234
A Case of Orbital Abscess following Porous Orbital Implant Infection
Seung Woo Hong, MD, Ji-Sun Paik, MD, So-Youl Kim, MD, Suk-Woo Yang, MD
Division of Ophthalmic Plastic and Reconstructive Surgery, Department of Ophthalmology, College of Medicine The Catholic University of Korea, Seoul, Korea
Purpose: We present a case of orbital abscess following porous orbital implant infection in a 73-year-old woman with rheumatoid arthritis.
Methods: Just one month after a seemingly uncomplicated enucleation and porous polyethylene (Medpor
Ⓡ) orbital implant surgery, implant exposure developed with profuse pus discharge. The patient was unrespon- sive to implant removal and MRI confirmed the presence of an orbital pus pocket. Despite extirpation of the four rectus muscles, inflammatory granulation debridement and abscess drainage, another new pus pocket developed.
Results: After partial orbital exenteration, the wound finally healed well without any additional abscess formation.
Conclusions: A patient who has risk factors for delayed wound healing must be examined thoroughly and extreme care such as exenteration must be taken if there is persistent infection. Korean Journal of Ophthal- mology 20(4):234-237, 2006
Key Words: Porous orbital implant infection, Orbital abscess, Partial orbital exenteration
Received: August 29, 2006 Accepted: October 2, 2006
Reprint requests to Suk-Woo Yang, MD. Department of Ophthal- mology, Kangnam St. Mary’s hospital, The Catholic University Medical College of Korea, #505 Banpo-dong, Seocho-ku, Seoul 137- 807, Korea. Tel: 82-2-590-1523, Fax: 82-2-599-7405, E-mail: swyang
@catholic.ac.kr
Infected porous orbital implants are, to date, rare. When they occur, implant removal has been the only successful treatment modality.
1,2 Several cases of porous implant infection have shown that removal of the implant did not worsen the progression of orbital infection.
3,4 To our knowl- edge, this is the first reported case of orbital implant infection not controlled with implant removal.
Case Report
A 73-year-old woman presented with purulent conjunctival discharge and pain in her left, enucleated eye. She had a medical history of oral steroid intake for rheumatoid arthritis and antihypertensive medication for several years. She had an ocular history of melting necrotizing scleritis, and it was so intractable that an enucleation had been performed a month previously. After enucleation, a synthetic porous polyethylene implant (Medpor
Ⓡ, POREX Surgical Inc., USA, 20 mm in diameter) wrapped with sterilized donor sclera was used to replace orbital volume.
A culture of the eye discharge revealed Propionibacterium acne, at which time systemic and topical antibiotic medica- tion was started. Despite massive antibiotic treatment, the discharge was still seen from the conjunctival wound, and the infection continued to melt the conjunctiva and wrapping donor sclera. The Medpor
Ⓡ implant was eventually exposed a month after implantation. The patient was diagnosed with implant infection and underwent an implant removal.
The wound seemed to recover well, but two months later, purulent discharge was again seen from the wound site.
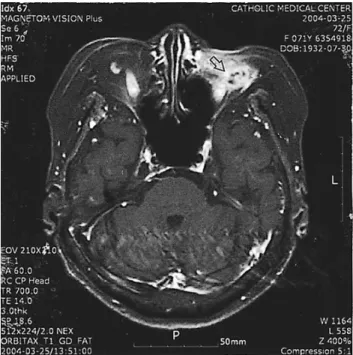
Magnetic resonance imaging of the left orbit revealed myositis of the four rectus muscles, inflammatory granula- tions, and abscesses around the orbit, especially around the optic nerve (Fig. 1). Extirpation of the four rectus muscles, removal of underlying inflammatory granulation, and abscess drainage were performed, and the wound was then soaked with betadine and antibiotic solution.
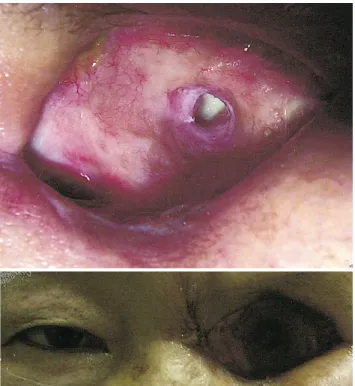
The wound recovered well, and a month after abscess excision, dermo-fat tissue harvested from the inguinal area was grafted to orbital defect site. The, graft failed to survive, and pus discharge from the wound developed once again. The graft was removed a month after implantation, but the discharge persisted (Fig. 2).
Follow-up magnetic resonance imaging two months after
removal of the dermo-fat graft showed inflammatory granula-
tions and abscess formation in the left orbit (Fig. 3). Out of
concern that the inflammation might spread to the brain, we