Introduction
The term ‘eating disorder’ includes bulimia nervosa and anorexia nervosa, and is defined as a persistent disturbance of eating behavior intended to control weight, which significantly impairs physical health or psychosocial functioning.
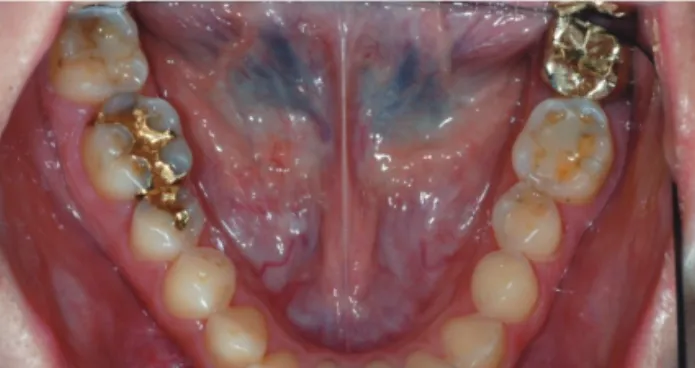
[1] This psychosomatic disease is characterized by conscious starvation, followed by a period of excessive carbohydrate intake, and then, it is often followed by deliberately induced vomiting. Although some patients’ symptoms were improved over time, a substantial proportion continues to have body-image disturbances, disordered eating, and other psychiatric difficulties.[2, 3] The greatest impacts on the oral cavity include severe lingual-occlusal tooth structure
Meng Ding, DDS
1, Sang-yoon Lee, DDS
2, Jae-Jun Ryu, DDS, PhD
1*
1
Department of Esthetic Restorative Dentistry, Graduate School of Clinical Dentistry, Korea University, Seoul, Korea.
2