Dept. of Oral and Maxillofacial Surgery, Section of dentistry, Seoul National University Bundang Hospital, Korea
Abstract
Purpose: The implant surface would be exposed during healing period by several causes as marginal bone resorption and inadequate drilling. Implant surface exposure can cause accumulation of plaque and microbials around implant and can develop peri-implantitis. Therefore, surgeon should be fully aware of adequate management of exposed surface of implant.
This study aimed to evaluate the result of various treatment on exposed surface of implant.
Material and methods: A retrospective chart review and radiologic analysis were conducted of 25 fixtures among 14 patients(male 9, female 5) during period from June 2007 to January 2008. We evaluated implant survival rate, soft tissue index and marginal bone loss after functional loading.
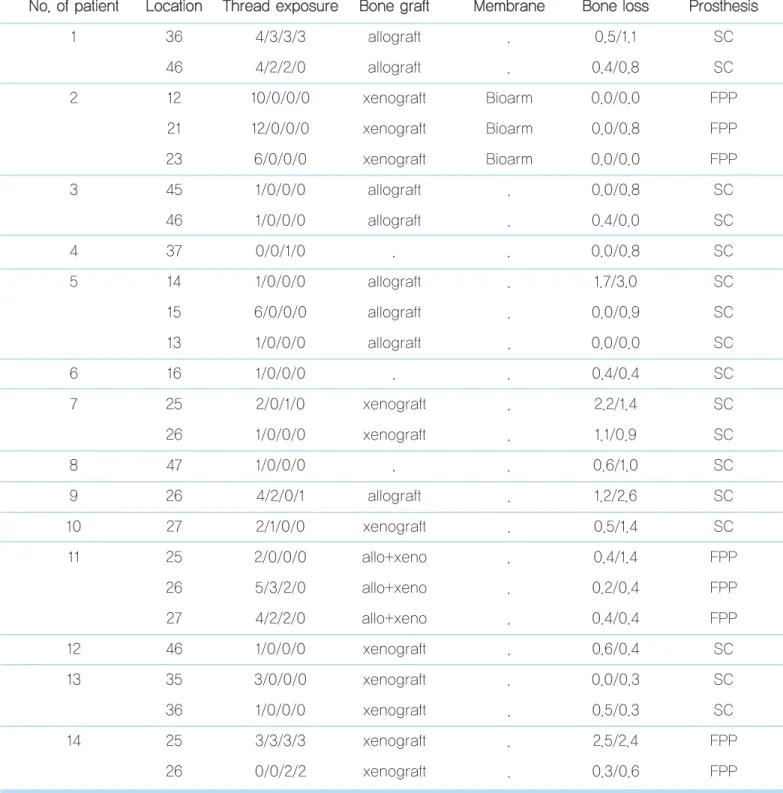
Results: In second surgery, measurement of implant thread exposure was 3.04mm ± 2.97 on buccal, 0.36 ± 0.9mm on lin- gual, 0.64 ± 1.11mm mesial, 0.64 ± 1.03mm distal in average. In 25 cases, bone graft was done on exposed area in 22 cases.
Allograft mixed with alloplast was used in 3 cases. Xenograft was used in 11 cases. And alloplast was used in 8 cases. The cases showed 100% survival rate and functioned stably during follow-up period.
Conclusion: We suggest that implant with exposed surface can function successfully with adequate treatment.
Key Words: thread exposure, bone graft
Treatment of implant with exposed threads during second surgery
Ji-Young Lee, Young-Kyun Kim
2차 수술 시 노출된 임프란트 나사산에 대한 처치
이지영, 김영균
분당서울대학교 병원 치과 구강악안면외과
부
적절한 위치의 임프란트 식립, 불량한 골질 및 골 양등은 식립된 임프란트 표면의 조기 노출의 원 인이 될 수 있다. 또한 일차 수술 시 임프란트 표 면이 노출되거나 골 접촉이 부족했던 경우 등에서 임프란트 의 변연골 흡수가 가속화 되어 조기 노출이 야기 될 수 있다.
이러한 조기 노출이 반드시 임프란트 실패와 연결되는 것은 아니지만, 치태 및 세균의 침착이 심화될 수 있고 지속적인 골 흡수와 임프란트 주위염으로 이어질 가능성이 높다.
1)따라서 술자는 노출된 임프란트 표면에 대한 적절한 처치 및 관리에 대해 숙지 할 필요가 있다. 본 연구에서는 2차 수술 시 노출된 임프란트 나사산에 대한 다양한 처치 증례 및 임프란트 생존 률, 보철 후 골 흡수 등에 대한 결과를 보고하고 이차 수술 시 노출된 나사산의 처치 방법 및 그 적응증에 대해 고찰 해 보고 자 한다.
2007년 6월 부터 2008년 1월 까지 분당서울대학교병원 치 과에서 1인의 치과의사에게 임프란트 시술을 받은 후 2차 수
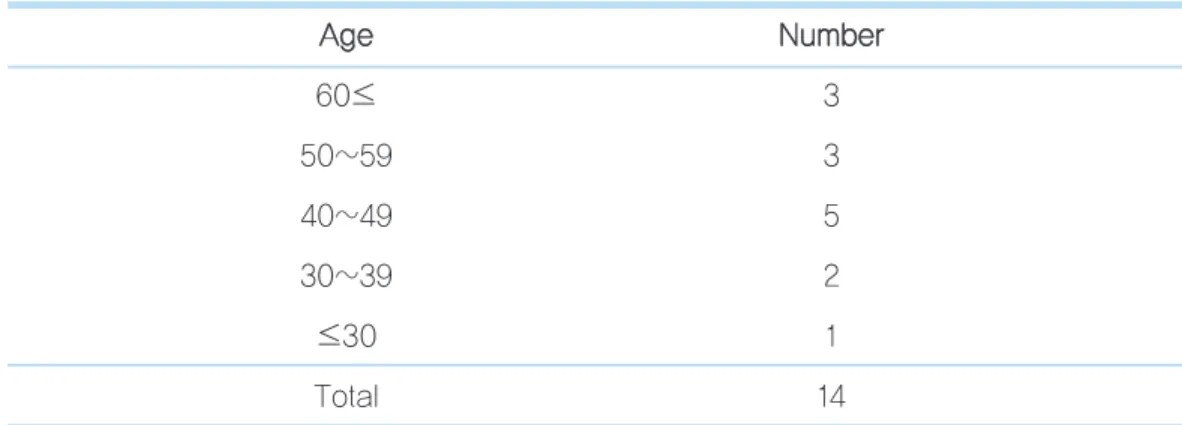
에서 2차 수술 시 나사산 노출이 관찰 되었다. 대상은 남자가 9명, 여자 5명이었으며 환자들의 나이는 21세부터 66세까지 로 평균 46.5세였다(Table 1, 2). 총 6명의 환자가 수술에 영 향을 미칠 수 있는 전신 질환을 보유하였으며 이 중 2명의 환 자는 2가지 이상의 전신질환을 보유하고 있었다. 전신 질환은 고혈압, 당뇨병, 심장질환, 갑상선질환, 간질환 등이었고 모 두 내과적으로 잘 조절 되었다. 흡연가는 1명이 있었다(Table 3). 평균 경과 관찰 기간은 13개월이었고 보철 후 6개월 이상 지난 증례들을 대상으로 하였다. 1차 수술 후 치유기간은 최 소 3개월에서 최대 5개월로 평균 4개월이었고, 2차 수술 후 보철물 제작까지의 기간은 최소 17일에서 최대 5개월로 평균 2개월 이었다. 2mm 이상 나사산이 노출된 증례에서 골이식 을 시행하였으며 1mm 노출된 증례는 골이식을 시행하지 않 았으나 예외적으로 협측에서 나사산이 노출된 증례는 골이식 을 시행하였다.
증례별로 사용된 임프란트의 길이 및 직경, 각 부위별 노출 된 정도, 최종 보철물 장착 후 주변조직 상태, 술 후 합병증, 노출된 부위의 처치 방법 등을 평가하였다. 그리고 1차 수술, 2차 수술, 보철 6개월 후 방사선 사진을 촬영하여 임프란트 변연골의 흡수 정도를 평가하였다. 변연골의 흡수는 평행 촬 영법으로 촬영된 치근단 방사선 사진상 임프란트 shoulder에 서부터 근원심의 치조정 부위 중 뚜렸하게 방사선 불투과성
Ⅱ
Table 1. Gender distribution G
Ge en nd de err N Nu um mb be err % %
Male 9 64
Female 5 36
Total 14 100
Ji-Young Lee et al: Treatment of implant that have exposed threads during second surgery. Implantology 2009
original article
이 관찰되는 부위까지의 높이를 수직으로 골높이를 측정하였 으며 근원심의 높이를 구하여 그 평균을 계산하였다. 방사선 사진 상 각 임프란트의 높이를 측정하여 확대율을 고려하여 변연골 흡수량을 계산하였다. 그리고 1차 수술 후 골흡수량과 보철 기능 후의 골 흡수량의 차이를 비교하여 기술 하였다.
이차 수술 시 임프란트의 각 부위별 노출량은 수술 시 피판 거상 후 치주 프루브(periodontal probe)를 사용하여 협,설, 근, 원심측에서 측정하였다.
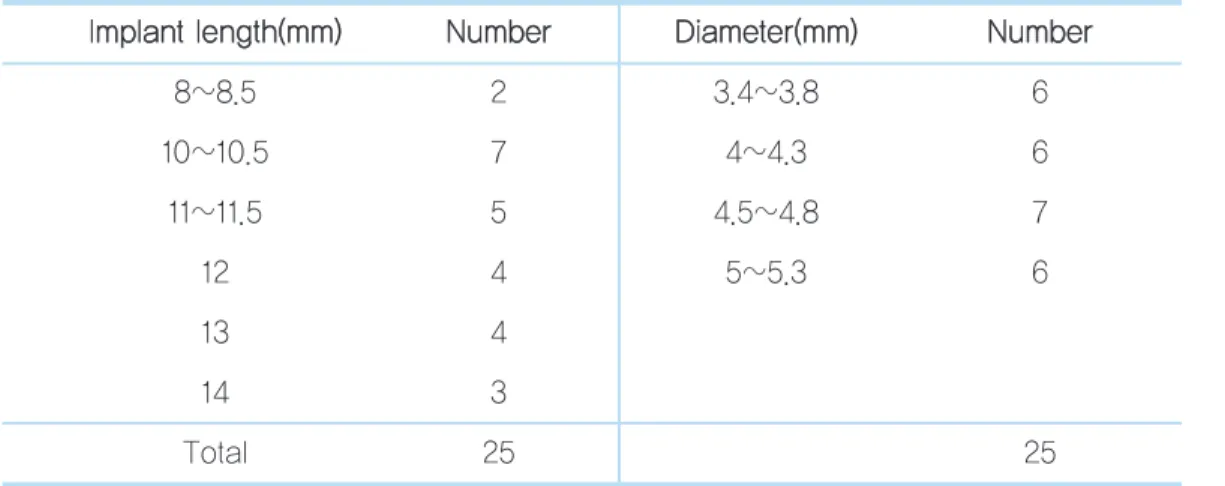
사용된 임프란트 종류 및 직경과 길이는 Table 4, 5와 같다.
3 증례에서는 노출부위에 특별한 처치를 시행하지 않았으며 22 증례에서 노출된 부위에 골이식재를 사용하였다. 골이식 이 시행된 증례들 중 3 증례에서 흡수성 차단막이 사용되었 다. 동종골은 oragraft
Ⓡ(LifeNet,U.S.A) orthoblast
ⓇII
Ⅲ
Table 2. Age distribution A
Ag ge e N Nu um mb be err
60≤ 3
50~59 3
40~49 5
30~39 2
≤30 1
Total 14
Ji-Young Lee et al: Treatment of implant that have exposed threads during second surgery. Implantology 2009
Table 3. Type of Systemic Disease S
Sy ys stte em miic c d diis se ea as se e a an nd d s sm mo ok kiin ng g N Nu um mb be err
Hypertension 2
Hypertension+Diabetes mellitus 2
Liver disease 1
Endocrine, disease 1
Total 6
Ji-Young Lee et al: Treatment of implant that have exposed threads during second surgery. Implantology 2009
Table 5. Length and Diameter of Implant
IIm mp plla an ntt lle en ng gtth h((m mm m)) N Nu um mb be err D Diia am me ette err((m mm m)) N Nu um mb be err
8~8.5 2 3.4~3.8 6
10~10.5 7 4~4.3 6
11~11.5 5 4.5~4.8 7
12 4 5~5.3 6
13 4
14 3
Total 25 25
Ji-Young Lee et al: Treatment of implant that have exposed threads during second surgery. Implantology 2009
Implantium 14
Oneplant 2
Total 25
• GS II (Osstem, Korea), Implantium (Dentium, Korea)
• Oneplant (Warantec, Korea)
Ji-Young Lee et al: Treatment of implant that have exposed threads during second surgery. Implantology 2009
Table 6. Type of Graft Material B
Bo on ne e g grra afftt m ma atte erriia all N Nu um mb be err((IIm mp plla an ntt))
Allograft 8
Xeno 11
Xeno+Allograft 3
Total 22
• Xeno: Xenogenic bone Allo: Allogenicbone
Ji-Young Lee et al: Treatment of implant that have exposed threads during second surgery. Implantology 2009
original article
Table 7. Overview of data N
No o.. o off p pa attiie en ntt L Lo oc ca attiio on n T Th hrre ea ad d e ex xp po os su urre e B Bo on ne e g grra afftt M Me em mb brra an ne e B Bo on ne e llo os ss s P Prro os stth he es siis s
1 36 4/3/3/3 allograft . 0.5/1.1 SC
46 4/2/2/0 allograft . 0.4/0.8 SC
2 12 10/0/0/0 xenograft Bioarm 0.0/0.0 FPP
21 12/0/0/0 xenograft Bioarm 0.0/0.8 FPP
23 6/0/0/0 xenograft Bioarm 0.0/0.0 FPP
3 45 1/0/0/0 allograft . 0.0/0.8 SC
46 1/0/0/0 allograft . 0.4/0.0 SC
4 37 0/0/1/0 . . 0.0/0.8 SC
5 14 1/0/0/0 allograft . 1.7/3.0 SC
15 6/0/0/0 allograft . 0.0/0.9 SC
13 1/0/0/0 allograft . 0.0/0.0 SC
6 16 1/0/0/0 . . 0.4/0.4 SC
7 25 2/0/1/0 xenograft . 2.2/1.4 SC
26 1/0/0/0 xenograft . 1.1/0.9 SC
8 47 1/0/0/0 . . 0.6/1.0 SC
9 26 4/2/0/1 allograft . 1.2/2.6 SC
10 27 2/1/0/0 xenograft . 0.5/1.4 SC
11 25 2/0/0/0 allo+xeno . 0.4/1.4 FPP
26 5/3/2/0 allo+xeno . 0.2/0.4 FPP
27 4/2/2/0 allo+xeno . 0.4/0.4 FPP
12 46 1/0/0/0 xenograft . 0.6/0.4 SC
13 35 3/0/0/0 xenograft . 0.0/0.3 SC
36 1/0/0/0 xenograft . 0.5/0.3 SC
14 25 3/3/3/3 xenograft . 2.5/2.4 FPP
26 0/0/2/2 xenograft . 0.3/0.6 FPP
• Bone defect: Buccal/Lingual/Mesial/Distal
• Bone loss: Mesial/ Distal
• SC; single crown, FPP; fixed partial prosthesis
• Unit of data is millimeter(mm)
이종골은 BioOss
Ⓡ( Geistlich Biomaterials, german), Biocera
Ⓡ(Oscotec, korea)제품이 사용되었다(Table 6). 임 프란트 보철물은 단일 수복관이 17 증례, 부분 고정성 보철 수 복물이 8 증례였다. 2차 수술 시 평균 나사산 노출량은 협측 3.04±2.97mm, 설측 0.36±0.9mm 근심 0.64±1.11mm 원심 0.64±1.03mm 였다. 2차 수술 후 모든 증례에서 술 후 합병증은 나타나지 않았다. 보철 6개월 이후 치조골 흡수량은 최대 2.5mm에서 최소 0.0mm 로 평균 0.08 ±0.09mm로 나타났다. 모든 증례에서 관찰 기간 동안 보철물은 안정적으 로 기능하였다(Table 7).
<증례>