INTRODUCTION
Breast cancer is a heterogeneous disease, which is characterized by a number of distinct biological entities associated with specific morphological and immunohis- tochemical features and clinical behavior.(1) Molecular and gene expression profiling studies have demonstrated that breast cancers comprise a group of tumors of several subtypes, including the luminal subtypes (hormone recep- tor-positive), the human epidermal growth factor receptor
2 (HER2)-positive, and the basal like subtype.(2) Basal-like breast cancer exhibits molecular charac- teristics that are predictive of a poor prognosis. In one previous study, intrinsic subtypes were compared with prognostic profiles in patients suffering from basal-like breast cancer, all of whom had a poor 70-gene profile, activated wound response, and high recurrence score.(3) Despite differences in the definition and prevalence of basal-like breast cancer in a variety of studies, the clinical outcomes of patients were generally poor.(4) However, no gene array profiling technique is currently clinically available, and immunohistochemical surrogate profiles for the basal-like profile have not yet been standardized or validated.(5) We utilized triple-negative breast cancers (TNBC) as a surrogate to represent the basal-like category of breast cancers because the immunostaining data were available.
Purpose: Patients with triple-negative breast cancer (TNBC) are known to carry an increased risk of distant metastasis and poor survival. The principal objective of this study was to investigate survival after brain metastases in patients with TNBC. Methods: The authors retrospectively evaluated clinical data obtained from 66 patients who had been diag- nosed with breast cancer and brain metastasis from 2003 to 2009. Estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth receptor-2 (HER2) statuses were determined via immunohistochemical staining. TNBCs were defined as those that were ER-negative, PR-negative, and HER2-negative. The time interval from initial diagnosis to brain metastasis and overall survival after brain metastasis was evaluated via the Kaplan-Meier method. Results: Twenty four (40.0%) of 60 patients were diagnosed with TNBC. The
clinicopathologic characteristics did not differ between the TNBC and non-TNBC patients. The disease-free survival durations of the TNBC and non-TNBC subjects were 17.9 and 25.6 months, respectively (p=0.135). The time intervals from initial diagnosis to brain metastasis were 25.5 and 43.7 months, respectively (p=0.027). The time intervals from distant metastasis to brain metastasis were 8.4 and 19.5 months, respectively (p=0.006). Overall survival durations from brain metastasis to death were 4.3 and 7.6 months, respectively (p=0.046). Conclusion: Patients with TNBC were more likely to develop brain metastasis earlier, and exhibit poor overall survival. Triple receptor status may be utilized as a prognostic marker for breast cancer patients with brain metastasis.
Key Words: Brain metastasis, Breast neoplasms, Triple negative
Breast Cancer
O R I G I N A L A R T I C L E
Clinical Outcomes in Patients with Triple-negative Breast Cancer and Brain Metastases
Hyuk-Chan Kwon, Sung Yong Oh, Sung-Hyun Kim
1, Suee Lee
1, Kyung A Kwon
1, Ji Hyun Lee
1, Mi Ri Lee
2, Se Heon Cho
2, Young-Jin Choi
3, Hyo-Jin Kim
1Medical Research Center for Cancer Molecular Therapy, Departments of 1Internal Medicine and 2Surgery, Dong-A University College of Medicine, Busan; 3Department of Internal Medicine, Pusan National University Hospital Medical Research Institute, Pusan National University School of Medicine, Busan, Korea
Correspondence: Hyo-Jin Kim
Department of Internal Medicine, Dong-A University College of Medicine, 3-1 Dongdaeshin-dong, Seo-gu, Busan 602-715, Korea Tel: 051-240-2951, Fax: 051-246-5044
E-mail: [email protected]
Received: October 26, 2009 Accepted: February 24, 2010 This study was supported by the Dong-A University research fund, 2007.
160
TNBC has become a commonly utilized descriptor for malignancies that estrogen receptor (ER), progesterone receptor (PR), and HER2 are all negative. TNBCs account for 10-17% of all breast carcinomas, depending on the thresholds employed to define ER and PR positivity, as well as the methods for HER2 assessment.(6) It has been well established that TNBC patients feature a relatively aggressive clinical course.(4) However, there have only been a few reports conducted thus far concerning TNBC with brain metastasis.(7-9)
The principal objective of this study was to assess clin- ical outcomes in TNBC patients with brain metastasis.
METHODS
Patients
We conducted a retrospective analysis using the medical records of patients who had been diagnosed with brain metastasis (BM) originating from breast cancer between January 2003 and January 2009. BM was diagnosed via magnetic resonance imaging (MRI) or computed tomo- graphy (CT) and/or lumbar puncture in cases in which patients evidenced symptoms such as headache, dizziness, nausea, or neurological deficits. This study was approved by the institutional review board of the Dong-A University Medical Center.
Treatment of brain metastasis
Patients with BM were treated as indicated with at least one of the following treatment modalities: whole brain radiotherapy (WBRT), surgical resection, and systemic treatments including chemotherapy and endocrine ther- apy. Corticosteroid treatment was administered after diagnosis, and continued throughout the ensuing treat- ment regimen. All patients with brain metastases were treated WBRT. The total dose was 30 Gy, applied in 10 fractions over two weeks. Intrathecal therapy for patients with leptomeningeal disease consisted of lumbar puncture or Ommaya reservoir with methotrexate 10-15 mg twice a week until malignant cells could no longer be detected in the cerebrospinal fluid.
Immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH)
Immunohistochemical analyses of ER and PR status were conducted using 4-mm sections of paraffin-embed- ded tissue specimens that were stained with monoclonal antibodies for ER (DAKO Co., Carpinteria, USA) and PR (DAKO Co.). We chose a cut-off level for negative cases of less than 10% positive nuclei with weak staining inten- sity, which is equal to Allred score 2. The tumor was considered to be HER2-positive if the primary or meta- static tumor was scored 3+ by HER2 IHC (Neo Markers, Fremont, USA), or in the case of IHC 2+ with HER2 gene amplification identified via the FISH method. TNBCs were defined as those that were ER-negative, PR-negative, and HER2-negative.
Statistical analyses
Chi-square and Fisher’s exact tests were utilized as categorical variables to compare patient characteristics among the three time period groups. A Kruskall-Wallis test was conducted in order to compare the median values of nonparametric variables. We established independent variables as follows: age at the time of diagnosis, tumor stage at primary diagnosis of breast cancer, tumor grad- ing, vessel invasion, adjuvant systemic treatment, and palliative systemic treatment.
Disease-free survival was calculated from the date of initial diagnosis to the date of first recurrence. Overall survival was calculated from the date of diagnosis of BM to the date of death or final follow-up. The interval bet- ween initial diagnosis and BM was calculated as the time from the date of initial diagnosis to the date at which BM was radiologically proven. The interval between the distant metastasis and BM was calculated as the time elapsed from the detection of the first recurrence to the radiological evidence of BM in breast cancer patients.
Survival durations were calculated via the Kaplan-Meier method. The log-rank test was employed for the com- parison of cumulative survival in the patient groups. To identify independent factors significantly related to pa- tient prognosis we used Cox’s proportional hazard analysis with a stepwise procedure. In all tests, p<0.05 was estab-
lished as the threshold of statistical significance. The SPSS software program (version 14.0; SPSS Inc., Chicago, USA) was employed in all analyses.
RESULTS
Patient characteristics
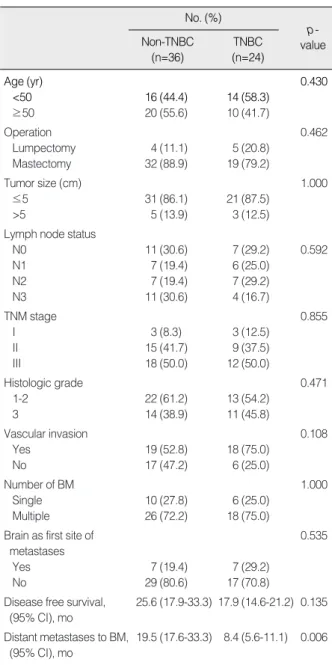
The clinical characteristics of the BM patients and the relationship with receptor status are presented in Table 1.
Twenty four patients (40.0%) were diagnosed with TNBC.
The median age at diagnosis of BM in the TNBC groups was 49 yr (range, 30-74 yr). Three patients had stage I disease at diagnosis, 9 patients had stage II, 12 patients had stage III at primary presentation. Approximately 88% of patients had T1 or T2 disease, and 70% were lymph node positive. Thirteen patients had histologic grade (HG) 1 or 2 tumors, and the others had HG 3 tumors. The most frequent presenting signs and symptoms of BM were headache, nausea, and vomiting, followed by dizziness, double vision, and unilateral weakness of the extremities.
The brain was the first site of metastasis in 7 patients (29.2%) and was accompanied, in the majority of cases, by other sites of metastatic disease. The most common sites of extracranial metastasis were the lung (60%), bone (50%), liver (45%), and the lymph nodes (45%). In 6 pa- tients (25.0%), a single BM was detected, and in 18 patients multiple parenchymal BM occurred; leptomeningeal carci- nomatosis was not observed in any of the TNBC patients.
However, the clinicopathologic parameters did not differ according to the breast cancer subtype (Table 1).
Clinical outcome according to breast cancer subtypes
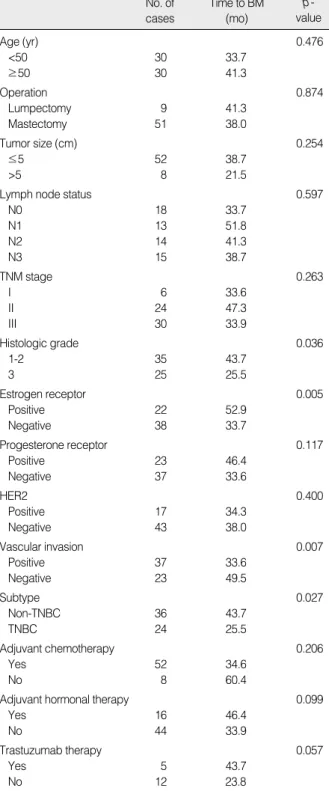
The disease-free survival durations of non-TNBC and TNBC patients were 25.6 months and 17.9 months, res- pectively (p=0.135). The median time intervals from dis- tant metastasis to BM were 19.5 months and 8.4 months, respectively (p=0.006). The median times from initial diagnoses to BM were 43.7 and 25.5 months, respectively (p=0.027; Figure 1). Primary tumor characteristics and the interval duration from initial diagnosis to BM are provided in Table 2. Histologic grade (p=0.036), ER status
(p=0.005), vascular invasion (p=0.007), subtype (p=0.027) were significantly related to the time interval from initial diagnosis to BM. However, only histologic grade was inde- pendent prognosis factor (relative risk [RR], 0.039; 95%
confidence interval [CI], 1.034-3.668; p=0.039). Among 17 HER2-positive patients, 5 received trastuzumsab treat- ment. These patients tended to exhibit a prolonged inter- val from initial diagnosis to BM (p=0.057; Table 2).
Table 1. Clinical characteristics of breast cancers with brain metastases according to subtype
No. (%)
p- value TNBC
(n=24) Non-TNBC
(n=36)
Age (yr) 0.430
<50 16 (44.4) 14 (58.3)
≥50 20 (55.6) 10 (41.7)
Operation 0.462
Lumpectomy 4 (11.1) 5 (20.8)
Mastectomy 32 (88.9) 19 (79.2)
Tumor size (cm) 1.000
≤5 31 (86.1) 21 (87.5)
>5 5 (13.9) 3 (12.5)
Lymph node status
N0 11 (30.6) 7 (29.2) 0.592
N1 7 (19.4) 6 (25.0)
N2 7 (19.4) 7 (29.2)
N3 11 (30.6) 4 (16.7)
TNM stage 0.855
I 3 (8.3) 3 (12.5)
II 15 (41.7) 9 (37.5)
III 18 (50.0) 12 (50.0)
Histologic grade 0.471
1-2 22 (61.2) 13 (54.2)
3 14 (38.9) 11 (45.8)
Vascular invasion 0.108
Yes 19 (52.8) 18 (75.0)
No 17 (47.2) 6 (25.0)
Number of BM 1.000
Single 10 (27.8) 6 (25.0)
Multiple 26 (72.2) 18 (75.0)
Brain as first site of 0.535
metastases
Yes 7 (19.4) 7 (29.2)
No 29 (80.6) 17 (70.8)
Disease free survival, 25.6 (17.9-33.3) 17.9 (14.6-21.2) 0.135 (95% CI), mo
Distant metastases to BM, 19.5 (17.6-33.3) 8.4 (5.6-11.1) 0.006 (95% CI), mo
TNBC=triple-negative breast cancer; BM=brain metastases; CI=con- fidence interval.
The median follow-up after the diagnosis of CNS metas- tasis was 21 months (range, 0.7-96 months), and the medi- an overall survival from the date of BM was 7.6 months (95% CI, 5.1-10.1 months). At 1 yr, 20% of the patients remained alive, whereas 10% were alive at 2 yr. As most patients evidenced active disease outside the brain, it was difficult to determine whether the patients died of intra- cranial or extracranial metastatic disease.
Table 3 shows overall survival according to selected patient characteristics. Patients suffering from single BM evidence longer overall survival durations (19.3 months) as compared with patients who had multiple BM (7.6 months;
p=0.021). Patients who responded to WBRT tended to
have longer overall survival durations (p=0.025). Median survival was 14.6 months in patients who received pal- liative chemotherapy versus 1.4 months for those who Table 2. Prognostic factors affecting median time from initial diagnosis to brain metastases in breast cancer
p- value Time to BM
(mo) No. of
cases
Age (yr) 0.476
<50 30 33.7
≥50 30 41.3
Operation 0.874
Lumpectomy 9 41.3
Mastectomy 51 38.0
Tumor size (cm) 0.254
≤5 52 38.7
>5 8 21.5
Lymph node status 0.597
N0 18 33.7
N1 13 51.8
N2 14 41.3
N3 15 38.7
TNM stage 0.263
I 6 33.6
II 24 47.3
III 30 33.9
Histologic grade 0.036
1-2 35 43.7
3 25 25.5
Estrogen receptor 0.005
Positive 22 52.9
Negative 38 33.7
Progesterone receptor 0.117
Positive 23 46.4
Negative 37 33.6
HER2 0.400
Positive 17 34.3
Negative 43 38.0
Vascular invasion 0.007
Positive 37 33.6
Negative 23 49.5
Subtype 0.027
Non-TNBC 36 43.7
TNBC 24 25.5
Adjuvant chemotherapy 0.206
Yes 52 34.6
No 8 60.4
Adjuvant hormonal therapy 0.099
Yes 16 46.4
No 44 33.9
Trastuzumab therapy 0.057
Yes 5 43.7
No 12 23.8
BM=brain metastases; TNBC=triple-negative breast cancer.
Proportion surviving
1.0
0.8
0.6
0.4
0.2
0.0
0.0 24.0 48.0 72.0 96.0 120.0 140.0 168.0 192.0 Months
Non-TNBC (n=36) TNBC (n=24)
Non-TNBC (n=36)
TNBC (n=24)
Figure 1. The median time intervals from initial diagnosis to brain metastases (p=0.027).
TNBC=triple-negative breast cancer.
Proportion surviving
1.0
0.8
0.6
0.4
0.2
0.0
0.0 24.0 48.0 72.0 96.0 120.0 144.0 Months
Figure 2. Overall survival from brain metastasis to death among non-triple negative and triple negative patients (p=0.046).
TNBC=triple-negative breast cancer.
did not (p<0.001). We analyzed 17 HER2-positive patients according to trastuzumab therapy. No significant differ- ence in median survival were noted after a diagnosis of BM between the tratuzumab-treated patients and the untreated patients (8.5 months vs. 7.3 months, respec- tively, p=0.579). And, overall survival from brain metas- tasis to death among non-TNBC and TNBC patients was significantly different (7.6 months and 4.3 months, res- pectively, p=0.046; Figure 2). A multivariate analysis using the Cox-regression test identified two risk factors:
no additional systemic treatment (RR, 2.714; 95% CI, 1.446-5.095; p=0.006) and TNBC (RR, 2.212; 95% CI, 1.162-4.209; p=0.016). However, number of brain metas- tases (p=0.050), and response to WBRT (p=0.387) were not independent prognostic factor for overall survival after BM.
DISCUSSION
Breast cancer is the second most common cause of brain metastases, and represents 14-20% of all such cases.(10) BM are clinically associated with a significantly detrimen- tal impact on survival. Mean survival in cases of diagnosed brain metastasis varies between 2 and 16 months. The mean 1-yr survival rate is estimated at only approximately 20%.(11) Improvements in systemic therapies have led to prolonged survival in patients with advanced breast cancer, making the issue of BM a more challenging one.
It has recently been demonstrated that gene expression profiling can be used to predict disease-free and overall survival in women with primary breast cancer, and several novel cancer subsets have previously been defined.(12) We divided the patients into two groups according to ER, PR, and HER2 expression. We observed that 24 patients (40.0%) were TNBC.
The majority of patients in this study received mul- timodality treatment, including WBRT and systemic chemotherapy and/or targeted drugs after the diagnosis of BM. These data showed that survival after a diagnosis of BM in breast cancer patients is improving. About 70%
of the patients received systemic chemotherapy after the diagnosis of BM. Patients who received systemic treatment Table 3. Prognostic factors affecting overall survival time from
brain metastases in breast cancer
p- value Median survival
(mo) No. of
cases
Age (yr) 0.995
<50 30 7.5
≥50 30 9.6
Tumor size (cm) 0.096
≤5 52 8.1
>5 8 3.0
Lymph node status 0.541
N0 18 12.6
N1 13 8.1
N2 14 7.6
N3 15 2.3
TNM stage 0.699
I 6 15.1
II 24 8.1
III 30 7.3
Histologic grade 0.585
1-2 35 7.6
3 25 8.1
Vascular invasion 0.574
Positive 37 8.1
Negative 23 7.3
Subtype 0.046
Non-TNBC 36 7.6
TNBC 24 4.3
ECOG Performance Status 0.102
0-1 25 13.6
≥2 35 4.6
Brain as first site of metastases 0.091
Yes 14 19.3
No 46 7.6
Number of BM 0.021
Single 16 19.3
Multiple 44 7.6
Resection of BM 0.085
Yes 15 9.6
No 45 7.6
Response to WBRT 0.025
CR or PR 18 19.3
SD or PD 13 7.5
Unchecked 29 4.4
Chemotherapy after WBRT <0.001
Yes 43 14.6
No 17 1.4
Trastuzumab therapy 0.579
Yes 5 8.5
No 12 7.3
TNBC=triple-negative breast cancer; ECOG=Eastern Cooperative Oncology Group; BM=brain metastases; WBRT=whole brain radio- therapy; CR=complete response; PR=partial response; SD=stable disease; PD=progressive disease.
after local treatment for brain lesion had a longer sur- vival than the patients who did not: 14.6 months vs. 1.4 months, respectively (p<0.001). This finding is consistent with previous report.(13) We also found that patients who responded to WBRT had a longer survival (19.3 months vs.
7.5 moths, p=0.025). However, about one-half of the patients did not have follow-up films, and they showed worst outcome. It can thus be assumed that many of the patients without follow-up films would have shown early progression of either brain or systemic disease. Single BM patients were better outcome than multiple number of BM (19.3 months vs. 7.6 months, p=0.021), it may be due to almost all patients with single BM received surgery followed by WBRT. However, only chemotherapy after BM was independent prognostic factor in multivariate analysis (p=0.006).
Several previous studies have demonstrated that women with TNBC are more likely to relapse, and have an asso- ciated poorer prognosis than do women suffering from non-TNBC.(3,4) However, the incidence and survival from BM in this cohort has yet to be well-defined.(7-9) We noted that, among women with TNBC, BM occurs relatively early in the natural course of the disease. The disease-free survival durations of non-TNBC and TNBC patients were 25.6 months and 17.9 months, respectively (p=0.135). The median time intervals from distant metas- tasis to BM were 19.5 months and 8.4 months, respectively (p=0.006). The median times from initial diagnosis to BM were 43.7 and 25.5 months, respectively (p=0.027).
These findings are consistent with a previously published report in which TNBC brain metastases were shown to develop earlier than in other receptor subtypes, occurring a median 22 months after primary diagnosis, versus 51 months for all other subtypes.(14)
Recent studies have assessed survival outcomes follow- ing the development of BM in patients with TNBC. Hines et al.(8) reported that 22% of patients had TNBC associ- ated with a median survival of 7 months (range, 0-20 months) after a diagnosis of BM. Dawood et al.(9) reported that 37.3% had TN disease associated with a median sur- vival of 2.9 months. In this study also showed that the overall survival duration from BM to death was shorter in
the TNBC patients than in the non-TNBC disease group (7.6 months vs. 4.3 months, respectively, p=0.046). In multivariate analysis TNBC was correlated poor overall survival (p=0.016).
TNBC has been recognized as a unique cancer subtype characterized by aggressive behavior and requiring a relatively aggressive therapeutic approach when compared with other breast cancer subtypes. As there is currently no role for hormonal or HER2-targeted agents in this regard, chemotherapy is currently the primary therapy for triple-negative breast cancer.(6) From a biological perspective, DNA-damaging agents (such as platinum agents) are of a high priority, owing to the relevance of the BRCA1 pathway and DNA repair dysfunction in this subtype, which may confer enhanced sensitivity to DNA- damaging agents.(15) In vitro, basal-like breast cancer cell lines are more sensitive to EGFR inhibitors than are luminal cell lines, and synergy with a combination of carboplatin and cetuximab has been reported.(16) Recently, two results of platinum-plus-cetuximab-based regimens as a pretreatment for TNBC have been reported. Cetuxi- mab and carboplatin treatment of TNBC patients yielded an 18% partial response and a 27% clinical benefit,(17) whereas a carboplatin-plus-irinotecan-and-cetuximab- treated group evidenced a 39% response with severe tox- icities.(18)
The association with BRCA1 pathway dysfunction in TNBC patients raises the possibility that poly (ADP-ribose) polymerase (PARP) inhibitors may prove to have some efficacy.(19) One previous report asserted that ASD2281, a PARP inhibitor, exerted few adverse effects and evi- denced activity in cancer associated with the BRCA1 or BRCA2 mutations.(20) Therefore, well-designed clinical trials with TN breast caner patients with BM using these agents will be necessary to improve clinical outcomes.
Our study has several limitations. First, in our analyses, we included only patients with complete information on ER, PR, and HER2 status available. This introduced some selection bias. Secondary, our small sample size probably contributed to limited power and imprecise effect esti- mates. Additionally, this was also a retrospective study, and lacked detailed molecular profiling and a hierarchical
cluster analysis of the tissue. However, the results of this study do appear to support the proposition that patients with TNBC with BM have poorer outcomes than non-TN cases, and require novel treatments for the prevention or treatment of BM.
CONCLUSION
Patients with TNBC have a shorter time to development of brain metastases, and show shorter survival durations after a diagnosis of brain metastases, than do non-TNBC patients. Triple receptor status could be useful in predict- ing survival in breast cancer patients with brain metas- tasis. Further clinical trials are needed to prevent BM using novel agents in TNBC patients.
REFERENCES
1. Simpson PT, Reis-Filho JS, Gale T, Lakhani SR. Molecular evolution of breast cancer. J Pathol 2005;205:248-54.
2. Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature 2000;406:
747-52.
3. Fan C, Oh DS, Wessels L, Weigelt B, Nuyten DS, Nobel AB, et al.
Concordance among gene-expression-based predictors for breast cancer. N Engl J Med 2006;355:560-9.
4. Rakha EA, Reis-Filho JS, Ellis IO. Basal-like breast cancer: a critical review. J Clin Oncol 2008;26:2568-81.
5. Nielsen TO, Hsu FD, Jensen K, Cheang M, Karaca G, Hu Z, et al.
Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res 2004;10:
5367-74.
6. Reis-Filho JS, Tutt AN. Triple negative tumours: a critical review.
Histopathology 2008;52:108-18.
7. Lin NU, Claus E, Sohl J, Razzak AR, Arnaout A, Winer EP. Sites of distant recurrence and clinical outcomes in patients with metastatic triple-negative breast cancer: high incidence of central nervous system metastases. Cancer 2008;113:2638-45.
8. Hines SL, Vallow LA, Tan WW, McNeil RB, Perez EA, Jain A. Cli- nical outcomes after a diagnosis of brain metastases in patients with estrogen- and/or human epidermal growth factor receptor 2-positive versus triple-negative breast cancer. Ann Oncol 2008;19:1561-5.
9. Dawood S, Broglio K, Esteva FJ, Yang W, Kau SW, Islam R, et al.
Survival among women with triple receptor-negative breast cancer and brain metastases. Ann Oncol 2009;20:621-7.
10. Lin NU, Bellon JR, Winer EP. CNS metastases in breast cancer. J Clin Oncol 2004;22:3608-17.
11. Shaffrey ME, Mut M, Asher AL, Burri SH, Chahlavi A, Chang SM, et al. Brain metastases. Curr Probl Surg 2004;41:665-741.
12. Ahr A, Karn T, Solbach C, Seiter T, Strebhardt K, Holtrich U, et al.
Identification of high risk breast-cancer patients by gene expression profiling. Lancet 2002;359:131-2.
13. Fromm S, Bartsch R, Rudas M, de Vries A, Wenzel C, Steger GG, et al. Factors influencing the time to development of brain metastases in breast cancer. Breast 2008;17:512-6.
14. Heitz F, Harter P, Lueck HJ, Fissler-Eckhoff A, Lorenz-Salehi F, Scheil-Bertram S, et al. Triple-negative and HER2-overexpressing breast cancers exhibit an elevated risk and an earlier occurrence of cerebral metastases. Eur J Cancer 2009;45:2792-8.
15. Taniguchi T, Tischkowitz M, Ameziane N, Hodgson SV, Mathew CG, Joenje H, et al. Disruption of the Fanconi anemia-BRCA path- way in cisplatin-sensitive ovarian tumors. Nat Med 2003;9:568-74.
16. Hoadley KA, Weigman VJ, Fan C, Sawyer LR, He X, Troester MA, et al. EGFR associated expression profiles vary with breast tumor subtype. BMC Genomics 2007;8:258.
17. Carey LA, Rugo HS, Marcom PK, Irvin W, Ferraro M, Burrows E, et al. TBCRC001: EGFR inhibition with cetuximab added to carbo- platin in metastatic triple-negative (basal-like) breast cancer. J Clin Oncol 2008;26. abstract #1009.
18. O’Shaughnessy J, Weckstein DJ, Vukelja SJ, Mclntyre K, Krekow L, Holmes FA, et al. Preliminary results of a randomized phase II study of weekly irinotecan/carboplatin with or without cetuximab in patients with metastatic breast cancer. Breast Cancer Res Treat 2007;
106. abstract #308.
19. Ashworth A. A synthetic lethal therapeutic approach: poly (ADP) ribose polymerase inhibitors for the treatment of cancers deficient in DNA double-strand break repair. J Clin Oncol 2008;26:3785-90.
20. Fong PC, Boss DS, Yap TA, Tutt A, Wu P, Mergui-Roelvink M, et al. Inhibition of poly (ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl J Med 2009;361:123-34.