1
Dept. of Prosthodontics, KangNam St.Mary's Hospital, the Catholic University of Korea
2
Dept. of Prosthodontics, Graduate School of Clinical Dental Science, the Catholic University of Korea
Abstract
Introduction of implant dentistry brought out a new era in clinical dental practice. During the past 40 years, prosthetic rehabilitation of the edentulous patient with implant-supported prosthesis has been developed into a viable and predictable treatment option. However, successful dental implant treatment has been associated with rigid protocols advocating lengthy periods of undisturbed healing.
During the past two decades this traditional protocol has been questioned and numerous clinical studies have reported on the outcome of immediate loading of implants in various clinical situations. The concept of immediate implant loading has become popular due to reduced overall treatment time, decreased patient’ s anxiety and discomfort, high patient compliance and better function and esthetics. However, research and understanding in immediate implant loading are still controversial.
Therefore, the purpose of this review is to provide rationales for immediate implant loading, and summarize current avail- able literatures. Results from this review indicated that immediate implant loading achieved a similar high success rate as conventional delayed implant loading. However, a careful case selection, a proper treatment plan, suitable implant systems, and precise surgical techniques are essential for optimal outcomes when immediate implant loading is applied.
Key Words : immediate loading, implant prosthesis, literature review
Current status of immediate Implant loading - a literature review
Se-Hoon Kahm
1, Seok-gyu Kim
21
가톨릭대학교 의과대학 강남성모병원 치과보철과
2
가톨릭대학교 의과대학 임상치과학 대학원 치과보철학과
상
실된 치아와 치주조직을 회복하는데, 전통적으 로 가철성 의치와 고정성 보철물이 환자의 상실 된 저작, 발음, 심미를 향상시키는데 이용되어왔 다. 하지만, 환자들은 특히 가철성 보철물의 기능에 대해서 만 족하지 못하는 경우가 많았으나, 항상 고정성 보철물이 가능 하지는 않았다. 1970년대에 Bra ˚nemark과 동료들이 약 30 년 전에 치과 임프란트의 장기 치료에 대한 보고를 한 뒤, 임 프란트는 상실 치아의 수복 수단으로 널리 쓰이고 있다
1-3). 30여 년 전의 Bra ˚nemark의 술식을 요약해 보면, 다음과 같 이 정리할 수 있다
4).
Bra ˚nemark’ s protocol
• Machined titanium implants
• 2-stage procedure
• Stress-free healing period of 3 to 6 months
• Atraumatic surgery
• Sterile conditions
• Radiographs at completion of healing process
• Acrylic occlusal surfaces
이러한 부분 중 가장 강조되는 것은 수술 부위에 3-6개월 간의 부하가 없는 치유 기간의 부여였다. 치유 기간 동안에 부 하를 가하지 않음으로써 임프란트의 미세동요를 방지하고, 골융합(osseointegration)을 촉진시키고, 연조직의 침투를 방지하여 임프란트의 임상적인 실패를 막을 수 있었다. 그것 은 '지나치게 짧은 치유기간은 후기 임프란트 동요뿐만 아니 라 초기동요의 위험도 증가시킨다.'는 것을 확실히 입증한 임 상적 데이터에 기초하여, 오랫동안 임프란트 치료의 원칙으 로 자리 잡았다
4-8).
하지만, 이런 치유 기간 동안에 환자들은 주로 가철성 임시 수복물을 사용되게 되는데, 이는 유지와 안정이 떨어져서 환 자들에게 큰 불편을 주었다. 이러한 불편감을 극복하기 위해 서 치유 기간을 줄이고자 하는 노력이 많이 이루어졌고, 2회 수술법을 1회로 바꾸는 방법과 이를 위한 임프란트들도 개발 되었다. 이러한 방법에서도 다양한 증례보고에서 높은 임프 란트의 성공율을 보여주었다. 비단 그 뿐이 아니라 임프란트 의 부하시기를 앞당겨서 치료를 하는 술식도 선보였으며, 즉 시부하도 이러한 부분에서 나타나게 되었다
8-12).
Cochran은 2005년 제2회 Evidence-Based Dentistry Conference를 통해 임프란트 치료의 패러다임의 변화를 다 음과 같이 분류했다
13). 초창기인 1960-70년도에는‘Devel- opment period’ 로 볼 수 있고, 이 때에는 완전 무치악을 대 체하는 주요한 수단으로 이용되었다. 1980~90년도에는
‘Exploration period’ 로 점차 임프란트 치료가 부분 무치악 의 수복 수단으로써 가치가 증가하게 되었다. 2000년 이후에 는‘Refinement period’ 로 임프란트 제품의 발전과 치료의 최적화할 방법들이 개발되었다. 이러한 발전에 발맞추어서 즉시부하도 전부 무치악의 고정성 총의치를 사용하던 것에 서, 부분 무치악과 단일치의 고정성 보철물을 즉시부하 하는 것으로 점차 확대되고, 각 제조사에서 제공하는 부품들로 더 편리한 임프란트 치료를 할 수 있게 되었다.
본 종설에서는 다양하게 이용되고 있는 즉시부하에 대한 많 은 논문들을 토대로, 이가 가진 과학적, 임상적 근거에 대해 알아보고, 더 안전한 즉시부하를 하기 위한 방법과 가이드라 인을 되짚어 보고자 한다.
온라인 문헌 검색시스템인 pubmed를 이용한 검색에서
‘immediate loading’ 을‘title/abstract’ 로 가지는 dental
Ⅱ
I
journal을 조사하였다. 현재(2008년 6월 30일)까지 482건의 문헌이 보고되었다(Fig.1).
1989년 이전에는 즉시부하에 대한 문헌보고가 거의 없었 고, 1990년대에도 소수의 문헌보고만이 있었다. 2000년도 이후에서야 본격적인 연구가 이뤄졌고, 2002년 이후에 이르 러 문헌 보고가 폭발적으로 증가했다. 하지만, 대부분은 증례 에 관계된 문헌보고들이 많았다. 성공적인 즉시부하의 방법 과 가이드라인을 제시하기 위해서, 2000년 이후에 발표된 review article 38건을 바탕으로 하여 즉시 부하의 이론적, 경험적 근거를 간단히 되짚어 보고, 이의 적응증과 비적응증, 그리고 부분별 가이드라인에 대해서 알아보기로 하겠다.
Terminology
• Immediate occlusal loading - immediate occlusal loading within 2 2 w we ee ek ks s of implant insertion (JOI 2004, AAID 2003 congress, Misch et al.14))
• Immediate loading - no later than 72 hours (Aparicio et al. 200315); Cochran et al. 200416))
• Immediate loading - within 4 48 8 h ho ou urrs s (JOMI 200417), the Sociedad Espanola de Implantes
World Congress consensus meeting, ID 200618))
• Immediate implant loading - implant supported restoration is placed into occlusal loading within a
att lle ea as stt 4 48 8 h ho ou urrs s after implant placement (ICOI meeting at Naples, ID 200719))
• Immediate / direct loading - the provisional / definitive prosthetic construction is attached to the implant w wiitth hiin n 2 24 4 h ho ou urrs s of the implant being placed (Ostman 200820))
이전에는 2주 이상의 early loading을 immediate load- ing으로 분류하기도 했으나, 최근의 정의는 대체로 임프란트 식립 후 24~48 시간 이내에 임시 혹은 최종 보철물을 장착하 는 것을 뜻한다고 하겠다. 즉시부하는 수술 횟수를 감소시켜 주며, 전체적인 치료시간을 줄여줄 수 있으며, 더 좋은 연조직 치유를 기대할 수 있고, 환자의 전체 치료기간의 감소로 환자 의 내원횟수도 줄일 수 있다. 환자들에게도 저작기능의 제공 이 되고, 심미적, 형태적, 기능적으로도 만족스럽기 때문에 많은 장점이 있다. 단, 미세동요도가 증가될 수 있어서 임프란 트 실패가 증가할 수 있고, 연조직이나 경조직 반응을 정확히 Fig. 1. Trend of published articles per year concerning immediate loading.
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
예측하기 힘들어서 치료가 어려워질 수 있다(Table 1).
Historical background
Linkow 등이 1970년대에도 immediate loading에 대해 서 보고하고 임상 적용을 하기는 했지만
21,22), 대중적으로 널 리 이용된 것은 앞서 본 것과 같은 2000년도 이후의 일이라 할 수 있다. 1970년도에는 Bra ˚nemark의 2회법 시술이 일반 적인 치료였으며, 오히려 이러한 시도는 임프란트의 실패를 증가시키는 결과를 가져왔고, fibrous encapsulation을 막기 위해서“3~6개월의 부하가 없는 치유기간” 이 더욱 필요하다 고 생각하게 되었다
23,24).
이러한 분위기 속에서도 1980~90년도에 Chiapasco 등은 하악의 임프란트 피개의치의 즉시부하에서
25,26), Schnitman 등은 고정성 임시 의치로 즉시부하하여 90% 수준의 높은 성 공율을 보여주었다
27). 이후로 10여 년이 지나서야 임상의나 학회로부터 인정을 받기 시작한 치료 방법으로 자리 잡았다.
2005년에 발표한 Ioannidou 등의 13개의 prospective study를 바탕으로 한 meta-analysis에서 일반적인 치유기 간 이후의 보철수복과 즉시수복의 문헌 비교에서도 즉시부하 에서 약간의 실패율이 증가하는 경향이 있었으나, 이는 통계 적인 차이를 보이지 않았고, 두 치료는 모두 성공적이라 할 수 있겠다
28). 이는 임프란트 재료의 발전과 표면 처리 방식의 변
화, thread design의 개선 등을 통해서 더 편리하게 이용할 수 있게 되었다.
1997년 이후에 발표된 즉시부하의 문헌 보고 중에서 2년 이상의 follow up을 한 문헌들을 몇 가지 살펴보면, Chiapasco 등의 1997년의 retrospective study에서 2~13 년간 총 226명의 환자와 740개의 임프란트를 대상으로 한 누 적성공율이 96.9%였고
25), Tarnow 등이 1997년에 발표한 증 례보고에서 1~5년동안 10명의 환자, 69개의 임프란트의 누 적성공율이 100%에 이르기도 했다
29). 이후 2000년대에 발표 된 다수의 후향적, 전향적 연구에서도 93.5~99.7%에 이르는 높은 성공율을 보고했으며, Degidi와 Piattelli가 2005년에 보고한 7년간의 전향적 연구에서 93.5%의 높은 성공율을 보 여주었으며, 대다수의 이전 문헌 보고들과 같이 생존율 곡선 을 고려하면 즉시부하 초기나 부하 후 1년 이내에 실패가 많 았으며, 그 이후에는 실패가 증가하는 경향을 나타내지 않았 다
30). 반면에 machined surface를 이용한 보고의 수는 많지 않았으며, 특히 2년 이상의 보고는 그 수가 많지 않았다. 그리 고 machined surface 임프란트의 성공율은 85-98%로 다양 하게 나타났다.
Rough surface의 임프란트가 machined surface의 임프 란트보다 유사하거나 높은 성공율을 나타내는 것을 알 수 있 으며, 연구 자체의 숫자나 사용된 임프란트의 수도 훨씬 많음 Table 1. Advantage & disadvantages of immediate implant loading technique
31)A
Ad dv va an ntta ag ge e o off iim mm me ed diia atte e llo oa ad diin ng g D Diis sa ad dv va an ntta ag ge e o off iim mm me ed diia atte e llo oa ad diin ng g No second stage surgery(decreased morbidity) Increased micro-movement (higher failure rate)
Less waiting time(better soft tissue healing) Unable to predict final soft and hard tissue outcomes
Less patient visits
Monitoring of the implant during healing phase Higher patient acceptance
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
을 알 수 있었다
29,30,32-39). 이는 임프란트 표면 처리나 디자인 등의 개선이 즉시부하의 적용이 다양해지는데 일조했다고 보 겠다. 임프란트 표면처리나 디자인의 향상은 즉시부하 성공 의 주요한 요인 중 둘인‘Primary stability’ 와‘Secondary stability’ 의 큰 도움이 되었기 때문이다(Table 2 and 3).
Where can we apply immediate loading?
초창기에 즉시부하는 완전 무치악에서 임시의치를 고정시 키는데, 주로 사용된 술식이었다. Hybrid type과 같이 완전 무치악에서 고정성 총의치를 만드는데 사용되거나, 피개의치 의 지대치로 사용된 경우가 많았다. 이러한 술식은 임프란트
의 초창기부터 사용되어왔으며, Schnitman 등이 1997년에 발표한 Bra ˚nemark 임프란트를 이용한 하악 완전 무치악을 고정성 수복물로 즉시부하한 후향적 연구에서 85.7%의 성공 율을 보여주었고
40), 이후에 발표된 Bra ˚nemark 등의 1999년 연구는 완전 무치악인 하악에서 3년간 98%의 성공율을 나타 냈으며
38), 2000년도 이후에는 대부분의 문헌보고에서 완전 무치악인 하악에서는 93% 이상의 높은 성공율을 보여주었다 (Table 4).
통상적으로 하악에 비해서 골질이 불리한 것으로 여겨지는 상악에서도 연구들이 진행되었는데, Grunder 등이 2001년 에 발표한 전향적 연구에서 1~5년 간의 임상경과 관찰에서 5 Table 2. Immediate implant loading of splinted prosthesis on the rough implant surface
31)A
Au utth ho orrs s T Ty yp pe e o off N No o.. o off N No o..o off P Pe erriio od d o off S Su uc cc ce es ss s ((Y Ye ea arr)) S Sttu ud dy y P Pa attiie en ntts s iim mp plla an ntts s S Sttu ud dy y((y yrrs s)) R Ra atte e C
Ch hiia ap pa as sc co o e ett a all.. (1997) Retrospective 226 740 2 to 13 96.9%
T
Ta arrn no ow w e ett a all.. (1997) Case reports 10 69 1 to 5 100.0%
G
Ga attttii e ett a all.. (2000) Prospective 21 84 2 to 5 96.0%
G
Ga an ne elle es s e ett a all.. (2001) Retrospective 27 161 1 to 3.3 99.0%
T
Te es stto orrii e ett a all.. (2003) Retrospective 15 103 4 98.9%
T
Te es stto orrii e ett a all.. (2004) Prospective multicenter 62 125 1 to 5 99.4%
D
De eg giid dii e ett a all.. (2005) Retrospective 43 388 5 99.7%
D
De eg giid dii & & P Piia atttte ellllii (2005) Prospective 11 93 7 93.5%
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
Table 3. Immediate implant loading of splinted prosthesis on the smooth implant surface
31)A
Au utth ho orrs s T Ty yp pe e o off N No o.. o off N No o..o off P Pe erriio od d o off S Su uc cc ce es ss s ((Y Ye ea arr)) S Sttu ud dy y P Pa attiie en ntts s iim mp plla an ntts s S Sttu ud dy y((y yrrs s)) R Ra atte e T
Ta arrn no ow w e ett a all.. (1997) Case reports 10 69 1 to 5 85.0%
B
Brra
˙˙a
˙˙n ne em ma arrk k e ett a all.. (1999) Prospective 50 150 0.5 to 3 98.0%
C
Ch hiia ap pa as sc co o e ett a all.. (2001) Prospective 20 40 2 97.5%
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
명의 환자, 48개의 임프란트에서 6개의 임프란트가 실패해서 임프란트의 누적성공율이 87.5%로 나타났다
41). 단, 이 보고 에서도 보철물은 임프란트가 실패하더라도 보철물의 성공율 은 100%로 나타났다. Grunder 등의 연구를 제외한다면, Tarnow
29), Horiuchi
42), Degidi
30,35), Fischer
43,44)등의 전 향적, 후향적 연구에서 97~100%의 높은 임프란트 성공율을 보고하였다(Table 5).
이러한 완전 무치악의 경우에 무치악의 위치가 상악이거나
하악이거나에 관계없이 대부분의 문헌 보고에서 94% 이상의 높은 성공율을 보여주었다. 단지, 장기간의 관찰기간은 완전 무치악인 하악 증례에서 더 많이 보고되고 있으며, 상악의 경 우에는 관찰기간이 짧은 경향이 있으나, 다수의 증례보고나 문헌보고에서 양측성으로 6개 이상의 다수의 임프란트를 식 립하고, 양측성 연결고정을 할 경우에는 높은 성공율을 보여
주었다
33,34,38,40-44,46-48). 이러한 완전 무치악증례에서 고정성
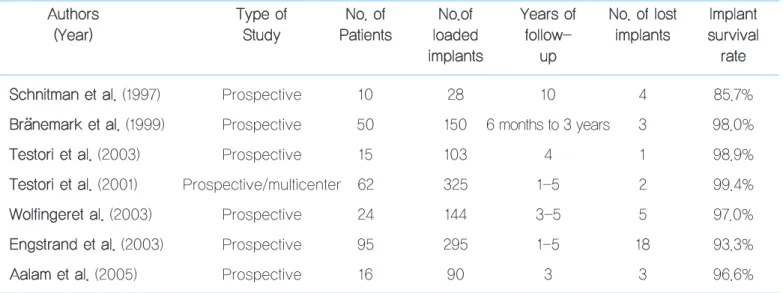
보철물의 지대치로써 임프란트의 사용이 증가됨에 따라서 다 Table 4. Immediate loading with fixed prosthesis in the totally edentulous mandible
45)A
Au utth ho orrs s T Ty yp pe e o off N No o.. o off N No o..o off Y Ye ea arrs s o off N No o.. o off llo os stt IIm mp plla an ntt ((Y Ye ea arr)) S Sttu ud dy y P Pa attiie en ntts s llo oa ad de ed d ffo ollllo ow w- - iim mp plla an ntts s s su urrv viiv va all iim mp plla an ntts s u up p rra atte e S
Sc ch hn niittm ma an n e ett a all.. (1997) Prospective 10 28 10 4 85.7%
B
Brra
˙˙a
˙˙n ne em ma arrk k e ett a all.. (1999) Prospective 50 150 6 months to 3 years 3 98.0%
T
Te es stto orrii e ett a all.. (2003) Prospective 15 103 4 1 98.9%
T
Te es stto orrii e ett a all.. (2001) Prospective/multicenter 62 325 1-5 2 99.4%
W
Wo ollffiin ng ge erre ett a all.. (2003) Prospective 24 144 3-5 5 97.0%
E
En ng gs sttrra an nd d e ett a all.. (2003) Prospective 95 295 1-5 18 93.3%
A
Aa alla am m e ett a all.. (2005) Prospective 16 90 3 3 96.6%
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
Table 5. Immediate loading with fixed prosthesis in the totally edentulous maxilla
45)A
Au utth ho orrs s T Ty yp pe e o off N No o.. o off N No o..o off Y Ye ea arrs s o off N No o.. o off llo os stt IIm mp plla an ntt ((Y Ye ea arr)) S Sttu ud dy y P Pa attiie en ntts s llo oa ad de ed d ffo ollllo ow w- - iim mp plla an ntts s s su urrv viiv va all iim mp plla an ntts s u up p rra atte e T
Ta arrn no ow w e ett a all.. (1997) Prospective 4 14 1-4 0 100.0%
H
Ho orriiu uc ch hii e ett a all.. (2000) Prospective 5 44 1-2 2 97.0%
G
Grru un nd de err e ett a all.. (2001) Retrospective 5 48 1-5 6 88.0%
D
De eg giid dii e ett a all.. (2005) Retrospective 43 388 5 8 98.0%
F
Fiis sc ch he err e ett a all.. (2006) Prospective 24 139 3 0 100.0%
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
양한 증례에서 임프란트의 즉시 부하 가능성이 높게 점쳐졌 으며, 부분 무치악과 단일치의 수복에서도 즉시 부하 증례에 의 적용을 고려할 수 있게 되었다. 완전무치악과 같은 양측성 연결고정은 할 수 없을지라도, 미세동요를 방지할 수 있는 안 정적인 인접면 접촉이나, 교합면의 수평적인 부하를 피할 수 있는 설계, 좋은 초기 안정성이 있다면 부분 무치악이나 단일 치에서도 그 가능성은 충분하다고 할 수 있겠다.
부분 무치악에 대한 보고는 5년 이상의 장기간의 문헌 보고 는 없었다. 대부분의 문헌 보고는 1년 정도의 후향적 연구였 으며, 성공율은 90~98.4%까지 상당히 높은 성공율을 보여
주었으며
49-52), 이는 5년에서 94~96%를 보여주는 완전 무치
악 증례의 임프란트 성공율과 크게 차이가 나지 않는 부분이 라 할 수 있다. 특히 환자의 drop-out이 많긴 했지만, Ostman 등의 2008년에 발표한 연구에서 4년까지의 경과관 찰에서 98.4%의 누적성공율을 보인 것은 고무적이 일이라 할 수 있겠다
45,53). 앞으로 장기간의 데이터가 모아진다면, 치료 에 대한 근거를 더 마련할 수 있을 것이다(Table 6).
단일치 수복에서 즉시부하의 적용에 대해서는 가장 긴 관찰 기간을 가진 보고가 Degidi와 Piattelli 등이 2006년에 발표 한 retrospective study로 5년 동안 111명의 환자 총 111개의 임프란트에서 5개 실패하여 누적성공율이 95.5%한 보고였으
며
54), 이 보고를 제외하면 3년이 가장 긴 관찰이었고, 보통 1 년에서 1년 반 정도를 관찰하였다
55-59). 이러한 단기적인 성공 율에서도 81~100%의 많은 편차를 보였으며, 단일치 수복에 서 즉시부하를 표준적인 치료법으로 생각해 보기에는 아직은 문제가 있을 수 있겠다. 하지만, 환자와 증례를 잘 선택해서 치료를 한다면, 적절한 치료로 자리 잡을 수 있을 것이고, 이 에 대한 방법은 이후에 다시 알아보기로 하겠다(Table 7).
앞서 살펴본 implant immediate loading은 상당히 높은 성공율을 나타내었다. 이는 기존의 치유기간을 기다린 임프 란트의 성공율과 많은 차이를 나타내지는 않는다. 기존의 방 법과 비교된 문헌들을 살펴보면, Ioannidou와 Doufexi의 13 개의 기존 지연 부하 방법과 임프란트 즉시나 조기 부하를 가 해 비교한 13개의 prospective study(1266개의 임프란트)의 meta-analysis에서 약간의 실패율이 증가하는 경향을 나타 내더라도 이는 통계적인 차이를 나타내지 않았다고 한다. 또 한, 이가 임프란트 실패에 큰 영향을 주거나 위험요소가 되는 것으로 나타나지는 않았다
60).
최근 Susarla 등의 연구에 따르면, 지연부하를 한 677명 (2349개의 임프란트)과 즉시부하를 한 178명(477개의 임프 란트)의 1년 간 임프란트의 생존율을 비교한 연구에서 지연부 하 임프란트가 95.5%, 즉시부하 임프란트가 90.3%로 나타났 Table 6. Immediate loading with fixed prosthesis in the partially edentulous maxilla/mandible
45)A
Au utth ho orrs s T Ty yp pe e o off N No o.. o off N No o..o off Y Ye ea arrs s o off N No o.. o off llo os stt IIm mp plla an ntt ((Y Ye ea arr)) S Sttu ud dy y P Pa attiie en ntts s llo oa ad de ed d ffo ollllo ow w- - iim mp plla an ntts s s su urrv viiv va all iim mp plla an ntts s u up p rra atte e R
Ro oc cc cii e ett a all.. (2003) Prospective 22 55 1 3 95.5%
O
Os sttm ma an n e ett a all.. (2008) Prospective 77 257 1-4 4 98.4%
S
Sc ch hiin nc ca ag glliia a e ett a all.. (2007) Prospective 20 44 1 2 95.0%
C
Co orrn ne elliin nii e ett a all.. (2006) Prospective 20 40 1 1 97.5%
M
Ma ac ch htte eii e ett a all.. (2007) Prospective 20 49 1 5 90.0%
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
으며, 이는 즉시부하가 임프란트 실패에 영향을 어느 정도 줄 수 있음을 시사한다. 이외에 흡연, 상악구치부, 짧은 임프란트 의 사용 등이 임프란트 실패에 영향을 줄 수 있다고 하였다
61). 이 논문만을 살펴본다면 부정적인 견해를 가질 수도 있으나, 통상적인 치유기간을 가진 임프란트의 성공율은 일반적인 90~100% 범위에 있으므로, 앞서 살펴본 완전/부분 무치악 임프란트 즉시부하와 단일치 임프란트 즉시부하에서조차도 실패에 결정적인 인자가 아니며, 특정한 조건을 만족하는 하 에서는 안정된 치료방법이라고 생각해 볼 수 있다.
Histological and biological background
임프란트의 성공에 대해서 평가를 하는 기준은 다양하지 만, 임상적으로 흔히 측정할 수 있는 누적생존율의 계산이나 변연골 흡수의 측정, 임프란트주위염의 존재 유무, 그리고 ISQ 값의 측정 등은 비침습적인 방법으로 좋은 평가 기준이 된다. 하지만, 임프란트가 골과 직접 접촉하여서 어떠한 반응 을 가지고 있는지 가장 확실하게 평가할 수 있는 방법은 임프 란트와 골이 접촉을 어떻게 하고 있는지, 얼마만큼의 양을 접 촉하는지, 골의 성숙도는 어느 정도인지 직접적으로 평가해 보는 조직형태학적인 연구가 가장 정확한 방법이 될 수 있다.
인체에서는 이러한 연구가 진행되는 것은 침습적이며, 관혈 적인 술식이기 때문에, 많은 연구가 이루어지지는 않았고, 여 기에 대해서는 주로 동물실험이 많이 이용되었고, 간간이 사 체에서 발거된 임프란트나 환자의 요구로 임프란트를 제거한 경우에 이뤄진 연구가 있었다
62-66).
Nkenke 등이 2003년에 발표한 minipig를 이용한 연구에 서 BIC, bone area, bone mineral apposition rate를 즉시 부하한 임프란트와 지연부하한 임프란트에서 비교를 하였는 데, 두 그룹 간의 통계적으로 유의한 차이를 나타내지 않았다.
BIC를 제외한 수치에서는 약간씩 즉시부하군이 높게 나오기 도 했고, 특히, 즉시부하군의 bone mineral apposition rate 는 42~98일 구간에서 높은 수치를 보였다. 즉시부하가 지연 부하와 거의 동일한 결과를 나타내고, 골침착에 있어서는 더 유리한 점이 있는 가능성을 밝힌 것으로 의미가 있을 수 있겠 다. 이외에도 다수의 동물실험에서 즉시부하가 지연부하와 차이가 없거나 일부분에서 골에 자극을 가해 더 좋은 결과를 보이기도 했다
67)(Fig.2).
Degidi 등이 2005년에 발표한 하악 구치의 soft bone에서 2개월의 임프란트 즉시부하 후 환자의 불편감으로 발거한 임 프란트 주위의 골조직을 조직학적으로 평가하였는데, BIC가 Table 7. Immediate loading with single restorations in the maxilla/mandible
45)A
Au utth ho orrs s T Ty yp pe e o off N No o.. o off N No o..o off Y Ye ea arrs s o off N No o.. o off llo os stt IIm mp plla an ntt ((Y Ye ea arr)) S Sttu ud dy y P Pa attiie en ntts s llo oa ad de ed d ffo ollllo ow w- - iim mp plla an ntts s s su urrv viiv va all iim mp plla an ntts s u up p rra atte e
Ericsson et al. (2002) Prospective 14 14 1 2 86.0%
Hui et al. (2001) Prospective 24 24 1-15 months 0 100.0%
Calandriello et al. (2003) Prospective 44 50 6-12 months 0 100.0%
Rocci et al. (2003) Retrospective 27 27 3 5 81.0%
Lorenzoni et al. (2003) Retrospective 12 12 1 0 100.0%
Degidi & Piatelli. (2006) Retrospective 111 111 5 5 95.5%
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
71%로 나타났다. 비록 soft bone일지라도 즉시부하의 적용 시에 2개월 치유 및 부하기간에서 골치유에 문제가 없었음을 보여 주었다
66).
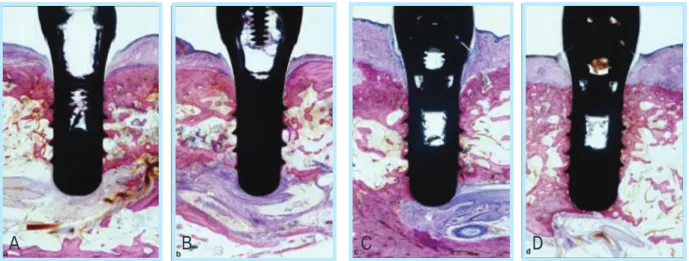
Quinlan 등의 2005년도 연구에 따르면, 개의 하악에서 각 각 부하시기를 달리하여 2일, 10일, 21일, 3개월로 하여, BIC 를 primary bone과 secondary bone(신생골)로 비교하고, total bone, bone marrow, connective tissue를 비교하였 다. 특이한 점은 신생골의 부하시기를 앞당긴 2일차에 부하를 시작한 군이 신생골의 양이 가장 많았다. 또한, connective tissue의 양도 비교를 해보면, 골의 생성이 더 많고, connec- tive tissue의 생성된 양이 적음으로 즉시부하를 한 군에서 더 좋은 결과를 보였다
68). 즉시부하를 가하는 것이 골치유에 더 도움이 될 수 있음을 시사한다. 여기에 대해서는 적절한 부 하의 양과 치유기간에 대해서 연구가 더 필요할 것이다
68)(Fig.3 and 4).
Luigi Guida 등의 2008년 연구에서는 대칭되는 두 치아를 발거해야 하는 환자에서 발치 후 즉시 임프란트 식립 후, 두 치아 중 하나에만 즉시부하를 가하고, 다른 하나는 치유 지대
주를 연결하여 치유기간을 준 뒤, 6개월 뒤 두 임프란트를 제 거하여 조직형태학적 평가하였다. 치유기간을 준 군에서 58%의 BIC를, 즉시부하군에서 52%의 BIC를 나타냈다. 수치 는 통계학적인 차이를 보이지 않았고, 오히려 즉시부하를 가 한 임프란트 주위에서 더 치밀하고 잘 성숙된 골이 발견되었 다
69). 즉시 발치 후 즉시 부하가 치유에 영향을 미치지 않는 것으로 생각되며, 오히려 적절한 부하가 치유에 긍정적으로 작용하는 것에 대해 생각해 볼 수 있겠다.
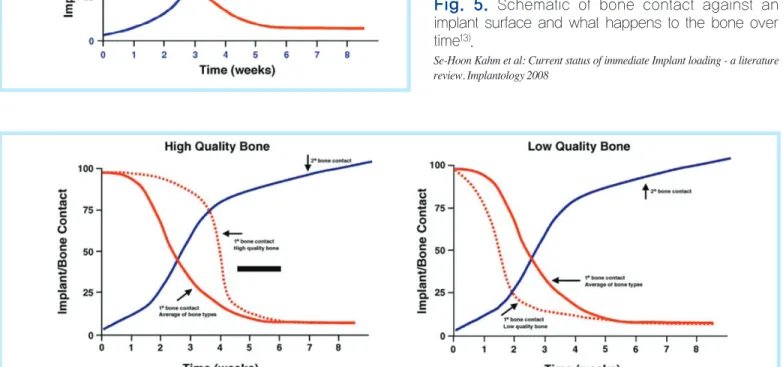
이전의 임프란트 치료와는 많은 점들이 변화했는데, 임프 란트의 osseointegration의 개념도 정적이며 안정된 것이 아 니라, 동적인 개념으로 변화하게 되었다. Cochran 등이 2006년 2nd Evidence-Based Dentistry Conference에서 새로운 정의로‘Stability of an implant in bone that rep- resents a dynamic equilibrium between existing native bone (primary contact) and remodeling and new bone formation (secondary contact) and it’ s maintenance at the bone-implant interface’ 로 생각하게 되었다. 이러한 접촉은 다음 그림과 같이 생각해 볼 수 있으며, 골질이나 골양 Fig. 2. Histomorphometric analysis(left) and Fluorescence labels(right). a, distance between outer bor-
der of first oxytetracycline label and xylenol orange label; b, distance between xylenol orange label and alizarine-complexon label; c, distance between alizarine-complexon label and second oxytetracy- cline label
67).
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
에 따라서 차이가 날 수 있고, primary bone contact과 secondary bone contact의 합으로 osseointegration을 생 각해 볼 수 있다
13,70,71)(Fig.5 and 6).
따라서 골질이 우수한 곳에서는 지연부하를 선택하더라도 이른 시기에 할 수 있으며, 골질이 불량한 곳에서는 그 시기를 늦춰야 할 수 있다. 이러한 골질에 대한 고려사항은 성공적인
즉시부하를 위한 고려사항에서 다시 언급하도록 하겠다.
‘Stability dip’ 이 나타나는 구간이 2~4주 사이 구간이므로 전체적인 stability가 상당히 뛰어난 식립 후 즉시부하는 생물 학적인 bone의 생리에도 상당히 합당한 부분이 많이 존재하 며, 이를 어중간한 early loading을 가하는 것보다 훨씬 안전 하고 우수한 보철수복 방법이라고 할 수 있다
13,70,71)(Fig.7).
Fig. 3. Quinlan’ s histologic cross-sections of implants from a) Group A : 3months, b) Group B : 21 days, c) Group C : 10 days, d) Group D : 2 days after 3 months of loading
68).
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
Fig. 4. Bone-to-implant contact and Tissue-to-implant contact between tissue and primary and secondary bone, bone marrow, and connective tissue for Groups A(3months), B(21days), C(10days), and D(2days)
68).
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
A B C D
Fig. 5. Schematic of bone contact against an implant surface and what happens to the bone over time
13).
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
Fig. 6. The change in primary bone contact when an implant placed in a site with a large proportion of dense bone such as cortical bone or less dense bone such as cancellous bone
13).
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
Fig. 7. The stability of an implant placed in high quality bone is large or less and stability dip
13).
Se-Hoon Kahm et al: Current status of immediate Implant loading - a literature review. Implantology 2008
Guidelines for successful immediate loading
앞서 살펴본 바와 같이 임프란트의 즉시부하는 환자와 술자 에게 많은 장점을 가져다 줄 수 있는 치료이다. 하지만, 이는 임프란트 실패율의 증가를 가져올 수 있는 양날의 검이기도 하다. 이러한 즉시부하를 성공적으로 하기 위해서 제안된 방 법들을 살펴보기로 하자.
1990년대에는 다른 생각을 가지고 있었는데, 1997년 Tarnow의 발표에서는 다음과 같은 가이드 라인을 제시했다
29).
1. Immediate loading should be attempted in edentu- lous arches only to create cross-arch stability.
2. Implants should be at least 10 mm long.
3. A diagnostic wax up should be used for template and provisional restoration fabrication.
4. A rigid metal casting should be used on the lin- gual aspect of the provisional restoration.
5. A screw-retained provisional restoration should be used where possible.
6. If cemented, the provisional restoration should not be removed during the 4~6 months healing period.
7. All implants should be evaluated with Periotest at staged 1, and the implants that show the least mobility should be selected for immediate loading.
8. The widest possible anterior-posterior distribution of implants should be utilized to provide resistance to rotational forces.
9. Cantilevers should be avoided in the provisional restoration.
당시에는 부분 무치악이나 단일치 수복에서의 즉시부하에 대해서는 생각을 할 수 없었던 시기여서 처음부터 양측성으 로 고정하여 초기 안정성을 높이는 부분을 강조했으며, Periotest를 이용한 동요도 여부를 검사의 한 기준으로 삼았 다. 하지만, 이제는 더 다양하고 더 많은 부위에서 즉시 부하
를 가할 수 있다고 생각하며, 비록 단일치에서는 아직 더 장기 간의 관찰이 필요할지라도 잘 설계된 치료 계획을 가진다면, 성공적인 치료를 할 수 있을 것이다. 이러한 변화된 부분에서 어떠한 치료 기준을 세울 것인가에 대해서 생각해 보자
31,45,72-79)