. 이나 폐 수포음은 청진되지 않았다. 환자는 체중 78 kg,. ticlipidine 500 mg을 복용하고 tissue type plasminogen. 키 169 cm로서 체질량 지수(body mass index)는 27.8. activator 100 mg으로 혈전용해요법을 시행 받았으나. Fig. 1. An electrocardiogram showed marked ST-segment elevations in the leads of V 3-6, I, II, III, and aVF on arrival at the emergency room.. 524. Korean Circulation J 2003;33(6):523-527.
(3) A. B. Fig. 2. A:even after a rescue percutaneous coronary intervention using repeated balloon angioplasties, coronary angiography revealed remained huge multiple thrombi within the proximal left anterior descending artery (LAD) with Thrombolysis In Myocardial Infarction (TIMI) flow I. B:after Abciximab (ReoPro®) administration, LAD flow was improved up to TIMI III with resolution of thrombus in the LAD.. 시행하였으나 음영 결손은 해결되지 않았다(Fig. 2A). 관상동맥 내로 100 μg의 nitrate, 2 mg의 nicorandil 등 을 수 차례 투여하였으나, 혈전으로 생각되는 음영 결손은 해결되지 않아서 Abciximab(ReoPro®)를 20 mg을 bolus로 정주하고 400 mg을 12시간에 걸쳐 주입하기 위해 시작하여 30분 경과한 후 실시한 관동맥 조영술에 서 음영 결손이 개선되기 시작하였다(Fig. 2B). 시술 후 심초음파도 검사에서 심첨부의 경한 운동 감 소 외에 특이사항이 없었고 이면성 심초음파도로 측정한 좌심실 구혈율은 66%였다. 환자에게 aspirin 200 mg, ticlipidine 500 mg, simvastatin 40 mg, nicorandil 10 mg 등을 복용 시키면서 퇴원 후 외래에서 관찰하였다. 퇴원 후 특이한 심장 증상은 없었으며 6개월째 시행한 추적 관동맥 조영술에서 관동맥 내 혈전은 관찰되지 않 았다(Fig. 3).. 고. Fig. 3. A 6-month follow-up angiogram showed no filling defects with good distal left anterior descending artery flow.. 찰. 신증후군은 혈전증의 위험도가 높은 질환으로 신증 증상 및 심전도상 ST 분절 상승이 지속되고 흉통이 지속. 후군에서 나타나는 과응고 경향과 고지혈증은 동맥경. 되어 관상동맥 조영술을 시행하였다. 근위부 좌전하행지. 화를 가속화하고 혈소판 응집을 증가시켜 관동맥 질환. 근위부에 혈전으로 생각되는 수개의 음영 결손이 관찰되. 의 발생 위험이 증가한다고 알려져 있다.. 었고 TIMI(Thrombolysis In Myocardial Infarction). 과응고 현상이 주된 것이며 고지질혈증, 스테로이드 투. flow Ⅰ 혈류를 나타내어 3.0 mm 풍선도자를 이용하. 여, 이뇨제 투여에 따른 저체액량 상태 등이 관여하는. 여 8 내지 12 기압으로 3차례 구제적 풍선 확장술을. 것으로 보고되었다.. 1)2). 혈전증은. 525.
(4) 신증후군 환자에서 과응고를 일으키는 정확한 기전 은 잘 알려져 있지는 않지만 antithrombin Ⅲ 결핍, protein C, S의 활성 이상, 섬유용해제 결핍, 혈소판 기 능 변화, 증가된 적혈구 접착능, procoagulant factor인 9-12). fibrinogen, factor Ⅷ의 증가 13). 가. 와 lipoprotein(a) 증. 등이 관여할 것으로 알려져 있다. 신증후군의 악. 화 시 야기되는 다량의 단백 소실은 Antithrombin Ⅲ 등의 소실과 다른 응고인자의 증가가 혈전 성향을 증가 14). 시킬 것으로 예상되었다.. 본 증례에서는 신증후군 치. 료를 위해 면역 억제제를 복용하며 저알부민혈증 상태였 으며, 혈청 지질검사에서 총콜레스테롤, 중성 지방, 저밀 도지단백 콜레스테롤, apolipoprotein B, lipoprotein(a) 가 현저하게 증가되어 있었으며, fibrinogen 수치도 증 가되어 관동맥 질환의 발생위험도가 높았다. 혈소판 당단백 IIb/IIIa 수용체는 collagen, thrombin, adenosine diphosphate 등에 의해 활성화된 혈소판에 서 형태 변화를 통하여 활성화되고 혈중에 용해되어 있 는 fibrinogen과 von Willebrand factor의 수용체로 작 용한다. Fibrinogen과 활성화되어 구조가 변화된 혈소 판 당단백 IIb/IIIa 수용체가 교차결합을 통하여 혈전이 형성된다. 따라서 혈소판 응집의 마지막 단계를 차단하 는 현재까지 알려진 가장 강력한 혈소판 응집 억제제인 당단백 IIb/IIIa 수용체 차단제인 Abciximab(ReoPro®) 은 급성 관동맥 증후군에 효과적으로 사용되고 여러 연 구를 통해 고위험군에서 관동맥 중재술 시술 결과를 향 상시킬 뿐 만 아니라 관동맥 내 혈전을 성공적으로 치 15-18). 료할 수 있다고 밝혀지고 있다.. 본 증례에서 급성 심근경색증이 신증후군 치료 중에 발생되었고 근위부 좌전하행지 관동맥에 다발성 거대 혈전이 혈전 용해제나 구제적 풍선확장술 후에도 용해 되지 않고 남아 있었으나 Abciximab(ReoPro®)을 사 용하여 효과적으로 치료할 수 있었던 예로서 신증후군 환자의 심근경색증 치료에 혈소판 당단백 IIb/IIIa 수용 체 차단제가 효과적임을 알 수 있었다.. 요. 약. 본 증례는 미세변화형 신증후군으로 치료 받고 있던 젊은 남자 환자에서 좌전하행지내 혈전에 의해 급성 심 근경색증이 발생되어 Abciximab(ReoPro®)을 사용하. 526. 여 효과적으로 치료하였던 예이다.. 중심 단어:심근경색증;혈전;혈소판;신증후군;중재술. REFERENCES 1) Ordonez JD, Hiatt RA, Killebrew EJ, Fireman BH. The. increased risk of coronary heart disease associated with nephritic syndrome. Kidney Int 1993;44:638-42. 2) Orth SR, Ritz E. The nephritic syndrome. N Engl J Med 1998;338:1202-11. 3) EPIC Investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in highrisk coronary angioplasty. N Engl J Med 1994;330:956-61. 4) EPISTENT Investigators. Randomized placebo-controlled and balloon angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein IIb/IIIa blockade. Lancet 1998;352:87-92. 5) Shim DS, Jeong MH, Kim W, Rhew JY, Yum JH, Kim JH, Cho JG, Ahn YK, Park JC, Ahn BH, Kim SH, Kang JC. Long-term clinical benefit of a platelet glycoprotein IIb/IIIa receptor blocker (Abciximab; ReoPro(r)) in diabetic patients undergoing high-risk percutaneous coronary intervention. Korean J Med 2002;62:171-81. 6) Kim W, Jeong MH, Kim KH, Park JC, Lee SH, Rhew JY, Kang KT, Kim NH, Ahn YK, Cho JG. The rescue use of platelet glycoprotein IIb/IIIa receptor blocker in high-risk patients with acute myocardial infarction underwent percutaneous coronary intervention. Korean Circ J 2001;31:492-9. 7) Zhao XQ, Theroux P, Snapinn SM, Sax FL. Intracoronary thrombus and platelet glycoprotein IIb/IIIa receptor blockade with tirofiban in unstable angina or non-Q-wave myocardial infarction. Circulation 1999;100:1609-15. 8) Gibson CM, de Lemos JA, Murphy SA, Marble SJ, McCabe CH, Cannon CP, Antman EM, Braunwald E. Combination therapy with abciximab reduces angiographically evident thrombus in acute myocardial infarction. Circulation 2001; 103:2550-4. 9) Rabelink TJ, Zwaginga JJ, Koomans HA, Sixma JJ. Thrombosis and hemostasis in renal disease. Kidney Int 1994; 46:287-96. 10) Zwaginga JJ, Koomans HA, Sixma JJ, Rabelink TJ. Thrombus formation and platelet-vessel wall interaction in the nephrotic syndrome under flow conditions. J Clin Invest 1994;93: 204-11. 11) Vaziri ND. Nephrotic syndrome and coagulation and fibrinlytic abnormalities. Am J Nephrol 1983;3:1-6. 12) Cruz C, Juarez-Nicolas F, Tapia E, Correa-Rotter R, PedrazaChaverri J. Abnormalities of coagulation in experimental nephrotic syndrome. Nephron 1994;68:489-96. 13) Tomas ME, Freestone A, Varghese E, Persaud JW, Moorhead JF. Lipoprotein(a) in patients with proteinuria. Nephrol Dial Transplant 1992;7:597-601. 14) Andrassy K, Ritz E, Bommer J. Hypercoagulability in the nephrotic syndrome. Klin Wochenschr 1980;58:1029-36. 15) Burzotta F, Hamon M, Sabatier R, Prati F, Boccanelli A, Grollier G. Large intracoronary thrombi with good TIMI flow during acute myocardial infarction: four cases of successful aggressive medical management in patients. Korean Circulation J 2003;33(6):523-527.
(5) without angiographically detectable coronary atherosclerosis. Heart 2002;88:e6. 16) Satler LF. Management of intracoronary thrombus in 2002. Catheter Cardiovasc Interv 2002;55:253-4. 17) Schlaifer JD, Horgan W, Malkowski MJ. Acute thrombotic occlusion of the left main coronary artery in a hypercoagulable patient treated with intracoronary abciximab. Clin Cardiol. 2001;24:788. 18) Jeong MH, Ahn YK, Park JC, Ahn BH, Na KJ, Kim NH,. Kim KH, Cho JG, Park JC, Kim SH, Kang JC. A case of successful primary coronary intervention for the total occlusion of left main stem with the aid of abciximab. J Korean Med Sci 2001;16:509-11.. 527.
(6)
수치

관련 문서